
Abstract
Background:
The aim of this study was to investigate the characteristics of carbapenem-resistant Klebsiella pneumoniae (CRKP) ST76 isolates collected during an outbreak in a hospital's intensive care unit and neurosurgery unit.
Methods:
Seventeen separate clinical isolates of CRKP were collected from patients from March 2016 to February 2017. Bacterial isolates were identified, and antimicrobial susceptibility testing was conducted using the VITEK-2 compact system. Isolates containing antibiotic resistance genes were characterized by polymerase chain reaction and DNA sequencing. Clonal relatedness was assessed by multilocus sequence typing and pulsed-field gel electrophoresis. Conjugation experiments were performed to determine the transferability of plasmids with antibiotic resistance. The genomic features and mobile genetic elements of ST76 CRKP were detected by whole genome sequencing.
Results:
ST76 KPC-2–producing CRKP prevailed in our hospital, causing an outbreak. The strains also carried blaSHV-1, blaCTX-M-15, blaTEM-1, qnrB, and acc(6′)Ib-cr resistance genes. Plasmids from 17.7% of the isolated strains bearing these resistance genes could be transferred into the recipient Escherichia coli J53 through conjugation. Sequencing results showed that the KP4 genome mainly consisted of a circular chromosome and three antibiotic resistance plasmids. The plasmid carrying the blaKPC-2 gene was located on a 437 kb IncFIB (pQil) plasmid with Tn1721-blaKPC-2-ΔT3 gene structure. Genes conferring resistance against aminoglycosides, quinolones, fluoroquinolones, beta-lactamase, phenicols, sulfonamides, and trimethoprims and the presence of virulence-associated genes related to iron acquisition or adhesins were determined.
Conclusion:
This is the first report of the whole genome sequence of a KPC-2–producing K. pneumoniae ST76 isolate. This work provides a basis for understanding antibiotic resistance and resistant plasmid transmission. Relevant departments should implement infection control and prevention measures to reduce the incidence of nosocomial infections.
Introduction
In recent years, carbapenem-resistant Klebsiella pneumoniae (CRKP) has been widely spread around the world. Infections with CRKP are characterized by high drug resistance, high mortality, easy transmission, and difficulty of treatment. As a result, CRKP has attracted considerable research and clinical interest. The resistance mechanisms of CRKP include the following components: the production of drug resistance enzymes such as extended-spectrum beta-lactamase (ESBL), carbapenemase, active efflux of bacteria, changes in bacterial outer membrane proteins, and the production of integrons that lead to the transfer of drug resistance genes through plasmids, transposons, insertion sequences, etc. The production of drug-resistant enzymes is the most important mechanism of resistance with relevance to the current study. Studies have shown that the carbapenemase carried by K. pneumoniae primarily includes class A (blaKPC-2, blaKPC-3), class B (blaNDM-1, blaNDM-5, blaIMP-1, blaIMP-4, blaVIM-1, blaVIM-2, blaSIM-1), and class D (blaOXA-48) proteins, where ∼71.0% to 95.3% of isolated strains produce the blaKPC gene the most common resistance gene among isolates in Asia.1–3 In this time since the blaKPC gene was discovered in the United States in 1996, it has rapidly spread across the globe. 4 Many countries, including Italy, Germany, Greece, Israel, Brazil, Mexico, South Korea, China, and Japan, have reported blaKPC-carrying isolates of CRKP. 5 Unsurprisingly, most outbreaks are relatively small scale. Multilocus sequence analysis has shown that there are several high-risk clones of CRKP carrying the blaKPC gene, notably ST258 in North America, Latin America, and Europe, and ST11 in Asia, and these strains have been the focus of considerable research. 6 However, there are still outbreaks of high-risk clonal populations such as ST76 about which little is known of its transmission mechanism, and reports of drug resistance gene are limited.
In this study, we report an outbreak of a CRKP ST76 isolate carrying the blaKPC-2 gene between the intensive care unit (ICU) and neurosurgery unit and explore its mechanisms of drug resistance and transmission. Whole-genome sequencing of ST76 CRKP was carried out to provide evidence to guide clinical anti-infective treatment and control of drug-resistant bacterial transmission.
Materials and Methods
Bacterial isolation and clinical information
Seventeen nonduplicate sequential strains of CRKP were collected from various types of specimens from patients in the ICU and neurosurgery unit at the 1,980-bed First Affiliated Hospital of Jiamusi University in Heilongjiang Province, northeast China, from March 2016 to February 2017. The ICU has 15 beds, neurosurgery unit has 50 beds, and the neurosurgery ICU has 6 beds, a total of 71 beds. These isolates were identified as CRKP strains by the VITEK-2 compact system (bioMérieux). Quality control strains (Escherichia coli ATCC 25922, Salmonella ser. Braenderup H9812, and E. coli J53) were used to confirm antimicrobial activity, as well as pulsed-field gel electrophoresis (PFGE), and conjugation experiments. Patient information was manually extracted from medical records. This study was approved by the Ethics Committee of the First Affiliated Hospital of Jiamusi University (2018025). The ethics committee determined that consent was not needed, as this study was retrospective and participants' identities were anonymized.
Antimicrobial susceptibility testing
The VITEK-2 compact system was used for antimicrobial susceptibility testing, and the results were interpreted according to the 2016 Clinical and Laboratory Standard Institute Guidelines. The minimal inhibitory concentrations (MICs) of imipenem, meropenem, and levofloxacin were determined using an Etest strip, and ertapenem resistance was determined by disc diffusion.
Detection of antibiotic resistance genes
The DNA was extracted from each strain of CRKP using the boiling method. Resistance genes were detected by polymerase chain reaction (PCR), including carbapenemase genes (blaKPC, blaNDM, blaIMP-4, blaIMP-8, blaVIM-1, blaVIM-2, blaOXA-23, blaOXA-24, and blaOXA-48), ESBL genes (blaSHV, blaTEM, blaCTX-M-1, and blaCTX-M-9), AmpC beta-lactamase enzyme (blaDHA and blaACC), and quinolone resistance genes (qnrA, qnrB, qnrS, qepA, and acc(6′)Ib-cr). Positive amplification products were sequenced, and the sequencing results were compared by BLAST.
Multilocus sequence typing and PFGE
Seventeen CRKP strains were assessed for clonal diversity by multilocus sequence typing (MLST) and PFGE. MLST was performed by amplifying seven housekeeping genes (gapA, infB, mdh, pgi, phoE, rpoB, and tonB) expressed by K. pneumoniae according to the protocol at Institute Pasteur MLST database. * Genomic DNA from 17 CRKP strains was prepared in agarose plugs and digested with the restriction enzyme XbaI for 3 hr at 37°C. The digested fragments were separated on a 1% pulsed-field certified agarose using the Bio-Rad CHEF Mapper System under the following conditions: temperature of 14°C, voltage of 6 V/cm, run time of 18 hr, and a switch time of 5–35 sec. The band patterns were analyzed using BioNumerics Software. PFGE patterns were identified according to the protocol at the Centers for Disease Control and Prevention (CDC) website.
Conjugation experiments
The transfer of antibiotic resistance genes was tested using a conjugation test in which E. coli J53 (sodium azide resistant) was used as the recipient strain and 17 CRKP isolates were used as the donor strains. Each isolate was inoculated along with the recipient strain into Luria-Bertani agar at a ratio of 1:3, and the mixtures were incubated for 24 hr at 35°C. Transconjugants were selected on Luria-Bertani broth containing sodium azide (100 μg/mL) and imipenem (1 μg/mL). The transconjugant strains were identified by PCR and sequencing. The MICs for imipenem and cephalosporins were measured using the VITEK-2 compact system.
Whole genome sequencing
KP4 genomic DNA was extracted from overnight cultures using a DNA Mini Kit (Qiagen, Hilden, Germany). The Illumina HiSeq 2000 system (Illumina, Inc., San Diego, CA), which generates 150-bp paired-end sequences, and the PacBio system (Pacific Biosciences, Menlo Park, CA), which assembles a 10-kb fragment library, were used with SOAPdenovo (ver 2.04). The genomic sequences were annotated using the Prokka 1.12 program. The expression of rRNA and tRNA was predicted using Barrnap 0.4.2 and tRNAscan-SE (ver 1.3.1) software, respectively, and bacterial gene expression was predicted using Glimmer 3.02 software. The annotated information for the predicted genes was obtained using BLAST aligned with the NRGene, EggNOG, and GO Databases. The PlasmidFinder Database and BLASTn were used to identify the incompatible groups. The antimicrobial resistance genes and virulence genes were identified after uploading the assembled genome to ResFinder and the Virulence Factor Database (VFDB). The KP4 genomic sequence was deposited at GenBank under accession no. SAMN10995707.
Results
Clinical characteristics of CRKP isolates
The clinical details of patients are shown in Fig. 1. The 17 CRKP isolates were identified in a diverse population of ICU and neurosurgery unit patients from March 2016 to February 2017. They were isolated from the respiratory tract (n = 14) and blood (n = 3). Patients were typically older, with only three patients younger than 50. Patients were admitted for various reasons, including 11 cases of cerebral hemorrhage, 4 cases of brain injury and trauma due to car accidents and falling objects, and 1 case each for intracranial lesion and intestinal obstruction. Among these, 70.6% of patients had surgery, 76.5% had tracheotomy and mechanical ventilation, and all patients received antibiotic treatment, catheterization, and arteriovenous catheterization. Hospital admissions were typically long, and the average admission time was 25.9 days. The mortality rate was 35.3%.
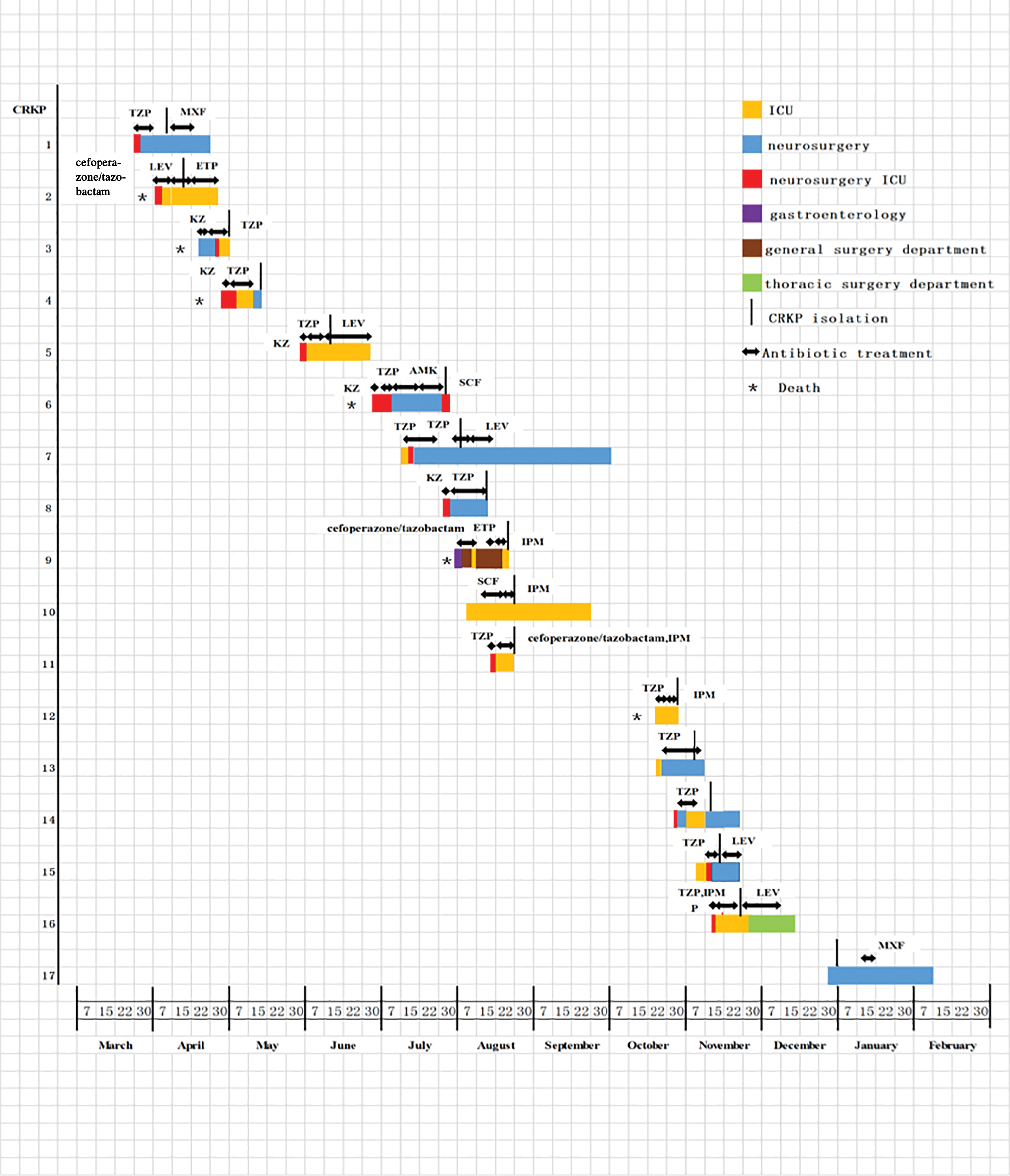
Epidemiology of the CRKP outbreak cases. AMK, amikacin; CRKP, carbapenem–resistant Klebsiella pneumoniae; ETP, ertapenem; IMP, imipenem; KZ, cefazolin; LEV, levofloxacin; MXF, moxifloxacin; SCF, cefoperazone/sulbactam; TZP, piperacillin/tazobactam. Color images are available online.
Antimicrobial susceptibility and resistance genes
All isolates were resistant to ampicillin–sulbactam, piperacillin/tazobactam, cefazolin, ceftriaxone, aztreonam, and imipenem, and all were susceptible to amikacin. There were varying rates of resistance against different antimicrobials: ceftazidime (94.1%, n = 16), gentamicin (94.1%, n = 16), cefepime (47.1%, n = 8), ciprofloxacin (17.7%, n = 3), and levofloxacin (17.7%, n = 3). The resistance genes found in at least 16 of the 17 (>94%) CRKP isolates included blaKPC (100%, n = 17), blaSHV-1 (100%, n = 17), blaCTX-M-15 (100%, n = 17), qnrB (100%, n = 17), blaTEM-1 (94.1%, n = 16), and acc(6′)Ib-cr (94.1%, n = 16). However, 5.9% (n = 1) of isolates produced qnrS. The resistance genes blaNDM, blaIMP-4, blaIMP-8, blaVIM-1, blaVIM-2, blaOXA-23, blaOXA-24, blaOXA-48, blaDHA, blaACC, qnrA, and qepA were not detected. These results are shown in Table 1.
Clinical Characteristics, Antimicrobial Susceptibilities, and Drug Resistance Genes of 17 Carbapenem-Resistant Klebsiella pneumoniae Isolates
AMK, amikacin; AMS, ampicillin–sulbactam; ATM, aztreonam; CAZ, ceftazidime; CIP, ciprofloxacin; CRO, ceftriaxone; ETP, ertapenem; FEP, cefepime; GEN, gentamicin; IMP, imipenem; KZ, cefazolin; LEV, levofloxacin; MIC, minimal inhibitory concentration; MLST, multilocus sequence typing; PFGE, pulsed-field gel electrophoresis; TZP, piperacillin/tazobactam.
Homology analysis
MLST analysis of 7 housekeeping genes of K. pneumoniae showed that 17 CRKP isolates belonged to the ST76 strain. According to a cutoff of 85% genetic similarity, all 17 CRKP isolates, of which 8 were obtained from the ICU and 9 were from neurosurgery unit, belonged to ST76 and shared the same PFGE pattern (Fig. 2), suggesting that they were clonally related.
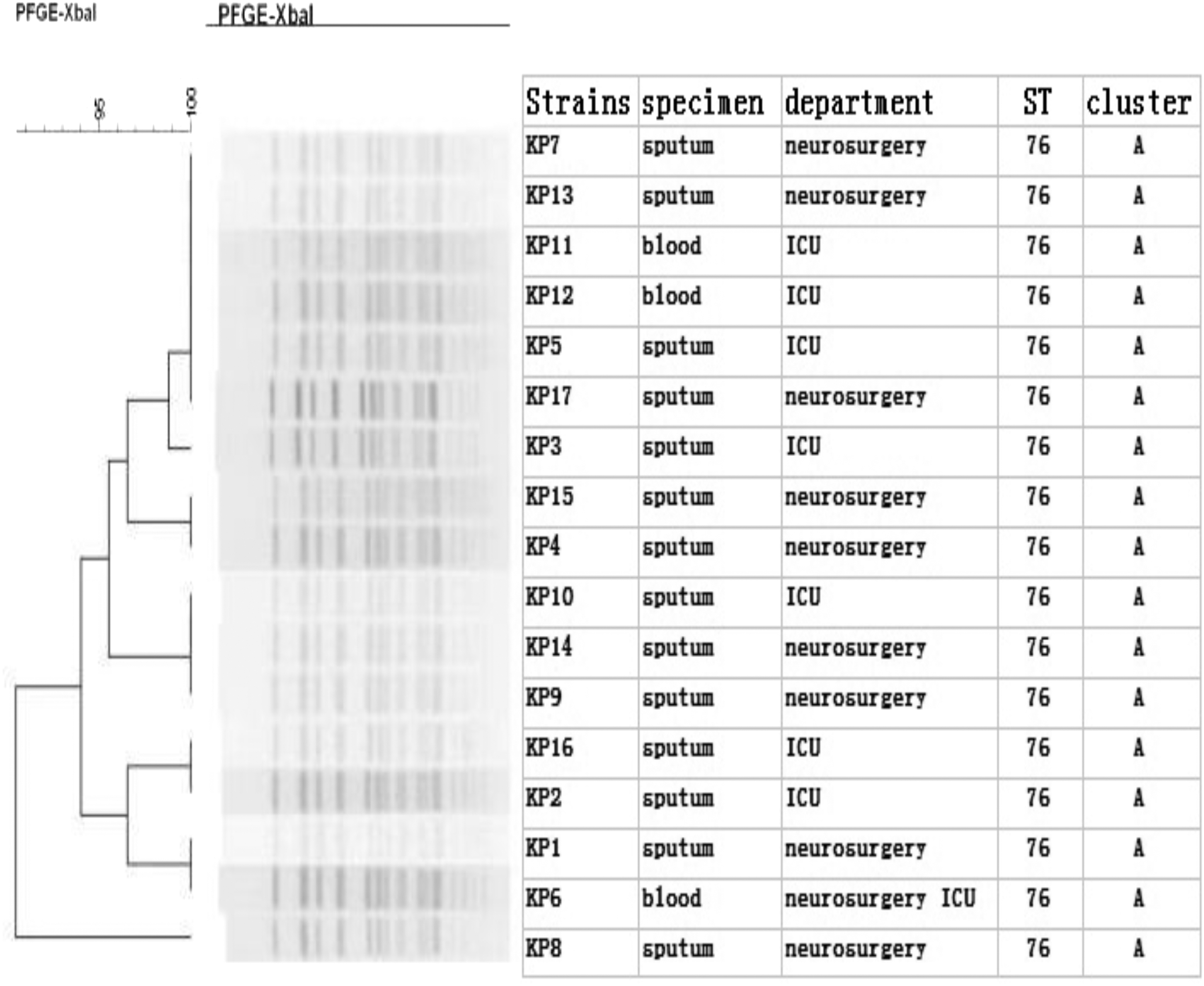
PFGE dendrogram of CRKP isolates from March 2016 to February 2017. All the isolates enclosed by rectangle belong to the A cluster, as well as sequence type ST76. PFGE, pulsed-field gel electrophoresis.
Conjugation experiments
Conjugation experiments revealed that plasmids harboring resistance genes were successfully transferred from three CRKP isolates to E. coli J53. These results are shown in Table 2. All transconjugants harbored blaKPC, blaSHV-1, blaCTX-M-15, qnrB, and acc(6′)Ib-cr resistance genes, but all recipients remained susceptible to cefepime, imipenem, amikacin, and levofloxacin. However, there was transconjugant JKP2 with resistance to piperacillin/tazobactam, and transconjugant JKP12 had resistance to ceftriaxone and ceftazidime.
Comparison of Donors and Transconjugant Minimal Inhibitory Concentration and Resistance Genes
KP2, KP6, and KP12 are the donor bacteria; JKP2, JKP6, and JKP12 are the recipients.
Genome sequencing and analysis
The sequencing of KP4 revealed a total of 155,278 (764,440,225 bp) paired-end reads that were generated by the Illumina HiSeq 2000 system and PacBio system. The draft genome consists of 5,921,738 bp with an N50 value of 4,191,470 bp and a guanine and cytosine content of 57%. The longest contig consisted of 60,010 bp. Our analysis showed that the KP4 genome consisted of a circular chromosome of 4,191,470 bp and three antibiotic resistance plasmids: tig7 (448,229 bp), tig1029 (33,653 bp), and tig1030 (92,144 bp). Based on a Prokka analysis, 6,051 putative open reading frames and 95 RNA genes on the circular chromosome are shown in Fig. 3.
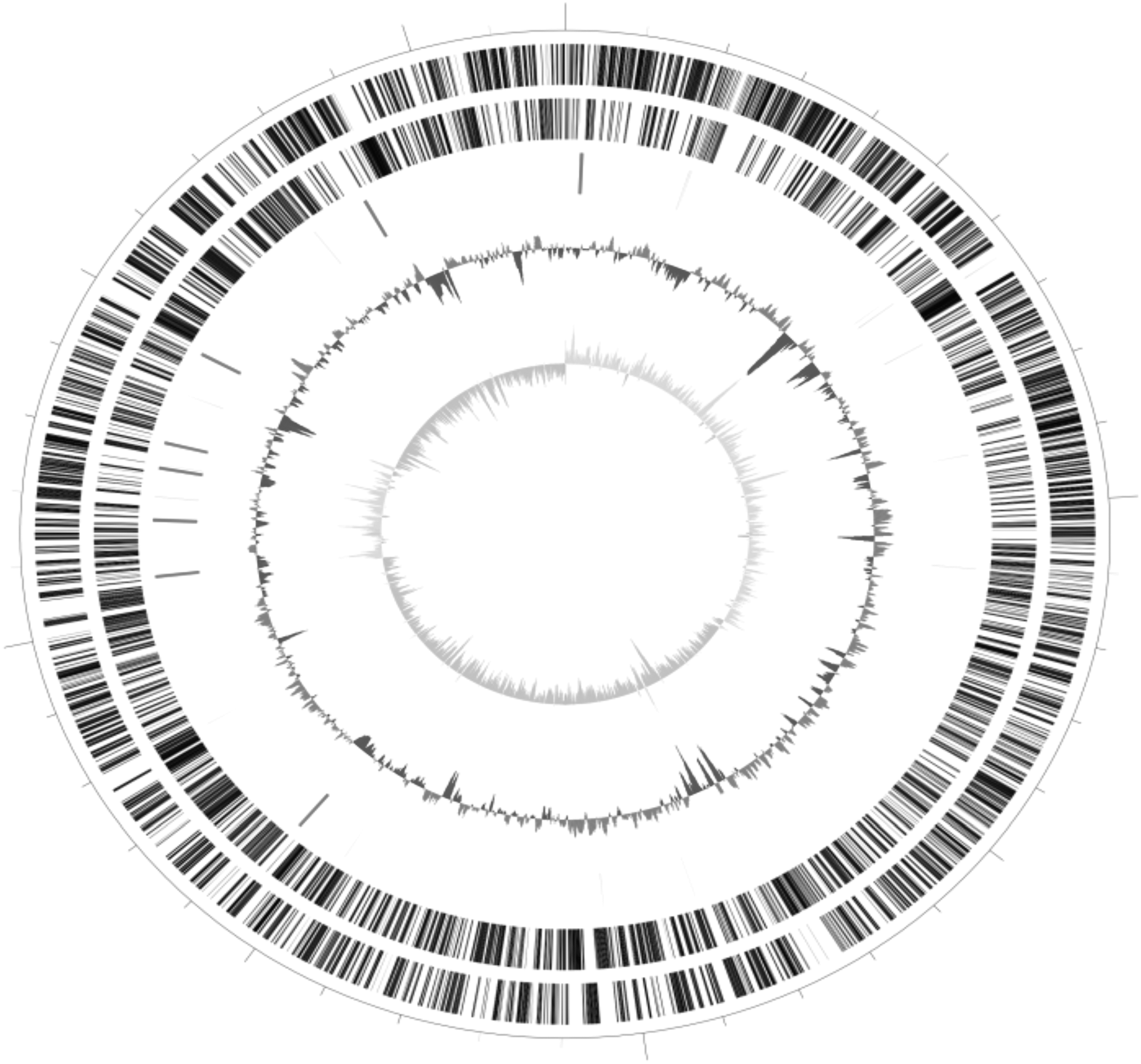
Schematic circular genome of KP4. The second and third circles from the outside to the inside represent the coding sequences on the positive and negative chains. The fourth circle represents rRNA and tRNA. The fifth circle represents the GC content, and the outer part indicates that the GC content in this region was higher than the average GC content of the whole genome. The innermost circle represents the GCskew value. GC, guanine and cytosine.
The plasmid carrying the carbapenem resistance gene blaKPC-2 on the tig7 plasmid belonged to the IncFIB (pQil) incompatibility group and had Tn1721- blaKPC-2-ΔT3 gene structure. BLASTn analysis revealed that the tig7 plasmid, with a 70% query coverage, was 99.45% similar to the K. pneumoniae TOP52_1721_U1 chromosome (GenBank accession no. PRJNA488268), which was isolated from a patient with a urinary tract infection. A schematic representation of the genetic environment of the blaKPC-2 genes on the tig7 plasmid is shown in Fig. 4. Resistance genes to aminoglycosides (aph(3″)-Ib and aph(6)-Id), quinolones (qnrB1), fluoroquinolones and aminoglycosides (aac(3)-IIa and aac(6′)-Ib-cr), ESBL (blaOXA-1, blaCTX-M-15, blaCTX-M-180, blaTEM-1B, and blaTEM-21), phenicols (catB3), sulfonamides (sul2), and trimethoprims (dfrA14) were identified on the tig1030 and tig1029 plasmids. KP4 contained some virulence-associated genes, including the iron acquisition genes aerobactin (iutA), enterobactin (entABCEF), and yersiniabactin (irp12, ybtAEPQTSUX, fyuA) and adhesin genes type 1 fimbriae (fimABCDEGH) and type 3 fimbriae (mrkD).

Discussion
From March 2016 to February 2017, a total of 17 CRKP isolates were detected from the ICU and neurosurgery unit of our hospital, and all of them were ST76. PFGE showed homology between all isolates, indicating an outbreak and spread between the two departments. These strains were different from ST11, which is the main epidemic strain in China; cases of ST76 have been rarely reported. ST76 has appeared in Shanghai, Nanchang, Qingdao, and Tai'an and has also been found in countries such as Israel and Bulgaria.7–9 However, none of its genetic characteristics has previously been reported. ST76 CRKP was isolated from an outbreak in Shanghai Children's Hospital in 2016, which did not cause any deaths. 10 The high mortality rate in our study may be closely related to the seriousness of the underlying diseases and complications of the patients. 11 Seventeen patients had severe craniocerebral injury and cerebrovascular disease and were treated with penicillins, cephalosporins, beta-lactamase inhibitors, and quinolones. Six of the eight patients with CRKP from the ICU had been treated with carbapenems; however, none of the patients was treated with carbapenems after the isolation of CRKP in neurosurgery unit, so they were considered to be cases of colonization. Neurosurgery unit patients often undergo invasive operations such as surgery, drainage, mechanical ventilation, catheterization, and transfer between the ICU and neurosurgery ICU wards. Thus, they are more likely to carry CRKP and cause infection when immunity is impaired.
Antimicrobial susceptibility testing of the 17 CRKP strains showed almost resistance to carbapenems, cephalosporins, beta-lactamase inhibitors, and aminoglycosides, but all strains remained highly susceptible to amikacin, levofloxacin, and ciprofloxacin, with good agreement with a report by Miao. 12 All strains carried the blaKPC-2, blaCTX-M-15, and blaSHV-1 genes, 16 strains carried the blaTEM-1 gene, and all of the tested strains contained 3 or more resistance genes. It is likely that the multiple resistances of CRKP are the result of the interaction of multiple genes. This study showed that the strain co-carrying qnrB and acc(6′)Ib-cr resistance genes accounted for 94.1%, and one strain contained the qnrS gene at the same time, which was inconsistent with general sensitivity to ciprofloxacin and levofloxacin. This finding may be related to the fact that quinolone resistance genes typically only confer low levels of quinolone resistance. 13 The resistance of the test strain to quinolone may also be related to changes in outer membrane permeability caused by gyrA and parC, making it difficult for the drug to enter the bacteria; however, further research is needed. The results showed that three strains successfully transferred resistance genes to the transconjugants, confirming that the resistance genes could be transferred horizontally between bacteria through plasmids. Although the resistance genes were successfully transferred, the MIC values of transconjugants were not significantly increased; imipenem was sensitive, and the MIC values of levofloxacin and amikacin were unchanged. This is possibly because the blaKPC-2 gene and other resistance genes are located in different plasmids that are potentially transferred to transconjugants together, thus affecting the expression of resistant genes. Although the transconjugants in this study were sensitive to imipenem, the horizontal transmission of multidrug resistance genes still needs an area of focus within hospitals.
Nearly 50 plasmids carrying blaKPC have been identified by whole genome sequencing analyses. BlaKPC is frequently located on different types of plasmids, including IncF, IncI, IncA/C, IncN, IncX, IncR, IncP, IncU, IncW, IncL/M, and ColE plasmids. 14 According to the differences between plasmid replicates, it appears that blaKPC mainly exists in the IncF plasmid, which is consistent with our findings. Tn4401 was first found in Europe and America and was considered to be the origin of the spread of the blaKPC gene. Subsequently, a series of studies have found that the blaKPC gene in China is mainly located in the transposon Tn1721 and is divided into two subtypes, A and B. The basic structure of Tn1721B is Tn1721, blaKPC-2, an additional inverted repeat sequence (IRL2), and several other genetic elements: Tn3, ISKpn6, and ISKpn8. 15 Li et al. reported that the gene environment of IncFIB plasmid carrying blaKPC gene, including Tn3, ISKpn8, and ISKpn6-like elements, found a 245-bp blaTEM insertion upstream of blaKPC-2 gene, in good agreement with the findings of this experiment. 16 Tn1721 transposon has primarily been reported in ST11 K. pneumoniae. This is its first report in ST76 K. pneumoniae, suggesting that the transfer of mobile elements carrying the blaKPC gene could cause more strains of K. pneumoniae to become resistant to carbapenem. The blaKPC gene copy number, the insertion or deletion of an upstream sequence to alter the structure of the promoter region, and loss of outer membrane porins are all factors that could affect the expression of the blaKPC gene, resulting in a change in the MIC value of the horizontally transmitted strain. 5
Iron is a necessary condition for K. pneumoniae to grow and reproduce during infection. The pathogen acquires iron from the host cell through a highly efficient iron uptake system, and the synthesized iron carrier combines with iron in the host transferrin to form a Fe3+ iron carrier complex that is recognized by the iron receptor protein on the outer membrane of the bacteria. Upon binding, this releases iron into the bacterial cells, promoting growth or reproduction and causing bacterial infection to intensify or spread. 17 The iron acquisition genes enterobactin (entABCEF) and aerobactin (iutA) play roles in combining iron with transferrin and permitting transfer from host cells, respectively. The product of virulence gene yersiniabactin (irp12, ybtAEPQTSUX, fyuA) not only has affinity to iron but also promotes the formation of biofilms by activating the outer membrane protein fyuA in the absence of iron to enhance virulence. 18 The combined action of various iron carriers increases the reproductive and pathogenic abilities of K. pneumoniae. Type 1 fimbriae, encoded by the fim A, B, C, D, E, G, and H genes, have been reported to be expressed in the urinary tract and contribute to bacterial adhesion, causing urethritis and cystitis. 19 The mrkD gene, encoding type 3 fimbriae, is thought to cause binding of bacteria to the trachea, oral cells, and lung tissue, mediating biofilm formation, and is associated with ventilator-associated pneumonia. 20 Both of these genes are associated with bacterial adhesion, making it easier for resistant bacteria to colonize patients. The presence of proadhesion properties in ST76 CRKP poses a challenge to treatment and may be one of the main contributing causes of this outbreak.
In this study, we reported a nosocomial outbreak of KPC-2–producing K. pneumoniae ST76 in the ICU and neurosurgery unit. To our knowledge, this is the first report of the whole genome sequence of KPC-2–producing K. pneumoniae ST76, providing a basis for understanding antibiotic resistance and genomic evolution. Specific infection control measures should be implemented to prevent the colonization and spread of CRKP in ICU and neurosurgery unit in our hospital: we recommend isolating patients with confirmed carbapenem-resistant Enterobacteriaceae infection, ensuring proper hand hygiene of medical staff, wearing isolation clothes, and using separate medical. Furthermore, implementation of active screening for patients who enter the ward, contact prevention for positive patients, reduction of invasive operations, and rational use of antibiotics could help prevent future outbreaks. Regular disinfection of the environment and articles in the ward, frequent bedding changes, and sterilization of the patient's medical waste may also help eliminate residual bacteria in infected patients' rooms. In summary, there is a need for strengthening the regular monitoring of wards to reduce the colonization and spread of resistant bacteria.
Footnotes
Acknowledgments
The authors thank Dr. Ming-Gui Wang from Huashan Hospital, affiliated with Fudan University, and Dr. Yun-Song Yu from Sir Run Run Shaw Hospital, affiliated with Zhejiang University, for their assistance with this work. The authors thank the team of curators at the Institute Pasteur MLST System (Paris, France) for importing novel alleles, profiles, and/or isolates to the Institute Pasteur MLST database.
Authors' Contributions
All authors contributed to this work. X.L.Z. and J.S.Z. conceived and designed the experiments; S.S.S., Y.X.Z., Y.F., and C.J.L. performed the experiments; L.Y., Y.W., and M.J.B. analyzed the data; and Y.C.W. wrote the article. S.S.S. and C.J.L. are the co-first authors. All authors reviewed and approved the final article.
Ethics Approval and Consent to Participate
The experimental protocols were approved by the Ethics Committee of Jiamusi University Clinical Medical College for Research. The committee's reference no. was 2018025. The need for individual informed consent was waived by the ethics committee because this study used previously existing samples collected during the course of routine medical care and did not pose any additional risks to the patients.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Excellent Team of Young Teachers Foundation of Heilongjiang Province (2018-KYYWF-0916), Heilongjiang Provincial Health and Family Planning Commission on Scientific Research Project (2017–405), and Jiamusi University President Innovation and Entrepreneurship Fund Project (XZYF2018–43).