
Abstract
Objectives:
The present systematic review and meta-analysis study aimed to investigate the prevalence of class 1 integrons and their associated antibiotic resistance in uropathogenic Escherichia coli.
Materials and Methods:
A systematic search was conducted to identify studies meeting our inclusion criteria in the Web of Science, PubMed, Embase, Scopus, and Google Scholar electronic databases to the end of July 2019. Finally, 35 articles were selected for data extraction, and meta-analysis was performed using the metaprop program in the STATA, version 11.0, software.
Results:
The pooled prevalence of class 1 integrons was 47% (95% confidence interval [CI]: 40–54), ranging from 6% to 90%. There was significant heterogeneity among the 35 studies (χ2 = 840.37; p < 0.001; I2 = 95.95%). The results of the subgroup analysis based on characterization of patients indicated that pooled prevalence of class 1 integrons was 52% (95% CI: 41–63; n = 14 studies) and 43% (95% CI: 34–54; n = 19 studies) in hospitalized and community patients, respectively. The lowest and highest prevalence of antibiotic resistance was observed for imipenem and ampicillin, respectively. According to the results of Begg's and Egger's tests, we did not find significant publication bias both in the included studies and in the subgroup analysis.
Conclusions:
The results show the high prevalence of class 1 integrons and high level of antibiotic resistance in association with those among uropathogenic E. coli. Moreover, the prevalence of class 1 integrons in Asian countries, as well as hospital-acquired urinary tract infection (UTI), was higher than in other countries and community-acquired UTI.
Introduction
Urinary tract infections (UTIs) are the most prevalent bacterial infections acquired in both hospitals and community settings, particularly in women. 1 Approximately up to 60% of women have at least one UTI during their life history. 2 UTIs are the second prevalent cause of human infections, followed by respiratory tract infections. Escherichia coli as the most common cause of UTIs are responsible for 75–90% of all diagnosed cases associated with both community and hospital origins. 3 The extraintestinal pathogenic E. coli group includes uropathogenic E. coli (UPEC) annually affecting a large portion of the population. 4
Nowadays, the increasing rate of antimicrobial resistance is a considerable public health concern in both developed and developing countries. 5 Increased application of antimicrobial agents is the main factor in the emergence and maintenance of resistant bacteria. Multidrug resistance (MDR) is an alarming problem worldwide, mainly linked to resistance genes existing in mobile genetic elements. Commonly, resistance genes are spread through mobile genetic elements, plasmids, and transposons. Integrons as genetic elements can be carried by these mechanisms.6,7 Although integrons are not mobile by themselves, they can be transferred horizontally. Resistance integrons are elements containing the components of a system for site-specific recombination and distinguishing, capturing, and carrying resistance genes in mobile cassettes. For these reasons, integrons are one of the major contributors to the spread and maintenance of MDR.8–10 Integrons are classified into several classes based on the sequence of their intI genes. Class 1–3 integrons are widely associated with resistance determinants in human clinical isolates. Class 1 integron is primarily associated with capture gene cassettes from a huge pool of resistance genes conferring antibiotic resistance. 10 Moreover, class 1 integron is the most frequently found element in nosocomial and community environments. 11
Since the integron system has the ability to create novel combinations of resistance genes, it may be a dynamic force in the evolution of MDR bacteria. Furthermore, the entire integron element is often contained within other mobile genetic elements such as the plasmid and transposon. The integron elements containing their gene cassettes can disseminate horizontally through bacterial populations. 12
To date, more than 130 different antibiotic resistance gene cassettes have been found within integrons, providing a higher chance of resistance to all the main classes of antibiotics such as aminoglycosides, sulfonamides, macrolides, trimethoprim, quinolones, and antiseptics.13–15
Although several studies only reported local information on the prevalence of integrons among E. coli isolates and the critical role of integrons in antibiotic resistance, there is insufficient global and comprehensive information on the prevalence of these genetic components in UPEC isolates worldwide. The present study aimed to investigate the prevalence of class 1 integrons and their associated antibiotic resistance in UPEC by a systematic review and meta-analysis.
Materials and Methods
Search strategies
The present study was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Data).
A systematic literature search was conducted in the Web of Science, PubMed, Scopus, Embase, and Google Scholar electronic databases. The search was limited to the articles published by international authors from the beginning to the end of July 2019. The following terms, “Integrons” OR “Int1” OR “Integrase” AND “Uropathogenic Escherichia coli” OR “UPEC” AND “Antibiotic resistance” OR “Antibiotic susceptibility” AND “Urinary tract infections” OR “UTI” OR “Urine sample” AND without country restriction, were searched as scientific keywords and phrases in the present survey.
Inclusion and exclusion criteria
To determine articles meeting the inclusion criteria and reduce the risk of error, two reviewers independently screened the databases with the related keywords and reviewed the titles, abstracts, and full texts, and any discrepancies were resolved by consensus. Articles with the following criteria were included in the study: (1) cross-sectional, retrospective, and cohort studies indexed in the Web of Science or PubMed or Scopus database and reporting the prevalence of integron class 1 in E. coli isolates collected from the urine of patients with UTI and (2) articles published worldwide with available English abstracts. Review articles, meta-analysis, or systematic articles, editorials, case report studies, letters to the editors, congress and meeting abstracts, studies with the sample size less than 10 isolates, studies with samples from environmental or nonclinical sources, studies that reported int1 among ESBL and MDR isolates, articles without full text, duplicate publications, and articles with unclear and missing data were excluded.
Quality assessment and data extraction
Five eligibility and quality assessment criteria were retrieved based on the Joanna Briggs Institute guidelines, and any disagreements were resolved by consensus. The following data were extracted for eligible studies: authors' names, publication year, performed time, study location, characterization of the studied population, sample size, prevalence of class 1 integrons, and antibiotic resistance pattern.
Statistical analysis
Analysis of data was conducted using the metaprop program in STATA statistical software, version 11.0 (Stata, College Station, TX).
16
The pooled prevalence of class 1 integron and associated antibiotic resistance with 95% confidence intervals (95% CIs) were estimated through the random effects model. In this meta-analysis, the CIs for proportions were computed using the score method.
17
To study i, ri denotes the number of observations with a certain characteristic, ni is the total number of observations, pi = ri/ni is the observed proportion, k is the total number of studies in the meta-analysis, and 1 − α refers to the selected level of confidence. The confidence limits for proportions for the ith study are computed as follows:
where z is the α/2th percentile of the standard normal distribution.
18
The pooled estimate is then computed using the DerSimonian and Laird method based on the transformed values and their variances.
19
The CIs for the pooled estimate are then computed using the Wald method. The variance-stabilizing transformation of the proportions is defined as follows:
Statistical heterogeneity between studies was calculated using the Cochran Q chi-square test and Cochrane I2. Additionally, the values of 25%, 50%, and 75% for I2 were considered as low, medium, and high levels of heterogeneity, respectively. 20 When the p-value is <0.10 for the Cochran Q chi-square test and the value of Cochrane-I 2 is more than 50%, heterogeneity was considered high. Furthermore, the random effect approach was employed to estimate pooled prevalence. The funnel plot, Begg's rank correlation test, and Egger's weighted regression tests were conducted to evaluate possible publication bias, and any asymmetry appearing in the funnel plot or p < 0.05 in the test used was indicative of statistically significant publication bias. 21 Possible sources of heterogeneity were calculated using a sensitivity analysis, metaregression analysis, and subgroup analysis based on the location of the study (continent and region) and the types of patients. 22 Moreover, a sensitivity analysis was assessed by influence analysis and ignoring of each study and the following that evaluating the estimated pooled prevalence in the absence of removed studies. In addition, the confounding effect of possible confounders such as the time of the study (performed years) was evaluated by conducting metaregression analyses.
Results
Database search and characterization of studies
Our comprehensive search identified 35 studies with eligibility criteria subjected to meta-analysis. Figure 1 presents the searching procedure to select eligible studies. Of the 35 included studies, 19 and 14 studies reported the prevalence of class 1 integrons from community and hospitalized patients, respectively. Of the 35 included studies, 8 studies reported the prevalence of antibiotic resistance associated with class 1 integrons. These studies used the disk agar diffusion method for antimicrobial susceptibility testing on UPEC isolates according to CLSI guidelines. 23 Table 1 shows the full characteristics of the included studies.
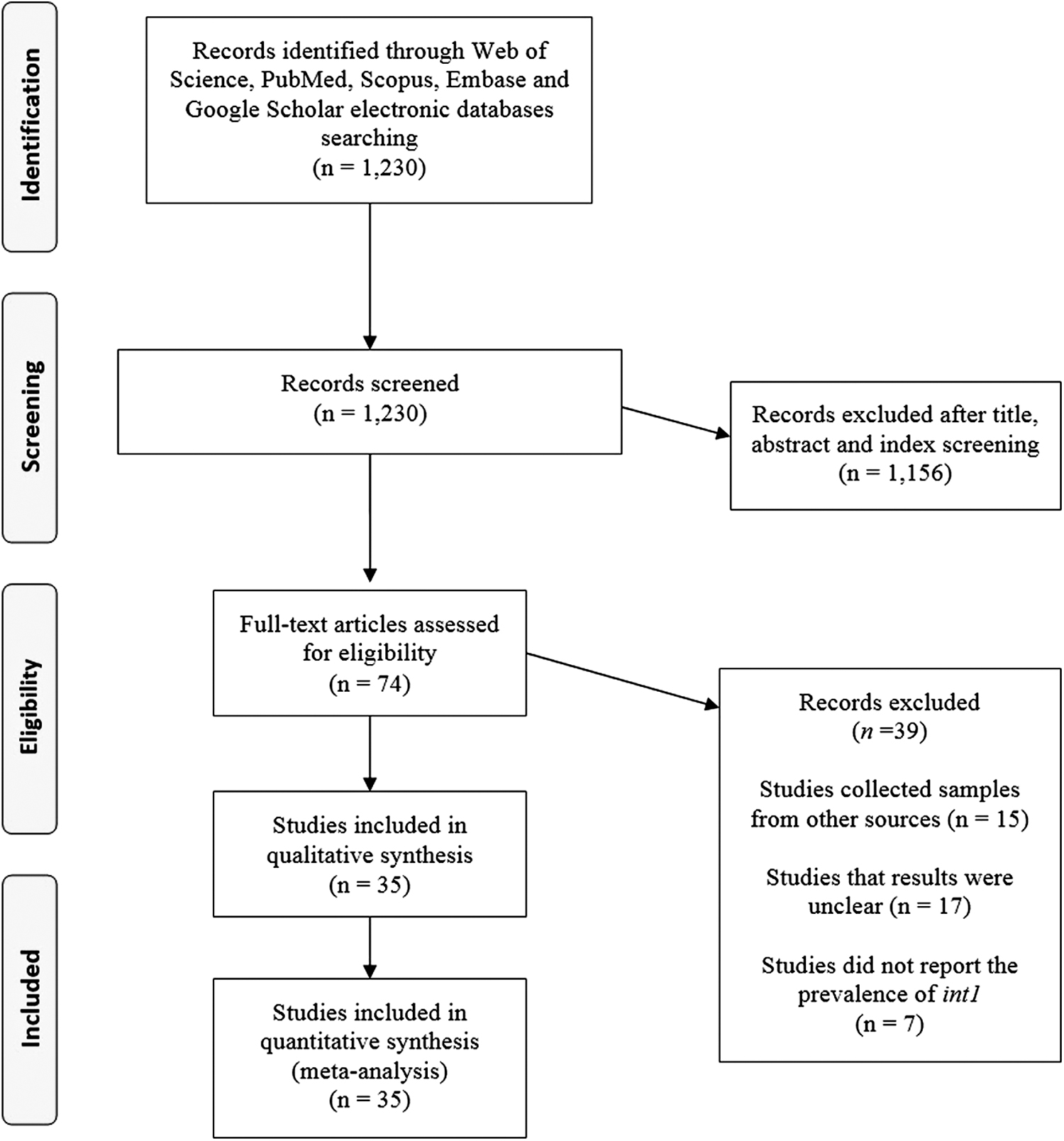
Flowchart of the study selection for inclusion in the systematic review.
The Main Characteristics of Studies Included in the Meta-Analysis
Prevalence of class 1 integrons
Thirty-five studies investigated the class 1 integrons among UPEC isolates from patients suffering from UTI.11–15,24–53 From those studies, the pooled prevalence of class 1 integrons was 47% (95% CI: 40–54) (Fig. 2). There was significant heterogeneity among the 35 studies (χ 2 = 840.37; p < 0.001; I2 = 95.95%). The funnel plot for publication bias did not show any evidence of asymmetry (Fig. 3). Additionally, Begg's and Egger's tests were conducted to quantitatively evaluate the publication bias. According to the results of Begg's (z = 0.21, p = 0.83) and Egger's tests (t = 0.95, p = 0.34), there was no significant publication bias (Fig. 3).
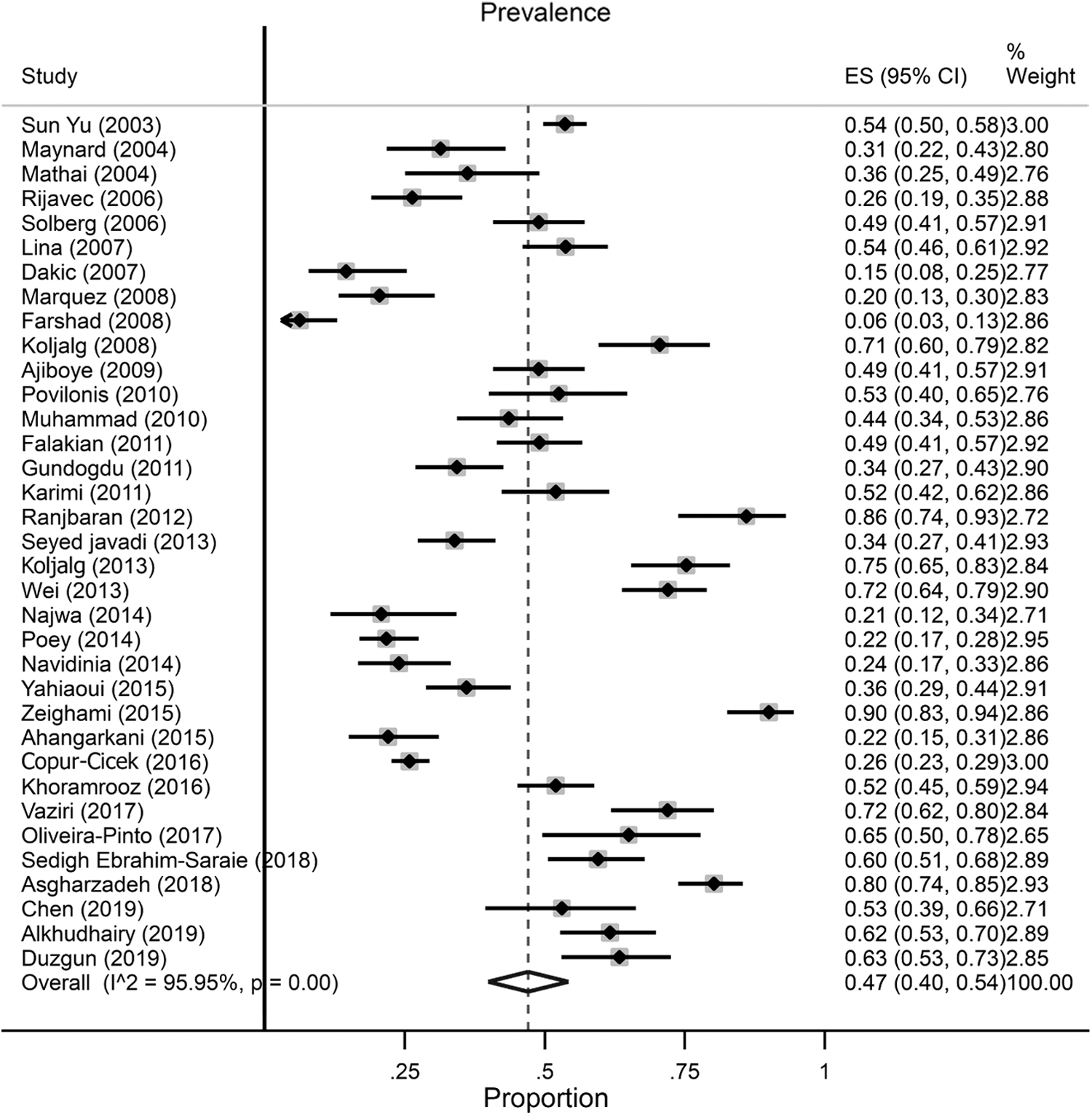
Forest plot of the meta-analysis of class 1 integron prevalence among UPEC isolates. UPEC, uropathogenic Escherichia coli.
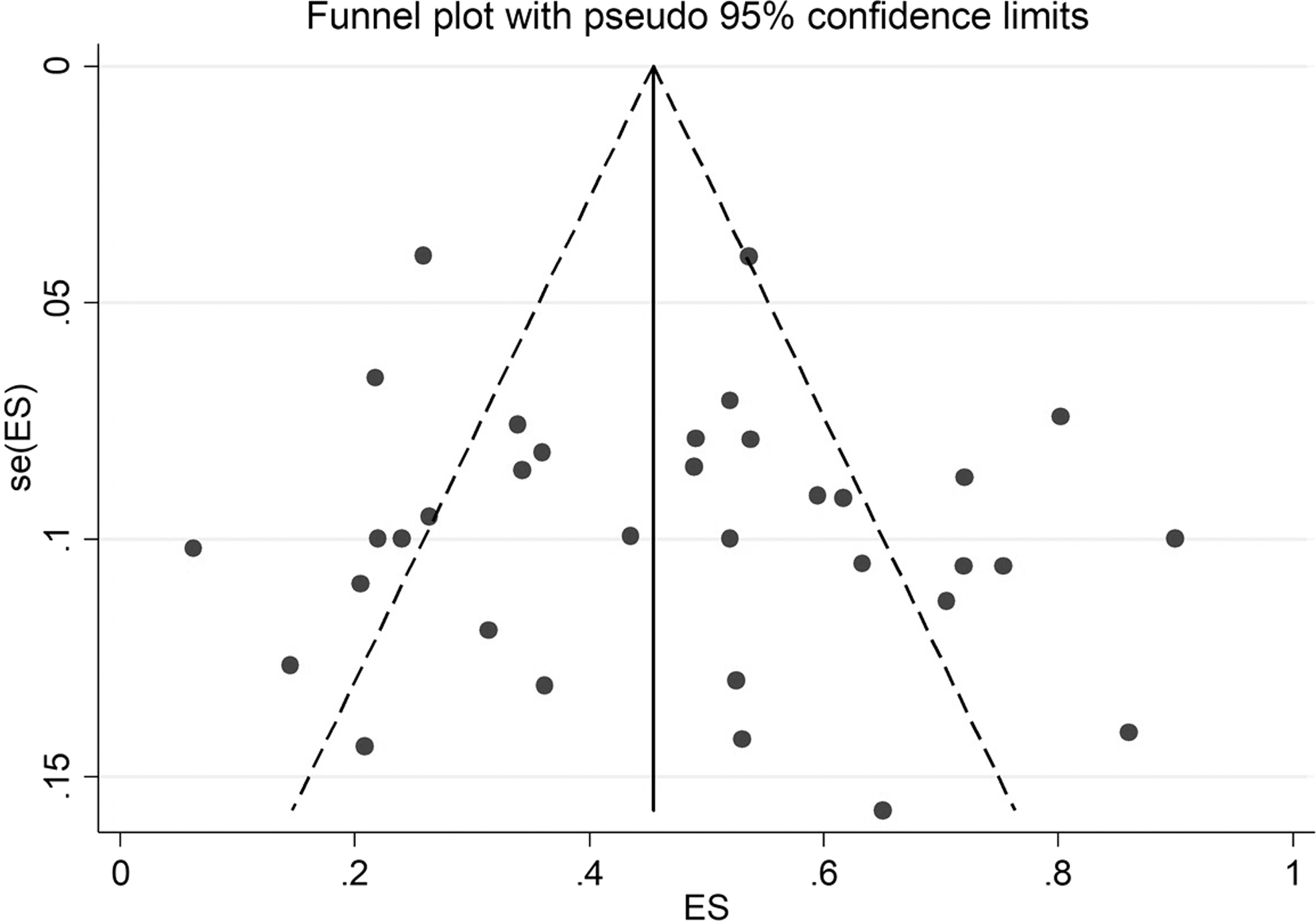
Funnel plot for evaluation of publication bias.
Subgroup analysis of prevalence of class 1 integrons
The subgroup analysis results based on continent indicated that Asian countries had the highest rate of class 1 integrons with 53% (95% CI: 44–62), followed by 44% (95% CI: 34–54), 43% (95% CI: 24–63), 32% (95% CI: 26–39), 29% (95% CI: 23–35), and 27% (95% CI: 22–33) in North America, Europe, Africa, Australia, and South America, respectively (Fig. 4). In addition, when data from Asian countries were separately analyzed, results showed that the pooled prevalence of class 1 integrons was 60% (95% CI: 47–73), 54% (95% CI: 40–67), and 45% (95% CI: 36–56) in East Asia, the Middle East, and South Asia, respectively. Studies conducted in the Middle East (χ 2 = 409.20; p < 0.00; I2 = 96.82%) and Europe (χ 2 = 151.29; p < 0.001; I2 = 96.70%) showed significant heterogeneity based on the Q statistic and I2 (Supplementary Fig. S1). The subgroup analysis results based on the source of infection indicated that the pooled prevalence of class 1 integrons was 52% (95% CI: 41–63; n = 14 studies) and 43% (95% CI: 34–54; n = 19 studies) in hospitalized and community-associated patients, respectively (Fig. 5).
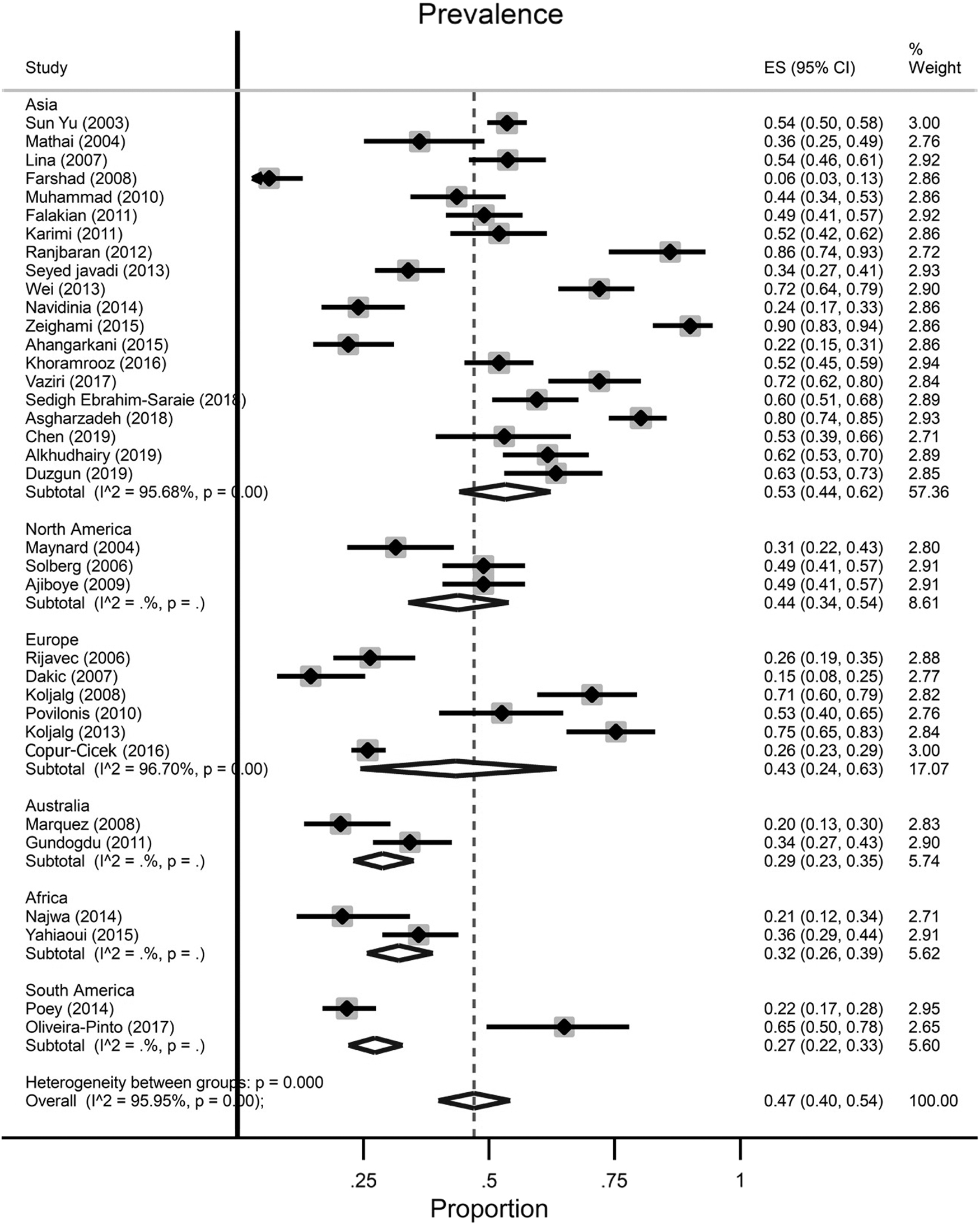
Forest plots of the overall prevalence of class 1 integrons based on the continent.
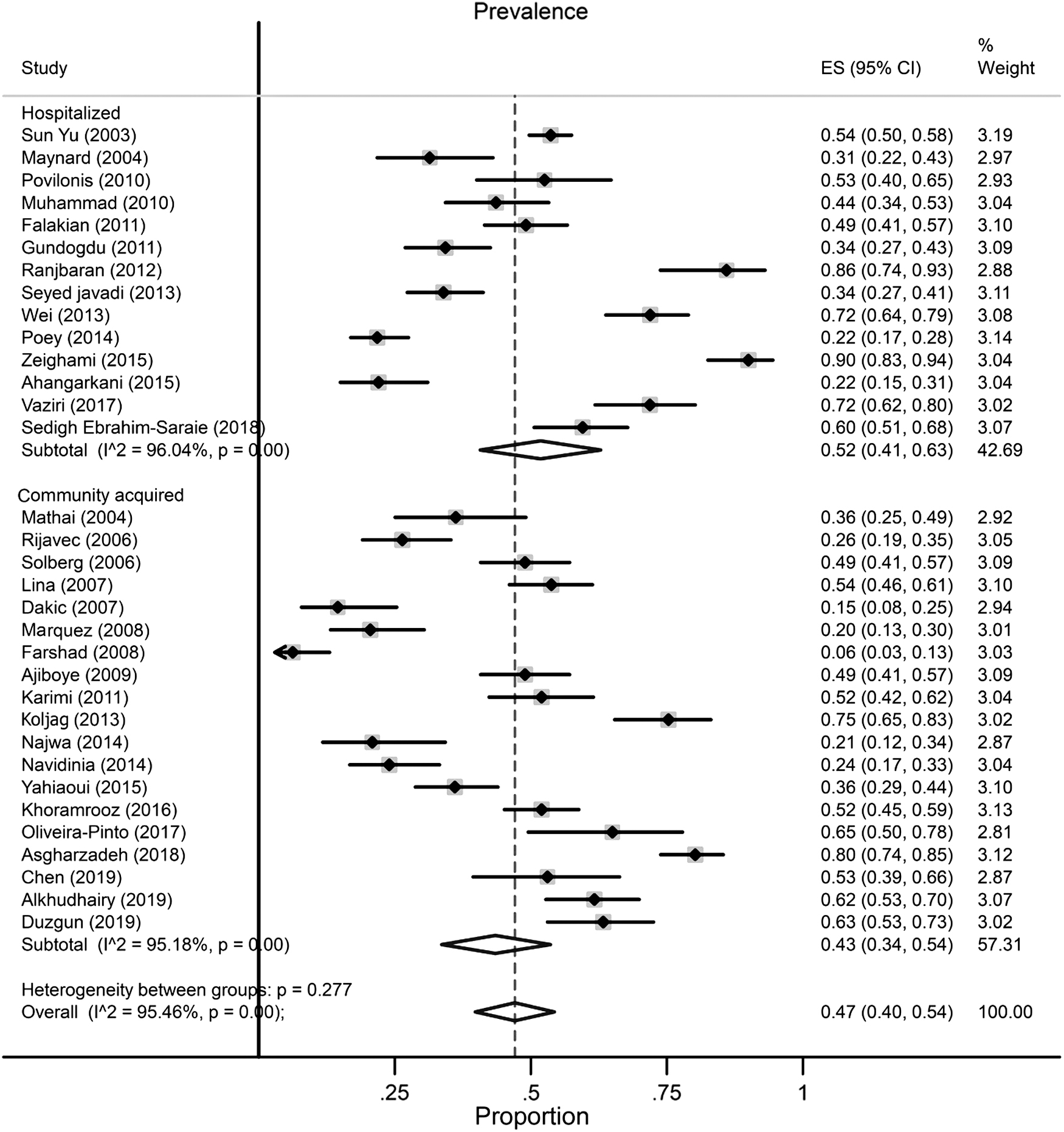
Forest plots of the prevalence of class 1 integrons based on the source of infection.
Prevalence of antibiotic resistance
According to the antibiotic resistance pattern, ampicillin had the highest antibiotic resistance rate at 85% (95% CI: 78–92; I2 = 59.55%; n = 6 studies), followed by tetracycline at 58% (95% CI: 48–68; I2 = 64.99%; n = 5 studies), while imipenem and amikacin were the most effective antibiotics with resistance rates of 5% (95% CI: 0–12; I2 = 85.46%; n = 6 studies) and 12% (95% CI: 1–29; I2 = 94.37%; n = 5 studies), respectively (Supplementary Table S1). Supplementary Table S1 and Supplementary Figure S2 show the estimated prevalence of different antibiotic resistance profiles in integron-positive E. coli strains. According to heterogeneity tests, significant heterogeneity was indicated.
Sensitivity analyses and metaregression
Metaregression results indicated that the prevalence of class 1 integrons among UPEC isolates was not significantly associated with year, coefficients: 0.14436 (95% CI: 0.0009254–0.029798, p = 0.06) (Fig. 6). Furthermore, no significant increasing trend was observed over time on the estimated pooled prevalence of class 1 integrons in the included studies. Moreover, Fig. 6 shows results of the influence analysis, demonstrating that none of the studies affect the estimated pooled prevalence. In addition, we excluded each study and examined the outcome. The sensitivity analyses also showed no significant change in estimated pooled prevalence in meta-analysis results after excluding studies with relatively lower quality (Supplementary Fig. S3).

Metaregression of the log-event rates by year.
Discussion
The extensive and inappropriate use of antibiotics, followed by the transmission of resistance genes through plasmids, transposons, and integrons, is an important factor in the emergence of MDR isolates.54,55 These determinants particularly contribute to horizontal transmission of genes among clinical isolates of E. coli and other Enterobacteriaceae. 56 To the best of our knowledge, this is the first comprehensive meta-analysis investigating the prevalence of class 1 integrons in E. coli recovered from UTI patients worldwide.
In the present review, the prevalence of class 1 integrons in UPEC isolates investigated from urine samples varied from 15% to 90% in international studies.15,53 Additionally, the pooled prevalence of class 1 integrons was reported as 47%. These results strongly indicate wide dissemination of class 1 integrons in UPEC, which may decrease the efficiency of antimicrobial agents. Several studies have revealed the high occurrence of class 1 integrons among Enterobacteriaceae.57,58 Among the studies, contrary to our results, Karami et al., in their meta-analysis study conducted in 2019 in Iran, reported the prevalence of class 1 integrons in 60% of Klebsiella pneumoniae isolates. 58 In another study in Iran, Pormohammad et al. indicated that the prevalence of integron classes in Gram-negative clinical isolates was 41%, being highly consistent with our results in E. coli. 59 Contrary to our results, Zeeshan Khan et al. showed that 79% of MDR E. coli harbored class 1 integrons. 60 Oliveira-Pinto et al. also investigated the presence of class 1 integrons in a collection of E. coli isolates obtained from healthy subjects and patients with UTI. 46 Analysis of the class 1 integron carriage revealed considerable variation in the incidence of commensal E. coli (11.9%) and UPEC (65%) populations. 46 In addition, in one study investigating the prevalence of class 1 integrons in fecal E. coli strains isolated from children with diarrhea and healthy mothers, the findings indicated that 37.3% of isolates harbored class 1 integrons. 61
To date, several studies have reported a variable prevalence of class 1 integrons among the E. coli strains obtained from the environment and animal sources. In this regard, Tajbakhsh et al. investigated the prevalence of class 1 integrons among E. coli strains isolated from aquaculture water of fish fields in Iran. The results demonstrated that 29.7% of isolates carried class 1 integrons. 62 Zhang et al. also examined the prevalence of integrons among E. coli isolates obtained from animal sources, in which class 1 integrons were found in 81% of strains. 63 The data, along with those found in the current study, suggest that class 1 integrons are highly widespread in clinical isolates and higher than the rate reported in fecal or commensal E. coli.
According to these findings, there is considerable discrepancy in the prevalence of class 1 integrons, and the reasons for this discrepancy may be related to the origin of isolates, characteristics of the type studied, and geographical distribution. Moreover, these factors may be considered a source of heterogeneity. We performed subgroup analysis of some factors that confound the assessment (types of patients and geographical distribution based on continent and region) and metaregression for controlling this heterogeneity.
The geographical distribution of UPEC containing class 1 integrons is variable in different regions of the world. Accordingly, the subgroup analysis of the geographical distribution indicated that the predominant prevalence of class 1 integrons was a frequency of 54% in Asian countries and 44% in North American countries. Furthermore, among Asian countries, studies conducted in East Asia and the Middle East reported a high prevalence of integrons; this high frequency was more effective in development of antibiotic resistance and emergence of the MDR strain. An evaluation of our results showed that the rate of integron-carrying E. coli was more frequent in Asia than in other regions.
Moreover, based on our findings, the high prevalence of the integron-positive strain was reported among isolates obtained from hospital-acquired UTI rather than community-acquired UTI. Thus, attention to standard principles and accomplishment of infection control against integron-containing isolates should be part of the national surveillance program in health care settings of these countries and populations. In addition, in the assessment of historical changes in the prevalence of class 1 integrons, a significantly increased rate of integrons was not observed in our studies.
Antibiotic resistance among integron-positive isolates was assessed among the included studies; therefore, we analyzed these patterns in more detail. According to the analysis of the antibiotic resistance pattern, ampicillin had the highest antibiotic resistance rate at 85%, followed by tetracycline with 58% resistance, while the pooled prevalence of imipenem and amikacin resistance was 5% and 12%, respectively. Based on the heterogeneity test, all antibiotics used had significant heterogeneity. Accordingly, among the investigated studies, considerable antibiotic resistance was observed. For example, the pool prevalence of SXT resistance was 62%, ranging from 6% to 100%, or of nitrofurantoin was ∼44%, ranging from 12% to 100%. This difference and heterogeneity may be owing to the different studied populations (inpatients and outpatients), the source of the sample, and policies of antibiotic stewardship guidelines.
To investigate the sources of heterogeneity, subgroup, metaregression, and sensitivity analyses were surveyed. On the contrary, to interpret outcomes of the reports, publication bias and heterogeneity should also be considered. In one study conducted by Pormohammad et al., the prevalence of antibiotic resistance in E. coli strains isolated from humans, animals, food, and the environment was investigated. 59 Their results indicated that colistin had the lowest prevalence, with a 0.8% rate, and amoxicillin had the highest prevalence, with a 70.5% rate (95% CI: 57.5–81), in E. coli strains isolated from humans. 59 The emergence of imipenem resistance among integron-positive isolates is at the high-risk level, which can be alarming for horizontal gene transfer to others, decreasing the efficiency of the last appropriate drug choice in E. coli isolates.
The limitations of our systematic review include the following cases: first, most of the available studies were limited to few regions, and results may not reflect the actual epidemiology in the world, especially at the continental level. Second, there was a lack of antibiotic susceptibility patterns among integron-positive isolate data in the included studies. Third, heterogeneity was reported among the included studies; therefore, we performed a subgroup analysis and metaregression. However, due to different sample sizes of studies and significant heterogeneity, the results should be interpreted with caution.
In conclusion, the results indicated the high prevalence of integron-positive isolates and the high level of antibiotic resistance in association with those in the urine source. Moreover, the prevalence of class 1 integrons and hospital-acquired UTI was higher in Asian countries than in other countries and populations. Thus, continuous and appropriate surveillance of hospital-associated infections, observance and evaluation of antibiotic sensitivity patterns, and development of antimicrobial stewardship programs are necessary to avoid the greater spread of these elements among bacteria.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.