
Abstract
The objective of this research was to determine the antimicrobial resistance of bacteria isolated from items related to hygiene and antisepsis, equipment, and instruments used in different hospital wards. Bacterial isolation and identification, phenotypic antimicrobial susceptibility assays, mecA gene detection, and multiple antimicrobial resistance index analysis were performed. In total, 105 bacteria were isolated from 138 items. Of these, 49.52% bacteria were collected from instruments, 43.80% from equipment, and 6.66% from items related to hygiene and antisepsis. All gram-positive bacteria (88 isolates) were identified as coagulase-negative Staphylococcus. Five species of gram-negative bacilli (17 isolates) were isolated, and the prevalence of Enterobacter agglomerans (29.41%), Escherichia coli (11.76%), and Serratia liquefaciens (11.76%) was high. Antimicrobial resistance was reported for 93.33% of the isolates. Gram-positive bacteria were resistant to sulfazotrim (88.64%) and penicillin (82.95%), while gram-negative bacteria showed resistance to sulfazotrim (70.59%) and ampicillin (64.71%). Analysis of multiple antibiotic resistance index showed that 73.33% of the isolates were a high risk to public health. The mecA gene was detected in 23 (71.88%) isolates. The evaluation of microorganisms isolated in the hospital environment revealed their high multidrug resistance index. Thus our study presses the need to pay more attention to the cleanliness of frequently used instruments, which may be potential sources of infections.
Introduction
Nosocomial infections are acquired in hospital environments, which may serve as a reservoir and source of transmission of different pathogens.1,2 Nosocomial infections have become a global public health problem. Epidemiological data reveal long hospitalization periods as the main reason underlying the rise in morbidity and mortality. 2
The term “hospital infection” has been recently replaced with “healthcare-related infection (HCRI)” owing to the emergence of multidrug-resistant bacteria that are associated with the indiscriminate use of antimicrobial agents. This may lead to an increase in bacterial resistance, resulting in unnecessary expenses for patients, as well as hospitals. 3 For instance, patients hospitalized in intensive care units (ICUs) are highly susceptible to HCRI, as they are administered high doses of antibiotics for prolonged durations that frequently increase their length of hospital stay. 4
According to the World Health Organization (WHO), the rational use of antimicrobials indicates the use of the right drug, at the right dose, and at an affordable price.5,6 However, the consumption of these drugs is high in clinical practice (human and animal), thus contributing to the development of antimicrobial resistance.6,7
Different microorganisms contaminate the hospital environment and contribute to HCRI. At present, oxacillin-resistant Staphylococcus aureus, 8 vancomycin-resistant Enterococcus sp., 9 enterobacteria producing extended-spectrum β-lactamase (ESBL), 10 and carbapenem-resistant Acinetobacter baumannii 11 are the main pathogens detected in hospital environments.
Microorganisms that remain viable on inanimate surfaces represent a low risk of infection transmission but favor indirect contamination upon contact with equipment, instruments, or more frequently the hands of health care professionals. Therefore, all materials used in hospitals may serve as potential risk factors to patients; hence, the cleanliness and hygienic handling of these materials are imperative to reduce incidences of HCRI.11–13
This study aimed to determine the antimicrobial resistance of bacteria isolated from instruments, equipment, and items related to hygiene and antisepsis used in different sectors of a hospital in the Northwest region of the state of Paraná, Brazil.
Materials and Methods
Ethical aspects
The study received authorization for research under the condition of confidentiality of the hospital's identity. This research was carried out with environmental materials and equipment, without the need for approval by the ethics committee, only permission from the management of the respective hospital.
Study site and sampling
From July to August 2018, samples from instruments, equipment, and items related to hygiene and antisepsis from different sectors of a hospital in the Northwest region of Paraná were aseptically collected using sterile swabs containing Aimes+charcoal medium (Copan Transystem, Italy). After sample collection, the swabs were stored at 4°C and immediately sent to the Laboratory of Veterinary and Preventive Medicine and Public Health of the Graduate Program in Animal Science with Emphasis on Bioactive Products of the Paranaense University (UNIPAR).
Sampling sites
Samples (listed below) were collected from the items in the following sectors: emergency room, infirmary, pediatric room, ICU, surgical center (where elective semicritical surgeries and emergency critical surgeries are performed), private wards, and health coverage agreement facilities.
Instruments
Samples from stethoscopes (olive and diaphragm), sphygmomanometers (cuff), and thermometers were collected from the emergency room, infirmary, pediatric room, ICU, private wards, and health coverage agreement facilities.
Equipment
Samples were collected from surgical rooms (in critical and semicritical sectors), furniture, appliances, and equipment such as anesthesia carts, O2 aspirators, exit cannula, surgical tables, anesthetic tables, spotlight (lateral handles), cardiac monitors (buttons), warmed cribs, portable vacuums, intensifier (on and off button), and electrocautery (on and off button). The surgical center also has an exclusive pharmacy, in which samples were collected from the medicine drawers (handles), suture drawers (handles), countertops, refrigerator (handle and rubber sealing), and cabinets. In addition, samples were obtained from fixed first-aid stretchers, runner stretchers, and wheelchairs in the corridor.
Items related to hygiene and antisepsis
Samples were obtained from dispensers for antiseptics, chlorhexidine, and degerming solution, as well as from taps (manual), wash basins (tub and wall), sinks for dumping organic material (walls) from semicritical sectors, and orthopedic chutes (hose) from critical sectors.
Bacterial isolation
The swabs were individually introduced into tubes containing 3 mL of Brain Heart Infusion (BHI) medium and incubated at 37°C for 24 hr. The obtained cultures were streaked on MacConkey agar and blood agar plates and incubated at 37°C for 24 hr to isolate gram-positive and gram-negative aerobic bacteria. The prominent colonies on each plate were isolated, spiked in BHI medium, and incubated at 37°C for 24 hr. The cultures were then stored in 10% glycerol at −20°C.
Identification of isolates
Each isolate was subjected to phenotypic characterization by Gram staining and biochemical tests. Catalase-positive gram-positive cocci were subjected to a coagulase test to classify them as coagulase-positive or coagulase-negative Staphylococcus (SCN). The biochemical identification of bacteria belonging to Enterobacteriaceae was carried out using a set of biochemical tests included in the “Enterobacteria Kit” (NewProv®, Paraná, Brazil), as per the manufacturer's recommendations. 14
Antibiogram
Antimicrobial susceptibility testing was performed by the agar-diffusion method according to the criteria established by the Brazilian Committee on Antimicrobial Susceptibility Testing (BrCAST). 15 Isolated colonies were seeded in BHI medium overnight. On the day of the experiment, the bacterial inoculum was standardized according to the McFarland 0.5 scale, and the bacterial suspension was inoculated onto Mueller Hinton agar plates using swabs. Antimicrobial-impregnated discs were subsequently placed, and the plates were incubated at 37°C for 18–24 hr. Inhibition zones were measured (mm), and the results obtained were recorded. The positive control used included the standard American Type Culture Collection (ATCC) strains, S. aureus 25923 and Escherichia coli 25922.
The susceptibility of gram-negative bacteria was tested against the following antibiotics: nalidixic acid (30 μg), amikacin (30 μg), amoxicillin (10 μg), amoxicillin+clavulanate (30 μg), ampicillin (10 μg), aztreonam (30 μg), ceftiofur (30 μg), ceftazidime (30 μg), ceftriaxone (30 μg), ciprofloxacin (5 μg), chloramphenicol (30 μg), enrofloxacin (30 μg), cefepime (30 μg), cefotaxime (30 μg), cefoxitin (30 μg), ertapenem (10 μg), gentamicin (10 μg), imipenem (10 μg), meropenem (10 μg), sulfazotrim (25 μg), tetracycline (30 μg), and tobramycin (10 μg).
The antibiotics tested against gram-positive bacteria were as follows: amoxicillin+clavulanate (30 μg), ampicillin (10 μg), cephalothin (30 μg), cefotaxime (30 μg), clindamycin (2 μg), enrofloxacin (5 μg), gentamicin (10 μg), norfloxacin (10 μg), oxacillin (1 μg), penicillin (30 μg), sulfazotrim (25 μg), tetracycline (30 μg), and vancomycin (30 μg).
Phenotypic detection of ESBL-producing enterobacteria
The phenotypic testing of ESBL-producing enterobacteria was performed by the double-disc synergistic test using cefotaxime (30 μg), ceftazidime (30 μg), ceftriaxone (30 μg), and aztreonam (30 μg). The discs were distributed at a distance of 20 mm from a disc containing amoxycillin+clavulanate (20/10 μg). Any increase or distortion in the zone of inhibition of one of the antibiotics toward the amoxicillin+clavulanate disc was suggestive of ESBL production. 16
The positive control used was an isolate from the bacteriological library of the Laboratory of Veterinary and Preventive Medicine and Public Health of the Graduate Program in Animal Science with Emphasis on Bioactive Products, Paranaense University (UNIPAR).
Index of multiple antimicrobial resistance
Multidrug resistance was detected by defining the multiple antimicrobial resistance (MAR) index as a/b, where a is the number of antimicrobials for which isolates were resistant, and b is the number of antimicrobials to which isolates were exposed. Values above 0.2 represent samples that pose a high risk to public health. 17
Detection of mecA gene
Staphylococcus isolates that (through antibiogram) were classified as resistant to oxacillin (including intermediate resistance) were tested for the presence of the mecA gene. 18 DNA was extracted using the PureLink Genomic DNA Kit (Invitrogen), as per the manufacturer's instructions. Polymerase chain reaction (PCR) comprised 0.5 μL of mecA1 primer (AAAATCGATGGTAAAGGTTGG) and 0.5 μL of mecA2 primer (AGTTCTGCAGTACCGGATTTG) (5 μM), 20 μL Platinum PCR SuperMix (Invitrogen), 2 μL DNA, and 2 μL free-nuclease water (total volume 25 μL). Amplification was carried out using a Thermo brand Px2 Thermal Cycler under the following conditions: 94°C for 5 min, followed by 40 cycles of 94°C for 30 sec, 57°C for 30 sec, and 72°C for 1 min, and a final extension at 72°C for 5 min. 18 S. aureus ATCC 33591 was used as the positive control, and S. aureus ATCC 25923 served as the negative control.
Amplified products were visualized by GelRed staining of the electrophoresed gel (Uniscience); products were detected as a single band of 533 bp.
Results
A total of 138 samples were collected from 27 instruments (52.17%), 50 pieces of equipment (36.23%), and 16 items related to hygiene and antisepsis (11.59%). From these samples, 105 bacteria were isolated. Of these, 52 (49.52%) bacteria were collected from instruments, 46 (43.80%) from equipment, and 7 (6.66%) from items related to hygiene and antisepsis.
Of the 105 isolates, 88 (83.81%) were classified as gram-positive bacteria and 17 (16.19%) were grouped as gram-negative bacteria. Gram-negative bacteria were isolated from all categories of hospital items except for items related to hygiene and antisepsis.
With respect to bacterial identification, 100% of gram-positive bacteria were SCN. Five species of gram-negative bacilli were detected, and Enterobacter agglomerans (29.41%), E. coli (11.76%), and Serratia liquefaciens (11.76%) showed high prevalence. In addition, 35.29% of gram-negative bacteria were nonfermenting gram-negative bacilli (NFGNB). We were unable to perform bacterial classification using our identification kit (Fig. 1).
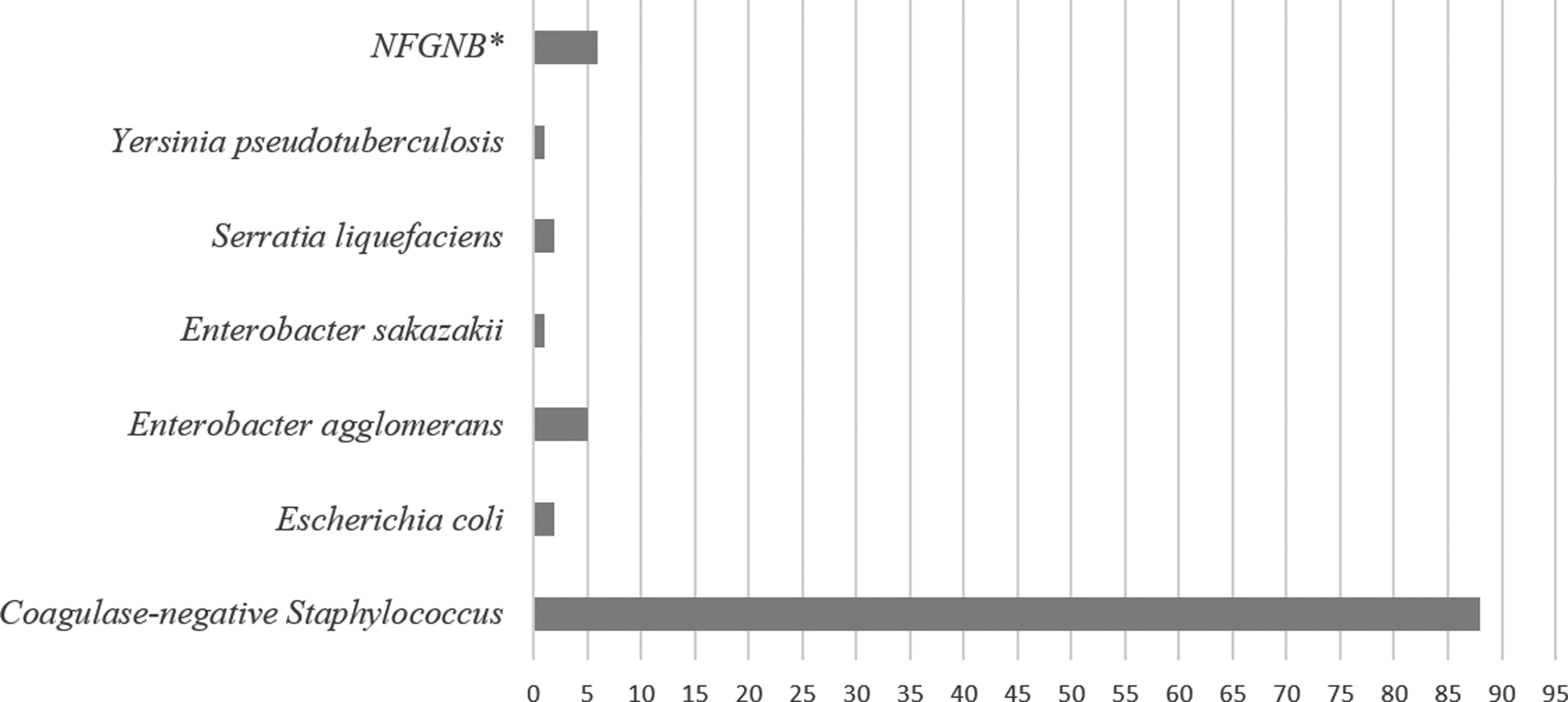
Absolute (N) frequency of bacterial isolates from instruments, equipments, and items related to hygiene and antisepsis from a hospital in the Northwest region of the state of Paraná, Brazil, in 2018. *Non-fermenting gram-negative bacilli.
Antimicrobial resistance was detected for 98 (93.33%) isolates. Gram-positive bacteria showed maximum resistance to the following antimicrobials: sulfazotrim (88.64%), penicillin (82.95%), ampicillin (80.68%), norfloxacin (37.50), clindamycin (36.36%), and oxacillin (36.36%). Microorganisms isolated from instruments, equipment, and items of hygiene and antisepsis were found to be resistant to sulfazotrim; all samples were sensitive to vancomycin (Table 1).
Resistance Profile of Gram-Positive Bacterial Isolates from Instruments, Equipment, and Hygiene and Antiseptic Items of a Hospital in the Northwest Region of the State of Paraná, Brazil, in 2018
R, resistant.
The isolated gram-negative bacteria were most resistant to sulfazotrim (70.59%), ampicillin (64.71%), amoxicillin (58.82%), chlorhexidine (47.06%), nalidixic acid (41.18%), and cefoxitin (52.94%). All gram-negative bacteria isolated from instruments were resistant to amoxicillin, ampicillin, and sulfazotrim, while the bacteria isolated from equipment showed maximum resistance against chloramphenicol (54.55%), sulfazotrim (54.55%), and ampicillin (45.45%) (Table 2).
Resistance Profile of Gram-Negative Bacterial Isolates from Instruments, Equipment, and Hygiene and Antisepsis Items of a Hospital in the Northwest Region of the State of Paraná, Brazil, in 2018
R, resistant; %, percentage.
In the double-disc synergistic test, none of the samples was found to produce ESBL, as evident from the absence in the distortion of the inhibition halos between the antimicrobial discs and the amoxicillin+clavulanate disc.
Evaluation of the MAR index showed that 70 gram-positive and 7 (41.18%) gram-negative isolates, representing 73.33% of all isolates, imposed a high risk to public health.
Figure 2 shows the origin of bacteria that were resistant to more than 50% of the tested antimicrobials; most of these bacteria (84.6%) were isolated from medical instruments such as stethoscopes (olive and diaphragm), thermometer, and sphygmomanometer (cuff) from different hospital sectors.
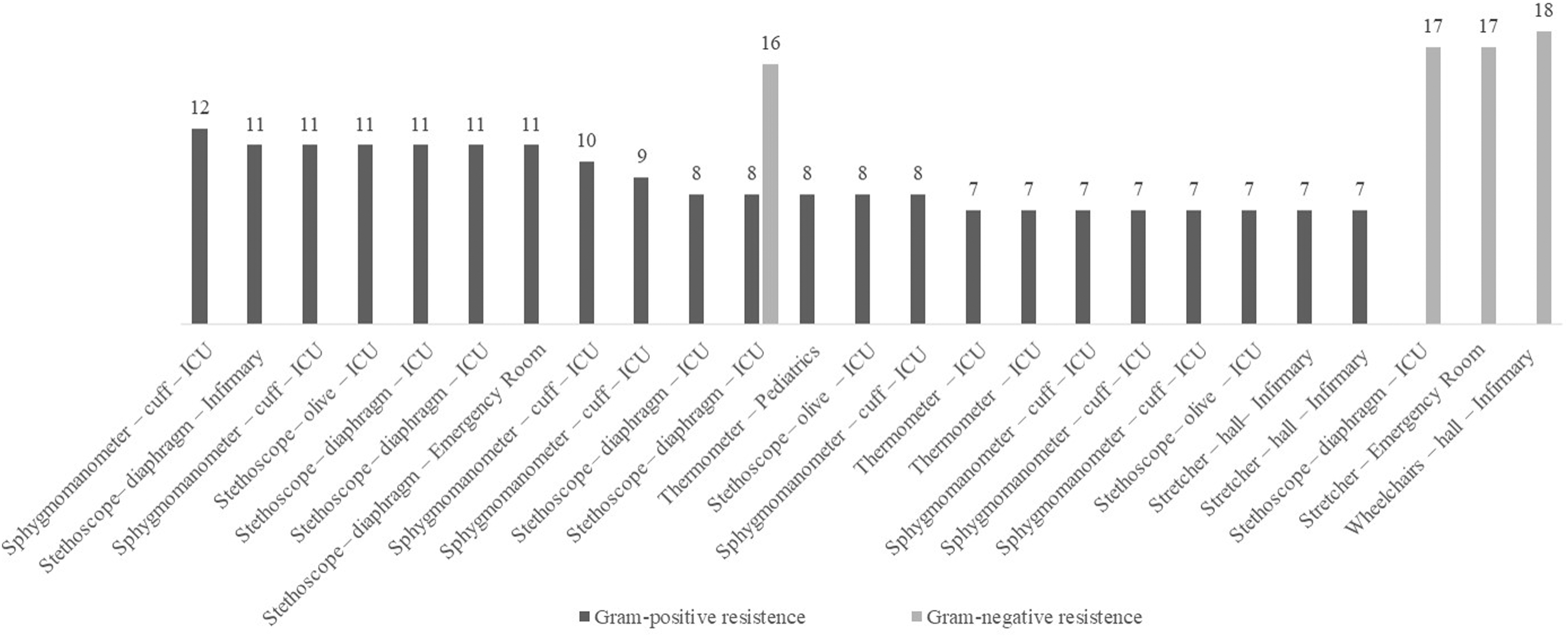
Origin of bacteria resistant to more than 50% of the antimicrobials tested per group (gram-positive and gram-negative bacteria) from environmental samples from a hospital in the Northwest region of the state of Paraná, Brazil, 2018.
The expression of mecA was detected in 23 (71.88%) of SCN, 21 of which were resistant to oxacillin and 2 showed intermediate resistance in the disc diffusion method (Fig. 3).

PCR assay for the mecA gene in isolates of Staphylococcus spp. from environmental samples from a hospital in the Northwest region of the state of Paraná, Brazil, 2018. Two percent agarose gel. LADDER, molecular marker; NC, negative control (ATCC 43300); PC, positive control (ATCC 25923). ATCC, American Type Culture Collection; PCR, polymerase chain reaction.
Discussion
Information on the microorganisms existing in the hospital environment may allow monitoring of infections and assessment of infection prevention practices. Efforts have been directed toward patient care, but the persistence of fungi and bacteria in materials used in health care facilities may contribute to increased frequency and severity of infection cases.
In the present study, 105 bacteria were isolated from 138 samples. Among the isolates, SCN was found to be predominant in 83.81% of the instruments (52.27%), equipment (39.77%), and items related to hygiene and antisepsis (7.95%). Nwankwo 19 evaluated the presence of microorganisms on forceps, scissors, floor, walls, suction tubes, sinks, and headboards of operating rooms and found SCN to be the most frequently isolated bacteria (28.3%). 19 A study evaluating ICU records and medical records prepared by nurses found SCN to be the most common contaminant (ca. 40%), demonstrating that record-keeping documents can also be a potential source of infection. 20
The predominance of SCN in hospital environments is understandable, as it is a part of the normal human microbiota. However, SCN has been recognized as a pathogen owing to its association with medical devices such as catheters, 21 relative virulence, high-level antibiotic resistance, and biofilm formation capacity. These properties allow SCN to colonize biotic and abiotic surfaces, 22 making it a typical opportunistic pathogen. The skin and mucous membrane are the main entry sources for bacteria causing endogenous infections that are transmitted by medical and/or nursing procedures. 22
The predominance of NFGNB, E. agglomerans, E. coli, and S. liquefaciens, among gram-negative bacteria was verified. The overall frequency of NFGNB was 35.29%; this approximates the values reported by Deliberali et al. 23 in a prospective analysis of hospitalized patients in Porto Alegre, Rio Grande do Sul. These authors found Pseudomonas aeruginosa (65.03%), A. baumannii (16.56%), and Stenotrophomonas maltophilia (9.5%) as the most prevalent species. 23 The involvement of this group of opportunistic bacteria was also investigated in infectious processes at a hospital in Campina Grande, Paraíba, in which the frequency was 15% over a period of 2 years. Nosocomial infections are known to be frequently caused by NFGNB that mainly affect immunocompromised patients or individuals who have undergone invasive procedures. 3
E. coli and species of Serratia and Enterobacter have been frequently detected as the causative agents of nosocomial infections.24–26 Bacteria belonging to Enterobacteriaceae are one of the main agents of infection in hospital environments. Some of these isolates show multiresistance antimicrobial profiles, carbapenemase production, or ESBL.27,28
The identification of a large number of SCN isolates and gram-negative bacilli in the materials used in hospitals confirms the importance of our findings because the Patient Safety and Quality in Health Services Bulletin classified a very similar microorganism profile as an etiological agent of central venous catheter-associated primary bloodstream infections in adult, pediatric, and neonatal ICUs. 29 The bacteria isolated from hospital environments were found to be associated with microbial infections in patients; therefore, it is important to assess the cleaning quality in hospital environments and to train medical professionals for controlling HCRI. 30
Antimicrobial resistance is a global public health issue, and the inappropriate use of antibiotics has aggravated the situation, imposing a tremendous challenge to treat such infections. Antimicrobial resistance was found in 93.33% of samples; sulfazotrim and beta-lactam drugs were among the antibiotics with the highest resistance. During the analysis of floors and surfaces at a hospital in Juiz de Fora, Minas Gerais, 69% of SCN isolates were oxacillin and penicillin resistant and 25% were sulfazotrim resistant. 31 Mahl and Rossi 32 evaluated the antimicrobial resistance of bacteria isolated from hospital mattresses and found that over 50% SCN and Enterobacter sp. were resistant to sulfazotrim, oxacillin, penicillin G, and ampicillin. 32
The inappropriate and excessive use of antibiotics has exerted a selective pressure on bacteria and contributed to the emergence of highly resistant strains. Resistance occurs in response to the reduction in the effectiveness of an antibiotic against the tested pathogen. Bacteria can use different mechanisms such as antibiotic inactivation, target change, mutation, and horizontal gene transfer to develop antimicrobial resistance. 33
Sulfonamides are cheap and efficient antibiotics and their use has been limited owing to the increase in the number of resistant microorganisms. Sulfonamides act on folic acid synthesis, specifically on the enzyme dihydropteroate synthase (DHPS), which is important in prokaryotes. However, some pathogens have developed mutations that render DHPS insensitive to sulfonamides. 34 In contrast, β-lactams are known to inhibit peptidoglycan synthesis, which leads to cell lysis. The production of beta-lactamase enzymes such as penicillinases, ESBL, cephalosporinase type AmpC, and carbapenemases that hydrolyze beta-lactam antibiotics is the main hurdle for the use of these drugs. As microorganisms are constantly adapting to the changing environment, new therapeutic approaches should be developed to address this issue that is associated with huge economic repercussions, increased hospitalization rates, increased lengths of ICU stay, and high mortality rates.35,36
The MAR index is a calculation developed by Krumperman 17 to express the risk associated with samples; MAR index indicates whether a sample is derived from an environment frequently exposed to antibiotics. 17 In our study, 79.55% SCN and 41.18% gram-negative isolates showed an MAR index of over 0.2 (high risk). Our results were corroborated by the reports from other authors who have shown that 62.90% of gram-negative effluent and air isolates from hospital environments have an MAR index >0.237 and that 52.6% of gram-positive and gram-negative isolates from infected wounds show an MAR index over 0.2. 38 Hospital infections and contamination of these places may be associated with cross contamination between hospitals, between patients and hospitals, and even between the hospital and the environment. 37
We failed to detect any strain producing ESBL, and none of the isolated Staphylococcus species was resistant to vancomycin. Only three isolates were resistant to ertapenem (one of the carbapenems tested). However, 32 SCN were resistant to oxacillin, and the mecA gene was detected in 71.88% samples, including the samples with intermediate resistance. Phenotypic and genotypic resistance was found to be predominant in the isolates collected from instruments such as thermometers, stethoscopes, and sphygmomanometers.
In a hospital in Rio de Janeiro, evaluation of laboratory coats, stethoscopes, and doorknobs showed that 84.7% Staphylococcus isolates were resistant to oxacillin. 39 Teixeira et al. 40 found 87.5% S. aureus isolates from stethoscopes to be resistant to methicillin. Stethoscopes and sphygmomanometers used in ICUs and surgical wards were found to be sources of transmission of oxacillin-resistant bacteria. 41 In addition, methicillin-resistant Staphylococcus spp. have been reported on hands and in nostrils of health care professionals,42,43 reinforcing the potential role of cross contamination as the vehicle for infection. There is great concern about the risk of dissemination of resistant bacteria and the transfer of resistance genes.
Conclusion
The evaluation of microorganisms present on items used in a hospital revealed the high antimicrobial resistance among the isolated bacterial strains. A large percentage of these microorganisms showed multiresistance. As these bacteria were isolated from inanimate objects, the findings of our study are alarming to understand the importance of correct and periodic maintenance of cleanliness and sterility of objects and environments in contact with patients. Such measures would reduce the risk of the spread of these bacteria. As it is impossible to keep these materials totally free of biological contamination, training health care personnel, hospital cleaning, correct execution of basic preventive measures, and monitoring microbial load on instruments such as stethoscopes, thermometers, and sphygmomanometers are highly recommended.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
To the University of Paraná-UNIPAR and the Araucária Foundation's Basic and Applied Research Program for the funding granted to this research, the National Council for Scientific and Technological Development, and the Coordination for the Improvement of Higher Education Personnel for granting the Support Program school fee to the Postgraduate of Private Education Institutions and Scholarship of the National Postdoctoral Program.