
Abstract
We aimed to compare efficacy of different patterns of antibiotics and explore the risk factors related to mortality in patients with bloodstream infections (BSIs) due to carbapenem-resistant Klebsiella pneumoniae (CRKP). This study retrospectively included 89 patients with BSIs due to CRKP with complete data during the year of 2018 in the First Affiliated Hospital of Zhejiang University School of Medicine. Overall, the 28-day mortality was 47.2% (42/89). Multivariate analysis of Cox regression revealed that hematological malignancy (hazard ratio [HR] 5.698; 95% confidence interval [CI], 2.405–13.504; p < 0.001) and Pitt bacteremia score (HR per unit increase, 1.303; 95% CI, 1.109–1.532; p = 0.001) were identified as independent predictors for 28-day mortality. Among 70 patients with appropriate therapy, 35 received tigecycline (TGC)-based therapy, 20 received polymyxin B (PMB)-based therapy, 9 received ceftazidime/avibactam-based therapy, and 6 patients had other kinds of antibiotics, including ciprofloxacin, amikacin, and cotrimoxazole. By adjusting variables selected by crude analysis, it showed that receiving PMB-based therapy provided a survival benefit comparing with TGC-based therapy (HR, 0.068; 95% CI, 0.018–0.260; p < 0.001). Hematological malignancy and Pitt bacteremia score were independent risk factors of death in patients with BSIs due to CRKP and PMB-based therapy improved survival rate compared with TGC-based therapy.
Introduction
Carbapenem-resistant Klebsiella pneumoniae (CRKP) infections have become an important public health problem in recent years. Patients with bloodstream infections (BSIs) due to CRKP suffer significantly high mortality (28- or 30-day all-cause mortality between 33.0% and 52.8%) worldwide.1–5 The survival rate is even lower in China compared with developed countries as a result of few choices in effective antibiotics.6,7 Carbapenems with prolonging injection duration and tigecycline (TGC) were widely accepted therapies for CRKP infections formerly. Unfortunately, CRKP strains isolated from Chinese hospitals appear to have high minimum inhibitory concentrations (MICs) for carbapenems for the past few years,6,7 which results in poor efficacy by administration of carbapenems. TGC in treating BSIs stays controversial because of its inability to achieve adequate concentrations in serum.8,9 Effective medications in previous studies such as polymyxins and ceftazidime/avibactam (CAZ/AVI) have not been available until 2018 and 2019 in China, respectively, so that we do not have enough data on efficacy in real world of these antibiotics. In this study, we reviewed medical records of patients with BSIs due to CRKP to compare different antimicrobial treatment options and identify risk factors of death in the First Affiliated Hospital of Zhejiang University Medical College, China.
Materials and Methods
Study design
This was a retrospective study conducted in the First Affiliated Hospital of Zhejiang University Medical College, a teaching hospital with 2500 beds in Hangzhou, China. Patients were included in this study if they were diagnosed with BSIs due to CRKP in this hospital from January 1 to December 31, 2018. For patients with ≥2 episodes of bacteremia, only the first episode was included. Patients would be excluded if (i) the positive culture results were considered contaminants as recorded in medical notes and (ii) key data, including 28-day outcomes, were missing.
Medical records were reviewed and the following data were collected: patients' demographic characteristics, underlying diseases, vital signs, mental status, organ support therapies, including continuous renal replacement therapy (CRRT) and mechanical ventilation, culture, and sensitivity results from different samples, antimicrobial regimens, including dose and duration, survival time, and outcomes within 28 days from onset of bacteremia. Charlson comorbidity index score, Pitt bacteremia score, and INCREMENT-carbapenemase-producing Enterobacteriaceae (CPE) mortality score were calculated.10–12
This study has been reviewed and approved by the Research Ethics Committee of the First Affiliated Hospital of Zhejiang University (ref# 2019-615).
Definitions
Onset of BSIs was defined as the date of collection of the first blood culture yielded CRKP. Microbial eradication was defined as negative culture for CRKP in blood specimens during follow-up. Charlson comorbidity index score was used to evaluate the comorbidities of patients. 10 Pitt bacteremia score was used to evaluate the severity of illness. 11 Receiving mechanical ventilation and CRRT was defined as having these treatments for at least 48 hr after onset of BSIs. Source of BSIs was judged by clinical and microbiological data. Severe sepsis and septic shock were defined according to an the Society of Critical Care Medicine (SCCM)/European Society of Intensive Care Medicine (ESICM)/American College of Chest Physicians (ACCP)/American Thoracic Society (ATS), and Surgical Infection Society (SIS). International Sepsis Definitions Conference Consensus. 13 INCREMENT-CPE mortality score was calculated from following variables: severe sepsis or shock at presentation (5 points); Pitt score of 6 or more (4 points); Charlson comorbidity index of 2 or more (3 points); source of BSIs other than urinary or biliary tract (3 points); inappropriate empirical therapy, and inappropriate early targeted therapy (2 points). 12
In this study, we considered antibiotic therapy appropriate if administered 5 days or less after onset of BSIs and including at least one active drug. If the active drug was started in 2 days or less after onset, we considered it early appropriate therapy. If the regimen was changed, the antibiotic regimen was identified as the one started in the 5 days or less after onset of BSIs and administered for at least half of the duration of therapy (for patients who died <48 hr after the start of therapy, at least one complete day of therapy was required). 14 Antibiotics were considered active if the isolate was susceptible or exhibited intermediate susceptibility according to 2017 Clinical and Laboratory Standards Institute (CLSI) criteria (see below for details). 15 Treatment regimens were classified as monotherapy (treatment with one in vitro active antibiotic) or combination therapy (treatment with two or more in vitro active antibiotics). Treatment with TGC and any other antibiotics except polymyxin B (PMB) and CAZ/AVI was considered receiving TGC-based therapy. Treatment with PMB and any other antibiotics except CAZ/AVI was considered receiving PMB-based therapy. Treatment with CAZ/AVI and any other antibiotics was considered as CAZ/AVI-based therapy. In our center, generally, TGC was administered every 12 hr for a total daily dose of 200 mg and PMB was administered every 12 hr for a total daily dose of 2.5 mg/kg of weight.
Microbiology
The isolates from blood were identified by the Vitek GNI-card (bioMérieux, Marcy-l'Étoile, France). Susceptibility testing was performed and interpreted according to the CLSI guidelines. 15 Carbapenem resistance was defined as an MIC of ≥2 μg/mL for ertapenem, or an MIC of ≥4 μg/mL for imipenem or meropenem. 15 Susceptibility for CAZ/AVI was defined as an MIC of ≤8/4 μg/mL. 15 The MIC of TGC was determined by using standard broth microdilution tests with fresh (<12 hr) Mueller–Hinton II Broth (cation-adjusted; Solarbio Science and Technology Ltd., Beijing, China). TGC susceptibility was defined as an MIC of ≤2 μg/mL according to the United States Food and Drug Administration breakpoints. 16 European breakpoints published by the European Committee on Antimicrobial Susceptibility Testing were used for identification of PMB susceptibility (an MIC of ≤2 mg/L as susceptible). 17
Statistical analysis
Continuous variables with a normal distribution were shown as mean and standard deviation, and those with a nonnormal distribution were shown as median and interquartile range (IQR). Bivariate associations between the binary outcome of 28-day all-cause mortality and patients' characteristics were assessed using univariate Cox regression analysis. All variables with p < 0.05 in the univariate analysis were entered into a Cox proportional-hazards model for multivariate analysis. Their contribution was assessed using the likelihood ratio test. Data were processed and analyzed by the Statistical Package for Social Science (IBM SPSS [R 24.0.0.0], Chicago, IL).
Results
Patient characteristics
A total of 89 patients were included in this study during a 1-year period. Twenty-four patients (27.0%) were female and 65 patients (73.0%) were male. The mean patient age was 55.2 ± 18.1 years (range, 16–90 years). Among all 89 patients, 29 received solid organ transplantation (SOT), including 21 having liver transplantation, 2 kidney, 2 simultaneous pancreas-kidney, 2 lung, and 2 heart; 15 had hematological tumors, including 7 receiving hematopoietic stem cell transplantation (HSCT). Twenty patients had diabetes mellitus. The median duration of hospitalization before the onset of bacteremia was 19 days (IQR, 9–35 days). Pitt bacteremia score of all patients was 3 points (IQR, 1–6 points). Over half of the patients (57.3%) developed severe sepsis or septic shock. More details are shown in Table 1.
Demographic and Clinical Characteristics of Eighty-Nine Patients with Bloodstream Infection due to Carbapenem-Resistant Klebsiella pneumoniae
Data are shown as mean ± standard deviation, median (P25, P75) or n (%).
In the subgroup of patients receiving appropriate therapy n = 70.
CPE, carbapenemase-producing Enterobacteriaceae.
Microbiology
All CRKP isolates were resistant to penicillin-inhibitor combinations and expanded-spectrum cephalosporins. The majority of the isolates were resistant to ciprofloxacin (98.9%), gentamycin (78.7%), co-trimoxazole (76.4%), and amikacin (68.5%). Resistance frequency to ertapenem was 100%; the MICs were 2 μg/mL in two isolates and ≥4 μg/mL in all others. Among the isolates, 96.6% were resistant to imipenem with MICs ≥8 μg/mL. Of the isolates, 96.6% were resistant to meropenem, 2 isolates having an MIC of 8 μg/mL, 65 having an MIC of 16 μg/mL, and 19 having an MIC of >16 μg/mL. The most active drugs were TGC (94.7% susceptible), PMB (100% susceptible), and CAZ/AVI (100% susceptible).
Risk factors of mortality
Crude analysis of Cox regression showed that hematological malignancy, SOT, Pitt bacteremia score, severe sepsis or septic shock, and appropriate therapy were associated with 28-day mortality (p < 0.05). By entering these variables into multivariate analysis of Cox regression, it revealed that hematological malignancy (hazard ratio [HR] 5.698; 95% confidence interval [CI], 2.405–13.504; p < 0.001) and Pitt bacteremia score (HR per unit increase, 1.303; 95% CI, 1.109–1.532; p = 0.001) were identified as independent predictors for 28-day mortality (Table 2).
Univariate and Multivariate Cox Regression Analysis for Mortality of Patients with Bloodstream Infection due to Carbapenem-Resistant Klebsiella pneumoniae (n = 89)
ICU, intensive care unit; CI, confidence interval; HR, hazard ratio.
Therapies and outcomes
Overall, the 7-day all-cause mortality was 28.1% (25/89), 14-day 37.1% (33/89), and 28-day 47.2% (42/89). The overall microbiological eradication rate was 59.6%.
Among 70 patients with appropriate therapy, 35 received TGC-based therapy, 20 received PMB-based therapy, 9 received CAZ/AVI-based therapy, and 6 patients had other kinds of antibiotics, including ciprofloxacin, amikacin, and co-trimoxazole. To compare the efficacy of TGC-based and PMB-based therapy, we analyzed data from patients receiving these two patterns of antibiotics. By adjusting variables selected by crude analysis, it showed that receiving PMB-based therapy provided a survival benefit comparing with TGC-based therapy (HR, 0.068; 95% CI, 0.018–0.260; p < 0.001) (Table 3; Fig. 1).
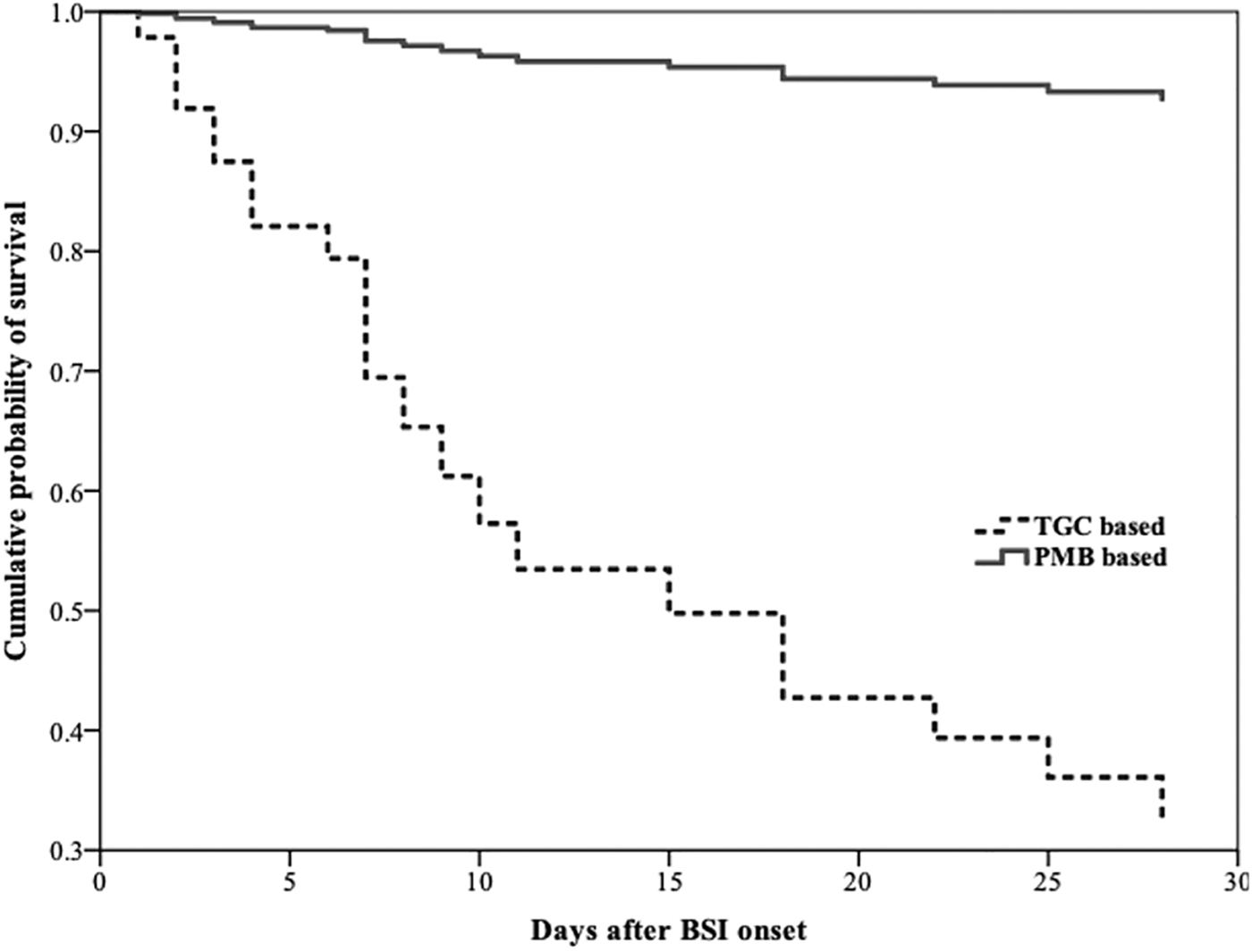
Cumulative probability of survival of patients with BSIs due to carbapenem-resistant Klebsiella pneumoniae receiving TGC- and PMB-based therapy (n = 55), p < 0.001 (Cox proportional-hazards regression model). BSI, bloodstream infection; TGC, tigecycline; PMB, polymyxin B.
Univariate and Multivariate Cox Regression Analysis for Mortality of Patients with Bloodstream Infection due to Carbapenem-Resistant Klebsiella pneumoniae and Receiving Tigecycline- or Polymyxin B-Based Therapy (n = 55)
TGC, tigecycline; PMB, polymyxin B.
Because of a relatively small number of patients receiving CAZ/AVI-based therapy, we listed the clinical characteristics of these patients in Table 4. Interestingly, all of nine patients receiving CAZ/AVI were SOT recipients. Eight of nine of them had microbiological response. Seven of nine had clinical response and finally survived on day 28.
Clinical Information of Patients with Bloodstream Infection Caused by Carbapenem-Resistant Klebsiella pneumoniae Receiving Ceftazidime/Avibactam
eCrCL, estimated creatine clearance, which was calculated by Cockcroft-Gault Formula; MIC, minimum inhibitory concentration.
Discussion
CRKP infection has become a great concern in clinical practice because of extremely poor situation of the patients, who usually stay in intensive care units or have severe underlying diseases, and lack of effective antibiotics worldwide. Our study focused on efficacy of different antibiotic patterns and risk factors of mortality on patients with BSIs due to CRKP in a teaching hospital in China during a 1-year period. In 89 patients included, the overall 28-day mortality was 47.2%. Hematological malignancy and Pitt bacteremia score were identified as independent risk factors of 28-day mortality. Seventy patients received appropriate therapy, most of whom were administered by TGC- and PMB-based therapy. By adjusting confounding factors, we found that receiving PMB-based therapy provided a significant survival benefit comparing with TGC-based therapy with an HR of 0.068. Descriptive results of patients receiving CAZ/AVI showed a quite low mortality of BSIs due to CRKP, but factors such as the relatively young age, SOT, and combination therapy with other antibiotics of those patients should be carefully considered.
The INCREMENT project, a retrospective international cohort study, including patients with BSIs due to extended-spectrum β-lactamase-producing Enterobacteriaceae or CPE, has given us a predictive score for early mortality of BSIs due to CPE. 12 In this study, we analyzed association between mortality and most important factors from the score and also some other clinically significant variables from clinical practice. The increase of each unit in Pitt bacteremia score adds 30% of mortality risk according to this study. Pitt bacteremia score was a well-known predictor of mortality according to previous studies.12,18,19 Other predictors in the INCREMENT-CPE mortality score were not statistically significant from our data. Reasons might be (i) the relatively small number of patients in our study and (ii) that a large percentage of patients in our cohort were with hematological tumors and SOT. Patients with hematological tumors have five times the mortality risk of those without hematological tumors. As we know, hematological patients are at high risk of developing infection because of neutropenia, chemotherapy, HSCT, and frequent hospitalizations. Studies from different areas showed that short-term all-cause mortality rates after carbapenem-resistant Enterobacteriaceae (CREs) infections in patients with hematologic tumors and HSCT ranged from 40% to 67%.3,20–22
TGC and polymyxin are commonly used in those patients in our center and retrospective data showed that polymyxin-based therapy provided a survival benefit than TGC-based therapy. However, this conclusion may not be easily extended to other patients out of our center or in other circumstances. Existing evidence is mostly based on observational studies. A recent systematic review, including 54 observational studies involving 3,195 CRKP-infected patients, found no significant differences in mortality, clinical or microbiological responses combination-containing and combination-sparing regimens of polymyxins, TGC, aminoglycosides, and carbapenems. Clinical outcomes did not significantly differ among the various monotherapies in the study. 23 Optimal therapy for CRKP infections still need to be defined by large-scale and well-designed randomized clinical trials.
This study displayed efficacy of CAZ/AVI in treating BSIs due to CRKP, with a high survival rate of 77.8% (7/9). The survival rate was also high in CRACKLE study, which included patients with mostly BSIs and respiratory infection due to CREs treated with CAZ/AVI and the 30-day all-cause mortality was 9%. 24 The satisfying efficacy may stem from following reasons. First, CAZ/AVI is a new β-lactamase inhibitor and has good activities in vitro against OXA-48 and KPC producers, while new β-lactamase inhibitors lack activity against metallo-beta-lactamases. 25 Fortunately, CRKP strains isolated in China were predominantly (more than 70%) producing KPC carbapenemases, especially KPC-2.26–28 Of isolates of K. pneumoniae, 93.8% were susceptible in vitro for CAZ/AVI according to the results from the China Antimicrobial Surveillance Network (CHINET) in 2017. 29 Second, most of the nine patients received combination therapy with meropenem, TGC, or polymyxin. Third and interestingly, all of the nine patients receiving CAZ/AVI were SOT recipients. Mortality rates in SOT recipients were reported ranging from 30% to 50%. 30 However, a recent cohort of 164 SOT recipients across 15 international sites found that while CRE infection usually occurs in early period after transplantation, the 1-year survival rate of patients who developed CRE infection within the first year of transplantation was 72%, probably indicating a good prognosis in those patients. 31
This study gave information about risk factors of mortality and antibiotic options in patients with BSIs due to CRKP from a single center in China. It confirmed the predictive value of Pitt bacteremia score and reminded us the high mortality risk of hematological malignancy patients. However, this study had several limitations. First, it was a retrospective study. Second, the relatively small number of subjects and large number of variables might make the conclusion not robust enough. We considered this problem, but insisted on including patients during a short period of 1-year for the consistency of medical environment and medication choices.
Conclusion
This was a retrospective study among patients with BSIs due to CRKP in a teaching hospital during a 1-year period. Hematological malignancy and Pitt bacteremia score were independent risk factors of death in patients with BSIs due to CRKP, and PMB-based therapy improved survival rate compared with TGC-based therapy.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a research grant from the Natural Science Foundation of Zhejiang Province (LQ18H190001) and a grant from National Natural Science Foundation of China (81971897).