
Abstract
Background:
Surveillance of antimicrobial resistance (AMR) requires an international approach with national and local strategies. Our aim was to summarize a retrospective 10-year report of antibiotic resistance of gram-positive and gram-negative bacteria in Mexico.
Methods:
A total of 46 centers from 22 states of Mexico participated. Databases of AMR from January 2009 to December 2018 were included for most species. The 10-year period was divided into five 2-year periods.
Results:
For Staphylococcus aureus, a decrease in resistance in all specimens was observed for erythromycin and oxacillin (p < 0.0001 for each). For Enterobacter spp., resistance to meropenem increased for urine specimens (p = 0.0042). For Klebsiella spp., increased drug resistance in specimens collected from blood was observed for trimethoprim/sulfamethoxazole, gentamicin, tobramycin (p < 0.0001 for each), meropenem (p = 0.0014), and aztreonam (p = 0.0030). For Acinetobacter baumannii complex, high drug resistance was detected for almost all antibiotics, including carbapenems, except for tobramycin, which showed decreased resistance for urine, respiratory, and blood isolates (p < 0.0001 for each), and for amikacin, which showed a decrease in resistance in urine specimens (p = 0.0002). An increase in resistance to cefepime was found for urine, respiratory, and blood specimens (p < 0.0001 for each). For Pseudomonas aeruginosa, aztreonam resistance increased for isolates recovered from blood (p = 0.0001).
Conclusion:
This laboratory-based surveillance of antibiotic resistance shows that resistance is increasing for some antibiotics in different bacterial species in Mexico and highlights the need for continuous monitoring of antibiotic resistance.
Introduction
Antimicrobial resistance (AMR
AMR surveillance requires an international approach with national and local strategies. 3 In 2018, the Mexican government published an agreement declaring the compulsory nature of the National Strategy of Action Against Resistance to Antimicrobials. 4 In Mexico, the drug resistance rates of some bacterial pathogens—both gram-positive and gram-negative—are available.5–14 However, these rates except for the SIREVA/GIVEBPVac group (Grupo Interinstitucional para la Vigilancia de Enfermedades Bacterianas Prevenibles por Vacunación, in Spanish) 15 that monitors AMR for Streptococcus pneumoniae, the rest are derived from isolated efforts, so hardly reflect the nationwide perspective of drug resistance.
For the surveillance of AMR, core data are generated by microbiology laboratories that routinely identify and determine the drug susceptibility of bacterial species isolated from clinical specimens. As a result, in addition to patient-specific results, this information about AMR can be grouped, analyzed over time, and monitored to identify changes.
Two years ago, a nongovernmental initiative launched the Network for Research and Surveillance of Drug Resistance (Red Temática de Investigación y Vigilancia de la Farmacorresistencia [INVIFAR] in Spanish) in Mexico. One focus of this network is the surveillance of resistance in common pathogens, including Enterococcus spp., Staphylococcus aureus, Escherichia coli, Klebsiella spp., Enterobacter spp., Salmonella spp., Shigella spp., Acinetobacter baumannii complex, Pseudomonas aeruginosa, and Stenotrophomonas maltophilia, and in collaboration with SIREVA/GIVEBPVac, S. pneumoniae. As part of this network's work, this article summarizes a retrospective 10-year report of AMR of gram-positive and gram-negative bacteria in Mexico.
Materials and Methods
Participating centers
Centers participating in the network were invited to voluntarily provide relevant data, including the number of beds, the capacity of the intensive care unit (ICU), the population served, and the methods used in the microbiology laboratory for identification and susceptibility tests. A total of 46 centers from the network agreed to participate, including 38 hospital-based laboratories and 8 external laboratories. In each center, strains were recovered and identified using conventional methods available. Of the 46 centers, 41 laboratories used commercial systems: 21 used VITEK 2 (Biomérieux, Marcy l’ Etoile, France); 10, Phoenix (Becton-Dickinson, Sparks, MD); 5, MicroScan WalkAway (Siemens Health care Diagnostics, West Sacramento, CA); and 5, Sensititre (TREK Diagnostic Systems, Inc., Cleveland, OH). The remaining five laboratories used biochemical tests for identification and the disk diffusion method for susceptibility.
Data collection and analysis
Databases from each hospital were collected by the coordinating center, and all the results were examined using the laboratory-based WHONET 5.6 program. All data were carefully reviewed by a medical microbiologist. Only one isolate per patient was included and only isolates collected from clinical isolates were included. The results were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) criteria (2018). 16
Clinical isolates collected from January 2009 to December 2018 were included for most species. Clinical specimens were screened for the AMR distribution of Enterococcus spp., S. aureus, S. pneumoniae, E. coli, Klebsiella spp., Enterobacter spp., Salmonella spp., Shigella spp., A. baumannii complex, P. aeruginosa, and S. maltophilia. Only isolates from clinically relevant specimens were included, such as urine, respiratory, blood, cerebrospinal fluid (CSF), and feces. For respiratory samples, only tracheal aspirates and bronchial lavages were included.
For S. pneumoniae, antimicrobial susceptibility was determined by the broth microdilution method according to the CLSI 2018 recommendations and interpretative criteria. S. pneumoniae ATCC 49619 was used as the control strain. This work was performed with the collaborative work with the SIREVA/GIVEBPVac network. 15
The conversion of the file to the WHONET format was done using the BacLink 2 tool, and all converted databases were deposited into the WHONET platform. All WHONET files from each center were aggregated and analyzed. Macros, including the species type, date of collection, and specimens, were used to facilitate the revision.
Statistical analyses
Differences in percentages of antibiotic resistance between the first and last period were assessed using a chi-squared test using the p < 0.05 criterion for statistical significance. Statistical testing was performed with the SPSS software, version 20.0 (IBM SPSS, Chicago, IL).
Ethics statement
The hospital ethics committee (Comité de Ética en Investigación del Antiguo Hospital Civil de Guadalajara “Fray Antonio Alcalde,” Jalisco, Mexico) approved this study with reference number 129/17. Informed consent was deemed not necessary by the ethics committee because no intervention was involved. The data and isolates for the study were deidentified so that these were irretrievably unlinked to an identifiable person.
Results
Characteristics of the participating laboratories and data received
In this 10-year study, the centers were distributed across 22/32 Mexican states. Characteristics of the participating hospitals are shown in Table 1. One of the hospitals provided data from only its ICU. Initially, a total of 273,893 strains were included for analysis. After eliminating duplicate isolates, information from 165,939 isolates was included for analysis. Drug resistance rates were calculated and are shown in Figs. 1–3. The number of isolates varied according to the study period, specimen, and antibiotic, and is shown in Supplementary Table S1.

Distribution of drug resistance among gram-positive species. The y axis represents the percentages or resistance.
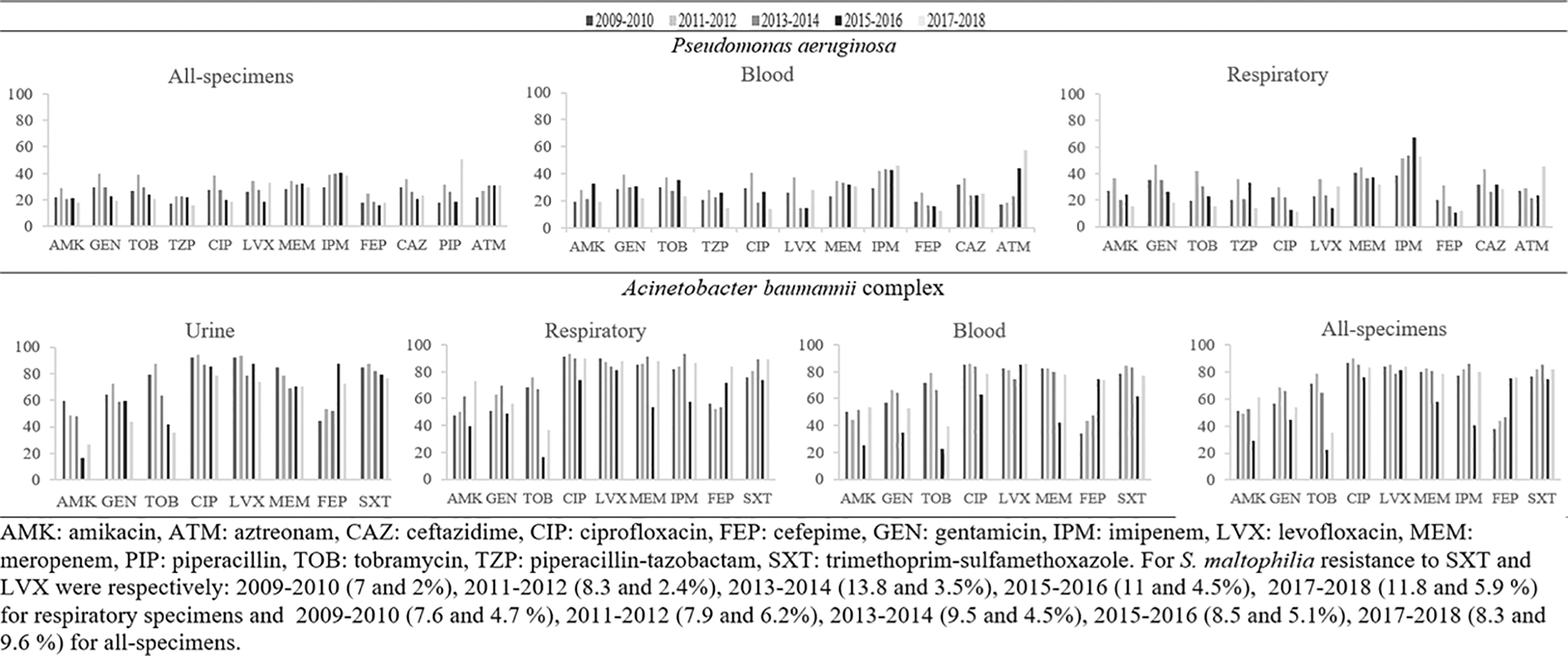
Distribution of drug resistance among gram-negative nonfermenter species. The y axis represents the percentages or resistance.
Characteristics of Hospitals Participating in the 10-Year Review of Drug Resistance
Univ, university; Gen, general; Spe, specialties; M&Ch, mother and child; Ped, pediatrics; Ad, adults; Pu, public; Pr, private; ND, no data.
The 10-year period was divided into five 2-year periods. Because some centers did not report data for the entire 10-year period, all those that provided data for at least 1 year before December 31, 2018, were included, and the available data for each 2-year period were combined. The number of centers participating for each period was as follows: 2009–2010, 6 centers; 2010–2012, 10 centers; 2013–2014, 18 centers; 2015–2016, 27 centers, and 2017–2018, 46 centers. For this reason, the first periods (2009–2010 and 2011–2012) are overrepresented by some centers.
Gram-positive bacteria
Enterococcus faecalis isolates collected from urine, blood, and all specimens (specimens where the pathogen may be considered the causative agent of disease) during the last four periods were analyzed (Fig. 1). High resistance to tetracycline was observed in blood and all specimens (>65%). For vancomycin and linezolid, percentages of resistance were lower than 5% in most cases. Nitrofurantoin remains an adequate alternative for urine infections (Fig. 1).
For Enterococcus faecium, resistance to nitrofurantoin decreased in urine (p < 0.0001), while resistance to penicillin increased in blood (p = 0.0335) and all specimens (p < 0.0001). Linezolid resistance was identified as lower than 4%.
For S. aureus, low percentages of drug resistance were detected for trimethoprim/sulfamethoxazole (SXT), linezolid, rifampicin, and gentamicin. A decrease in drug resistance in all specimens was observed for erythromycin (from 66.8% to 40.3%, p < 0.0001) and for oxacillin (from 44.5% to 26.2%, p < 0.0001), indicating a trend toward higher susceptibility rates among S. aureus clinical isolates. No resistance was detected for vancomycin.
For S. pneumoniae, several specific sites of isolation were analyzed, including respiratory specimens, sterile fluids, and CSF-only specimens. When only respiratory specimens (tracheal aspirates and bronchial lavages) were included, the frequency of penicillin (p = 0.0045) and cefotaxime (p = 0.0003) resistance decreased. No resistance to vancomycin was detected. No other significant differences were detected.
Gram negatives
For E. coli, resistance to ampicillin was up to 100% (Fig. 2). In general, high frequency of resistance to fluoroquinolones and other aminoglycosides (tobramycin and gentamicin) was observed. Resistance to cephalosporins was higher than 30% for all specimens. Resistance to carbapenems remained low (up to 2.8%). In general, no significant changes were observed in these periods.

Distribution of drug resistance among Enterobacteriaceae species. The y axis represents the percentages or resistance.
For Enterobacter spp., resistance to amikacin and cefepime remained low, whereas resistance to meropenem increased for urine specimens (p = 0.0042).
For Klebsiella spp., resistance to SXT, gentamicin, ceftazidime, tobramycin (p = 0.0001 for each), meropenem (p = 0.0014), and aztreonam (p = 0.0030) increased in specimens collected from blood. In addition, increased gentamicin resistance was also observed for isolates collected from respiratory-related specimens (p < 0.0001).
For Klebsiella spp. isolated from urine samples, increased resistance was detected for aztreonam, gentamicin, and ceftazidime (p < 0.0001 for each). When isolates collected from all specimens were included, increased resistance was detected for aztreonam, tobramycin, SXT, gentamicin (p < 0.0001 for each), and cefuroxime (p = 0.0002).
For Salmonella spp. (not Typhi), resistance to ciprofloxacin, and SXT decreased for specimens collected from any site (p = 0.0035). For Shigella spp., high resistance to SXT and ampicillin was detected during the entire study period.
For A. baumannii complex, high drug resistance was observed for almost all antibiotics throughout the study period, except for tobramycin, for which resistance decreased for all, urine, respiratory, and blood isolates (p < 0.0001 for each), and for amikacin, for which resistance decreased in urine specimens (p = 0.0002).
In addition, an increase in resistance to cefepime was found (up to 83.6%) for all specimens, urine, respiratory, and blood (p < 0.0001 for each). Carbapenem resistance remained steadily high.
For P. aeruginosa, aztreonam resistance increased for isolates recovered from blood (p = 0.0001) and for all specimens (p = 0.0108) (Fig. 3).
For S. maltophilia, levofloxacin resistance slightly increased for isolates from all specimens (p = 0.0280), reaching up to 9.6% in the last study period (2017–2018).
Discussion
In this study, a decrease in drug resistance was observed for oxacillin in S. aureus (from ∼50% to 25%), indicating a lower prevalence of methicillin-resistant S. aureus (MRSA) isolates. Since 2005, S. aureus infections have reportedly decreased by 43% overall, with a 55% decrease in MRSA (p < 0.001) and a 66% decrease in hospital-acquired MRSA infections in the United States. 17 According to the Centers for Disease Control and Prevention (CDC), the reduction in MRSA bloodstream infections stagnated between 2012 and 2016; from 2016 to 2017, these infections reduced by only 8%. 18 The decrease in MRSA infections has been attributed to the disappearance of the predominant MRSA ST239 clones in some populations. 14 Recently, MRSA clinical isolates from the prevalent clonal complex 5 MRSA from different regions in Mexico were analyzed in a multinational collaborative phylogenetic study. 19 A major feature of the study was that Mexican MRSA isolates belonged to a divergent subclade of CC5-II, subclade CC5-II-A, which evolved from the United States around the late 1990s. This subclade was further subdivided into ST5-II and ST1011 subclades that showed a geographical structure by region within Mexico: ST5-II was from central and western Mexico and ST1011 was from central and northern Mexico. The MRSA strains are characterized by AMR to ciprofloxacin, erythromycin, clindamycin, and penicillin and high sensitivity to fusidic acid, mupirocin, rifampin, and tetracycline. It should be mentioned that these strains were exclusively MRSA.
For S. pneumoniae, almost half of the strains showed erythromycin resistance, as has been shown in similar studies. 20 When only respiratory isolates were included, the frequency of penicillin and cefotaxime resistance decreased. Furthermore, an increase in resistance was detected for erythromycin in CSF specimens, but the difference did not reach significance (p = 0.0600). This result should encourage clinicians to use β-lactams for the treatment of pneumococcal pneumonia in children and adults. The two most important factors for changes in antibiotic resistance for pneumococci are the introduction of conjugate vaccines and the prescription of antimicrobials in the community, mainly for the treatment of upper respiratory tract infections. It has been demonstrated that 46.4% of serotype 19A strains are resistant to penicillin. Differences observed among respiratory and CSF isolates may be explained by the relationship between serotype 19A and penicillin- and macrolide-resistant isolates. This serotype is an important cause of some cases of invasive and noninvasive diseases in Mexico, as shown by the SIREVA/GIVEBPVac network. 21
E. coli has alarming resistance values for β-lactams. In our previous report of only 6 months (first semester of 2018), we detected resistance to β-lactams nearing 50%. 22 A previous meta-analysis showed a frequency of extended-spectrum β-lactamase producing E. coli of 42.4%, with an overall multidrug resistance prevalence of 22%. 23
For Enterobacter spp., an increase in resistance to meropenem was observed for isolates collected from urine. Carbapenemases that belong to the New Delhi metallo-β-lactamase (NDM), Verona integron-encoded metallo- β-lactamase (VIM), K. pneumoniae carbapenemase (KPC), or class D-lactamases (OXA-48 like) have been identified in the Klebsiella aerogenes and Enterobacter cloacae complex. 24 We have no data of the mechanisms related to carbapenem resistance or the genes encoding these carbapenemases. However, it is essential to consider the relevance of the genes that may be involved in carbapenem resistance in these species, especially because KPC and NDM are related to more severe infections.25,26
For Klebsiella spp., resistance to SXT, gentamicin, ceftazidime, tobramycin (p = 0.0001 for each), meropenem (p = 0.0014), and aztreonam (p = 0.0030) increased in specimens collected from blood. In addition, increased gentamicin resistance was also observed for isolates collected from respiratory-related specimens (p < 0.0001).
For Klebsiella spp., meropenem resistance increased in isolates collected from blood. Carbapenem resistance is of concern because it is frequently associated with KPC in this bacterial genus.25,26,13,27
For Salmonella spp., a decrease in resistance to ciprofloxacin (from 16.7% to 6.1%) and SXT (from 50% to 15.7%) was observed for specimens collected from any site. Our previous report showed a 17.4% resistance rate to ciprofloxacin. A previous report showed no resistance to this antibiotic, but the isolates analyzed were both from animal and human specimens. 28
For Shigella spp., high resistance to SXT (higher than 68%) was detected throughout the study period. In our previous study, the analysis of 28 isolates of Shigella spp. revealed resistance rates of 37.5%. In the present study, a larger number of isolates were analyzed, and this may explain this difference. A previous report in 2013 showed resistance percentages to SXT of 58%, 29 which are more in agreement with these results.
Several therapeutic challenges exist with P. aeruginosa due to the limited effective treatment strategies and the reports of increased carbapenem resistance worldwide, with a prevalence up to 88%.30–33 Our findings show that resistance to carbapenems has remained stable during the last decade, with percentages ranging from 27.9% to 29.4%.
The most frequently associated enzymes to carbapenem resistance caused by carbapenemases in P. aeruginosa are from class B, with higher morbidity and mortality rates in bloodstream infections. 34 In our study, no data of associated genes were collected. However, the increased aztreonam resistance detected for isolates from blood may suggest the presence of class A enzymes (maybe KPC or GES) and not class B enzymes, at least not as a unique mechanism.
SXT and levofloxacin are the most common antibiotics used to treat infections associated with S. maltophilia, 35 with a report of nonsusceptibility from 75.5% to 65.6% over the 10-year period (ending in 2008). In our study, a slight rise in levofloxacin resistance was observed in respiratory specimens (from 2% to 5.9%) with a resistance for all specimens in the last study period (2017–2018) up to 9.6%. Our results reinforce the need for surveillance of AMR to control antibiotic overuse.
High drug resistance was detected for almost all antibiotics for the A. baumannii complex, with carbapenem resistance remaining steadily high and an alarming increase in cefepime resistance (up to 83.6%). The A. baumannii complex remains a high multidrug-resistant organism that has been reported in Mexico.36–38
The strengths of this retrospective analysis system include the comprehensive geographical coverage, the large number of centers that participated (including both hospital and nonhospital centers), and the large amount of data collected.
We acknowledge some weaknesses in our study, including incomplete data collection (because reports were voluntarily), and variation in laboratory test methods and antibiotics included. Furthermore, the lack of information for some antibiotics such as tigecycline and daptomycin, as well as the absence of confirmation of linezolid resistance, limits the full comprehension of some of the results.
Given that each center obtained different antibiotic profiles for each strain, and some centers provided information for some antibiotics and others did not, we included all the information reliable given the number of isolates tested for certain antibiotics in at least three 2-year periods.
In conclusion, this laboratory-based surveillance of AMR shows that resistance to some antibiotics is increasing in different bacterial species in Mexico. Our study highlights the need for continuous monitoring of AMR by local and national strategies.
Footnotes
Acknowledgments
This study is the result of the work of the Network for the Research and Surveillance of Drug Resistance (INVIFAR by the acronym in Spanish), which at present includes 72 centers from 27 out of 32 states of Mexico and the SIREVA/GIVEBPVac group (Grupo Interinstitucional para la Vigilancia de Enfermedades Bacterianas Prevenibles por Vacunación, in Spanish). We thank Andrea López -Gamboa and Myriam A. Zamora-Márquez for technical assistance in the preparation of tables and figures.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.