
Abstract
Introduction:
Carbapenem-resistant Enterobacteriaceae (CRE) represents an urgent threat worldwide. We aimed to investigate the frequency of carbapenem-resistant Klebsiella pneumoniae and Escherichia coli in Iran.
Materials and Methods:
PubMed/Medline, Embase, Scopus, Web of Sciences, and Iranian databases were searched to find potentially relevant articles. Statistical analyses were performed using STATA version 14.
Results:
Forty-nine studies fulfilled the inclusion criteria. The pooled rates of resistance to carbapenem in K. pneumoniae and E. coli were 24.0% (95% confidence interval [CI] 18.0–31.0) and 5.0% (95% CI 2.0–8.0), respectively. blaOXA-48 gene was the most common cause of carbapenem resistance in K. pneumoniae and E. coli.
Conclusions:
CRE is prevalent in Iran, which confers the importance of strength prevention and control measures.
Introduction
The multidrug-resistant gram-negative bacteria (MDR-GNB) are an important threat to public health. Carbapenems, a class of β-lactam antimicrobials, are considered last-line agents against MDR-GNB. This is due, in part, to their broad-spectrum antibacterial activity.1–4 The increasing prevalence of carbapenem-resistant Enterobacteriaceae (CRE) strains is related to high mortality and it is increasing around the world. 1 In the USA, there were an estimated 140,000 cases per year of health care-associated CRE infections. 5 Among the Enterobacteriaceae family, Klebsiella pneumoniae and Escherichia coli are among the most common agents of community- and hospital-acquired infections.6–8 They are also among the most common agents reported for CRE infections around the world. 5
There are various types of mechanisms that lead to carbapenem-resistant GNB. One of the main mechanisms is acquiring plasmid-encoding carbapenemase. 9 According to the Ambler classification, there are three classes of carbapenemase: (1) class A containing serine carbapenemases such as non-metallocarbapenemase/imipenemase (NMC/IMI), KPC (K. pneumoniae carbapenemase), Guiana extended-spectrum β-lactamase, and Serratia marcescens enzyme (SME); (2) class B containing metallo-β-lactamases (MBLs) such as VIM (Verona integrin-encoded metallo-β-lactamase), NDM (New Delhi metallo-β-lactamase), and imipenemase (IMP); and (3) class D containing enzymes such as OXA-48 (oxacillinase-48), OXA-232, OXA-181, and OXA-204.10–14 In the study by Grundmann et al., the most common carbapenemases in E. coli and K. pneumoniae were OXA-48-like enzymes and KPC enzymes, respectively.15,16 Another mechanism that leads to carbapenem resistance is overexpression of ESBL and/or AmpC β-lactamases combined with a reduction of membrane permeability due to porin modification. Modification of two major porins, OmpK35 or OmpK36, in K. pneumoniae or complete loss of porins, OmpF and OmpC, as in E. coli can lead to carbapenem resistance.6,17,18
There are many original reports from Iran about the prevalence of CRE in recent years,19,20 but, a comprehensive systematic review and meta-analysis have not been conducted. Thus, the purposes of this work were to estimate the frequency of carbapenem-resistant K. pneumoniae and E. coli in Iran and to define the mechanisms that lead to carbapenem resistance in these two bacterial species.
Materials and Methods
Search strategy and study selection
PubMed/Medline, Embase, Scopus, Web of Sciences, and Iranian databases from January 2010 to June 2019 were searched to identify potentially relevant studies. The search terms were as follows: “Klebsiella pneumoniae” OR “Escherichia coli” AND (“carbapenem” or ‘imipenem” or “meropenem”) AND Iran. Similar strategies were used for Iranian databases.
Two authors (M.A. and F.F.) independently reviewed the potentially relevant studies and disagreements were resolved by consensus discussion.
Articles were included if they reported the carbapenem resistance in clinical isolates of K. pneumoniae and/or E. coli and/or described the mechanisms of carbapenem resistance in these bacteria. Only studies written in English or Persian were included. Case reports and reviews were excluded. Our study was according to the PRISMA guideline. 21
Data extraction
The following data were extracted by two independent reviewers: first authors, published year, city, sample size, mean age, sites of infection, proportion of resistance, diagnostic methods, and the mechanisms of carbapenem resistance.
Quality assessment
We assessed the quality of the references according to the checklist provided by JBI (Joanna Briggs Institute). 22
Data analysis
The combined rates of carbapenem-resistant K. pneumoniae and E. coli, with 95% confidence intervals (95% CIs), were analyzed by the random-effects model. Q- and I2 statistics were used to assess the between-study heterogeneity. 23 To assess the possibility of publication bias, we performed the Begg's test. 24 STATA version 14 was used to analyze the data.
Results
From the databases, 1,066 publications were retrieved. After the evaluation of the titles, abstracts, and full texts, 49 studies were included in this systematic review and meta-analysis (Fig. 1). These 49 studies were divided into 2 groups comprising 39 datasets (35 investigations the mechanisms of carbapenem resistance and 33 investigating the frequency of carbapenem resistance) for K. pneumoniae and 18 datasets (10 investigating the mechanisms of carbapenem resistance and 14 investigating the frequency of carbapenem resistance) for E. coli. Characteristics of the included articles are described in Tables 1 and 2.
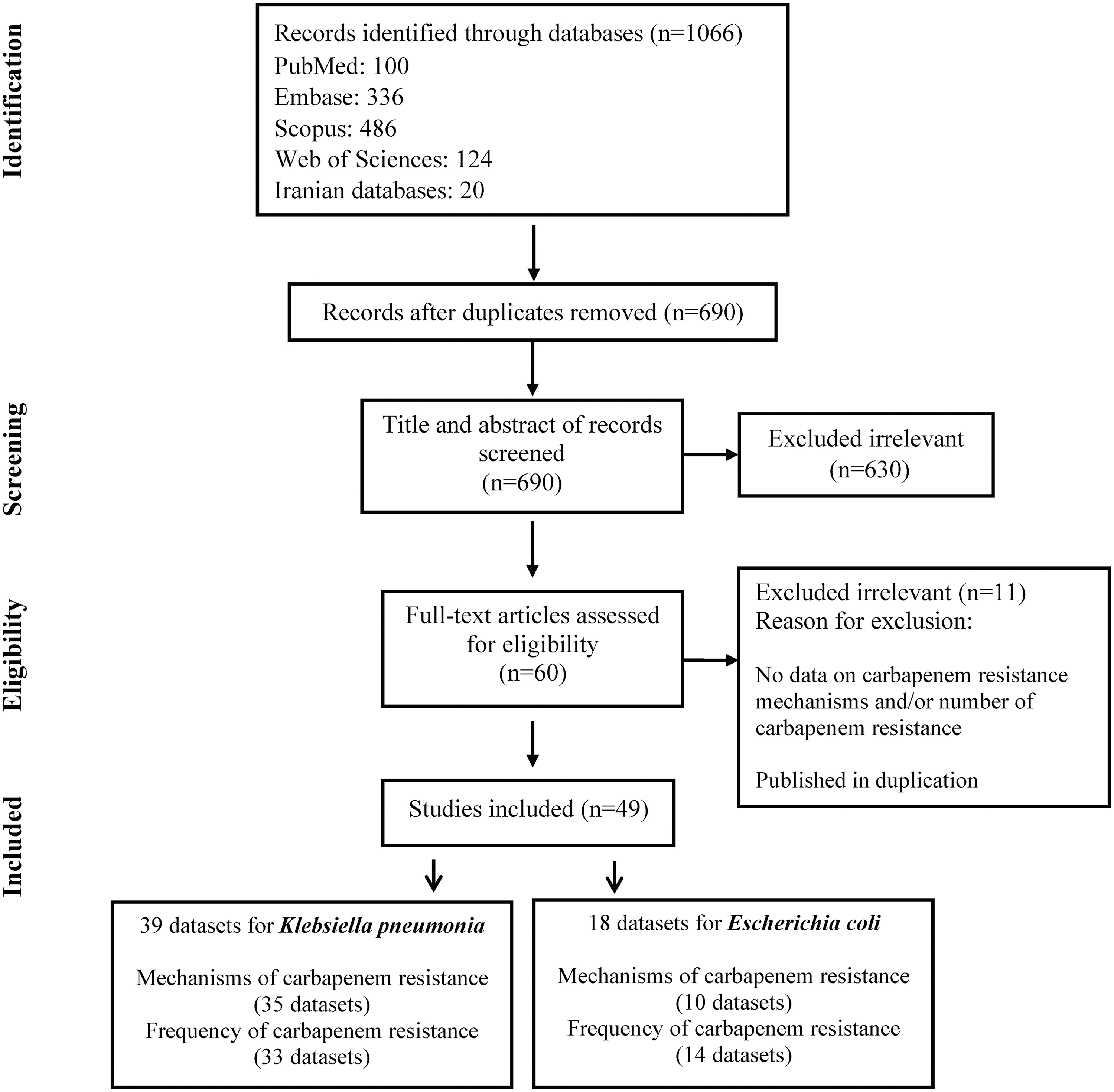
Flowchart for selection of the study.
Characteristics of Included Studies for Klebsiella pneumoniae
NR, not reported.
Characteristics of Included Studies for Escherichia coli
MHT, modified Hodge test.
All included articles were cross-sectional studies, including from 23 to 992 clinical samples per study. Studies were conducted in different cities; Tehran and Isfahan were the most frequently represented cities. Resistance was determined according to the Clinical and Laboratory Standards Institute (CLSI) guidelines in all included studies. PCR, disk diffusion, and modified Hodge tests were used to determine the CRE. Based on the JBI, the included articles had a low risk of bias.
Frequency and mechanisms of carbapenem resistance in K. pneumoniae
The estimated rate of carbapenem-resistant K. pneumoniae was 24.0% (95% CI 18.0–31.0, I2: 96%) (Fig. 2). Based on Begg's test, publication bias was observed (p = 0.013).

The pooled rate of resistance to carbapenem in Klebsiella pneumonia.
Our analysis indicated that 47.1% of carbapenem-resistant K. pneumoniae possessed the blaOXA-48 gene. Therefore, blaOXA-48 was responsible for resistance to carbapenem in the majority of clinical isolates of K. pneumoniae (Table 3). The data also indicated that the acquisition of blaNDM gene is the second cause of resistance to carbapenems in K. pneumoniae.
Mechanisms of Carbapenem Resistance in Klebsiella pneumoniae
Frequency and mechanisms of carbapenem resistance in E. coli
The estimated rate of carbapenem-resistant E. coli was 5.0% (95% CI 2.0–8.0) (Fig. 3). No evidence of publication bias was observed (Begg's tests p-value was 0.139).

The pooled rate of resistance to carbapenem in Escherichia coli.
As shown in Table 4, blaOXA-48 (37.1%), blaNDM (21.9%), and blaIMP (9.6%) genes were responsible for carbapenem resistance in E. coli.
Mechanisms of Carbapenem Resistance in Escherichia coli
Discussion
The emergence and distribution of CRE are classified as one of the highest risks for public health. There is a high risk of infection with CRE in patients with prior antibiotic exposure and suppressed immune systems, recipients of organ transplant, invasive devices like central venous catheters, or those mechanically ventilated for more than 72 hours.5,25 In Iran, there is an increasing prevalence of CRE, which is similar with neighboring countries, including Turkey, Iraq, and Pakistan with relatively high rates of CRE.26–29 Unfortunately, there are no surveillance programs for the prevalence of CRE in Afghanistan, but there are some reports of detecting CRE strains. 27
Carbapenems are important for the treatment of health care-associated infections and are used when bacteria have high antibiotic resistance.30,31 Therefore, the increased prevalence of CRE may lead to increased mortality, prolonged hospital course, as well as increased health care spending and utilization.31,32
As mentioned, one of the main mechanisms of resistance to carbapenem in E. coli and K. pneumoniae is the production of carbapenemase (i.e., NDM, KPC, VIM, IMP, and OXA).9,33 Other mechanisms of resistance are the modification of porins combined with the overproduction of AmpC β-lactamases. 17 The current meta-analysis indicated that blaOXA-48 gene (47.1%) and blaNDM gene (30.11%) were responsible for resistance to carbapenem in K. pneumoniae. Likewise, the most commonly reported mechanisms of resistance to carbapenem in E. coli were due to the existence of blaOXA-48 (37.17%) and blaNDM (21.92%) genes, respectively.
These bacterial strains can receive the plasmid carrying the blaOXA-48 gene and therefore can produce OXA-48 carbapenemase.34,35
The OXA-48 is a β-lactamase in class D Ambler classification and can hydrolyze penicillins and imipenem, and has trivial activity against broad-spectrum cephalosporins. 36 However, in one study, about 25% of OXA-48 carbapenemase producers showed susceptibility to extended-spectrum cephalosporins. 35 Initially, OXA-48 carbapenemase was first reported from Turkey, by isolating from a K. pneumoniae clinical strain, in 2001. 37 Dissemination of blaOXA-48 gene is frequently by insertion of Tn1999-like transposons in pOXA-48a plasmid, and becomes a major concern in antimicrobial drug resistance.37,38
The data also indicated that the acquisition of blaNDM gene is the second most common cause of carbapenem resistance in E. coli and K. pneumoniae. The blaNDM gene can be found in different types of plasmids (i.e., IncHI1, IncX, and IncL/M). 32 The blaNDM is an MBL that is not inhibited by β-lactam inhibitors and hydrolyzes most of β-lactams, including carbapenems, penicillins, and cephalosporins; however, this does not have an effect on aztreonam.39,40 The blaNDM gene has been spread worldwide and bacterial strains producing blaNDM are endemic in India, Balkan, and Middle Eastern countries. There are new concerns about South Africa becoming endemic as well.41,42
The CRE is spreading around the world may be due to the travel of patients to other countries. 43 Also, there are limited treatment options for CRE, because these strains are resistant to many antimicrobial drugs, so it is necessary to follow appropriate control and treatment for patients infected with CRE. The available therapeutic options are divided into two categories of mono-therapies and combination therapies. Currently, the active drugs for the treatment of CRE include the polymyxins, tigecycline, fosfomycin, and aminoglycosides. 44 Several studies reported combination therapies due to synergistic effects of antibiotics and persistence against the emergence of drug monoresistance lead to better clinical outcomes and a decrease in mortality.45,46
Delayed antibiotic treatment for severe infections with CRE, such as severe sepsis, could increase the mortality, so a proper empirical therapy based on suspected bacterial agents, epidemiology of local drug resistance, and patient risk factors should be performed. 47 Therefore, for severe infections with CRE, an empirical therapy, including the combination of carbapenems, colistin, or aminoglycosides, according to the epidemiology of local drug resistance should be prescribed. 47
Some limitations to this study need to be presented. Data about noncarbapenemase carbapenem-resistant mechanisms, including modification of porins in K. pneumoniae and E. coli, were limited and needed more investigations for better comparing the mechanisms of CRE. Another limitation was due to the lack of data about CRE in some of the regions of Iran; the reported prevalence of this study does not fully represent the situation of CRE in Iran. Likewise, there were limited data about risk factors for CRE infections that needed further studies. In addition, not all included studies tested the same carbapenemase genes. Thus, the frequency of each carbapenemase gene in this study may be biased. Finally, there was heterogeneity between the included studies.
In conclusion, these results indicated that CRE is prevalent in Iran, which confers the importance of strength prevention and control strategies.
Footnotes
Authors' Contributions
M.J.N. and P.T.: designed the study. M.J.N., M.A., F.F., B.D., S.D., S.Z., and B.H.: performed the search, study selection, and statistical analysis. M.J.N. and S.M.J.M.: wrote the first draft of the article. M.J.N., M.M., M.G., H.G., Z.S.S., H.D, and P.T.: revised the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Shahid Beheshti University of Medical Sciences, Tehran, Iran.