
Abstract
Klebsiella pneumoniae is an opportunistic bacterial pathogen most commonly associated with nosocomial infections, especially in intensive care unit (ICU) patients. Routine surveillance cultures for carbapenemase-producing Enterobacteriaceae have become a common practice for hospital infection prevention. The objective of this study was to investigate the genetic relatedness of carbapenem-resistant K. pneumoniae carrying blaNDM gene across multilocus sequence typing (MLST) scheme. Surveillance rectal swabs from 4,463 ICU patients admitted to the Rio de Janeiro hospital (March 2016–2017) were screened on CHROMagar mSuperCARBA. Of these, 631 isolates were subjected to VITEK 2 system for phenotypic microbial identification and antibiotic susceptibility testing. Out of 631 isolates, 108 were identified as K. pneumoniae, 103 of which were confirmed by PCR of 16S–23S rDNA internal transcribed spacer (ITS). Eleven blaNDM-positive isolates were subsequently screened for blaKPC, blaBKC, blaIMP, blaVIM, blaSPM, blaOXA-48, and mcr-1-8 genes. Twenty-seven percent (3/11) revealed co-occurrence with KPC, OXA-48, and VIM, 46% (5/11) with KPC and VIM, and 18% (2/11) with VIM type. No strains harbored the blaBKC, blaSPM, blaIMP, and mcr-1 to 8 resistance genes. All 11 isolates were resistant to β-lactams, ciprofloxacin 90%, tigecycline 82%, gentamicin 73%, and amikacin 18%, and were classified as multidrug resistant (MDR), extensively drug resistant (XDR), and pandrug resistant (PDR). Molecular epidemiology data based on MLST revealed 11 different STs, 8 of which were novel and 3 were previously described. Six out of the eight new STs were associated with MDR and PDR strains and two clonal complexes were reported, including CC258 and CC15. The coexistence of NDM-producing K. pneumoniae and other carbapenemase has been frequently described worldwide. Moreover, we report for the first time K. pneumoniae co-harboring up to four carbapenemases from active surveillance cultures.
Introduction
The presence of carbapenem-resistant Acinetobacter baumannii, carbapenem-resistant Pseudomonas aeruginosa, and mainly carbapenem-resistant Enterobacteriaceae (CRE) in health care facilities, and especially in the intensive care unit (ICU), constitutes a constant public health threat.1–3 The intestinal tract represents an important reservoir for nosocomial pathogens, including CRE. Routine surveillance cultures for gastrointestinal screen to CRE have become a common practice and essential part of hospital infection prevention and control programs in many countries.4–6 Therefore, intestinal carrier identification of multidrug-resistant (MDR) bacteria can be crucial to decide upon the adoption of contact precautions and other interventions to limit the spread of this pathogen.7–10
Currently, MDR Klebsiella pneumoniae (MDR-KP) is considered one of the microorganisms most associated with nosocomial infections, especially in patients admitted to ICU. 11 It has shown high rates of resistance to a broad spectrum of antimicrobials, including β-lactams, fluoroquinolones, and aminoglycosides.12,13 Some studies have revealed the relationship of colonized patients with subsequent infection with MDR-KP.14–17 Recently, Gorrie et al. revealed that K. pneumoniae is a fairly common component of the human gut microbiota (6%), and may have an impact on the health of ICU patients. Among 27 infections with this micro-organism diagnosed in the ICU, 48% occurred in patients considered previously colonized. 18 Furthermore, the MDR organism transmission between patients is an important mechanism for outbreaks that emerge in hospitals, especially in ICUs.1,19,20 Thus, active surveillance is considered an important approach in the prevention and control of antimicrobial resistance programs, enabling early detection of emerging pathogens and epidemiological characteristic monitoring.10,21
The K. pneumoniae carbapenemase (KPC; type A), Verona integron-encoded metallo-β-lactamase (VIM; type B), the New Delhi metallo-β-lactamase (NDM; type B), and the oxacillinase-48 (OXA; type D carbapenemase) are the most frequent carbapenemases with worldwide expansion. 22 The CRE harboring the blaKPC-2 gene is among the most frequently isolated pathogen. This allele is usually carried by mobile genetic elements such as plasmids and transposons, which may be associated with other carbapenemase genes.20,23–26 This way, it can spread horizontally between pathogenic and saprophytic bacteria, increasing the antibiotic resistance reservoir in both environmental and clinical microbiome. 27 P. aeruginosa was the first micro-organism to carry VIM gene, but has quickly spread to Enterobacteriaceae.28–31 VIM-encoding CRE is endemic in Greece and Italy, and their emergence in the United States may be associated with travel and hospitalization in these countries.26,32,33 To date, 28 NDM enzyme variants have been found in Enterobacteriaceae, Acinetobacter spp., and P. aeruginosa from several countries34,35 This carbapenemase has a greater ability to degrade penicillins, cephalosporins, and a few of the carbapenems compared to VIM, and a higher propagation potential than KPC.36,37
Several reports have been suggesting the relationship of multidrug resistance with molecular epidemiological data based on multilocus sequence typing (MLST).38–40 K. pneumoniae ST258 is the most common carbapenem-resistant ST type in the United States and Greece. It has been reported in >25 countries, including KPC epidemic countries such as Northeastern United States, Argentina, Brazil, Colombia, Eastern China, Greece, Israel, Italy, Poland, and Puerto Rico.41,42 In addition, it is responsible for >77% of the outbreaks in the United States and 90% of all carbapenem-resistant K. pneumoniae (CRKP) infections in Israel.43,44 Moreover, ST11 and ST437 are described as prevalent K. pneumoniae clones in Brazil. 45
This study aimed to investigate the genetic relatedness of NDM-producing K. pneumoniae co-occurring with VIM, KPC, and OXA-48 enzymes in active surveillance cultures among patients admitted to ICU across the MLST scheme.
Materials and Methods
Study setting
Rectal swabs of 4,463 patients admitted to the ICU of Rio de Janeiro Hospital from March 2016 to 2017 were screened. This hospital has 213 beds, receives 6,649 people per year, and is a reference for medium and high complexity care, with emphasis on several specialties. This study was approved by the Research Ethics Committee of the Oswaldo Cruz Foundation (Fiocruz) (1.787.832).
CRKP identification and antimicrobial susceptibility
The rectal screening samples from surveillance cultures were seeded in CHROMagar mSuperCARBA and colonies suggestive of K. pneumoniae (metallic blue) were subjected to Vitek II for phenotypic identification and antimicrobial susceptibility. Subsequently, genomic DNA was obtained using the DNeasy Blood & Tissue Kit (QIAGEN®), according to manufacturer's instructions. The identity of isolates was confirmed by K. pneumoniae 16S–23S ribosomal intergenic region-specific PCR analysis. 31
Resistance genes profiles
Initially, the CRKP isolates were screened by PCR for the presence of blaNDM gene as previously described. 46 Subsequently, the NDM-positive isolates were screened for genes that encode other carbapenemases (blaKPC, blaBKC, blaIMP, blaVIM, blaSPM, and blaOXA-48) and mobile colistin resistance (mcr alleles 1–8) also as previously described.47–53 The strains K. pneumoniae ATCC BAA1705 (blaKPC), K. pneumoniae CCBH 24217 (blaNDM), K. pneumoniae CCBH 24264 (blaOXA-48), P. aeruginosa CCBH 20008 (blaVIM), P. aeruginosa CCBH 25732 (blaSPM), P. aeruginosa CCBH 24208 (blaIMP), Escherichia coli BL21+pET-26BKC-1 (blaBKC), and E. coli CCBH 23595 (mcr-1) were used as positive controls.
Multilocus sequence type analysis
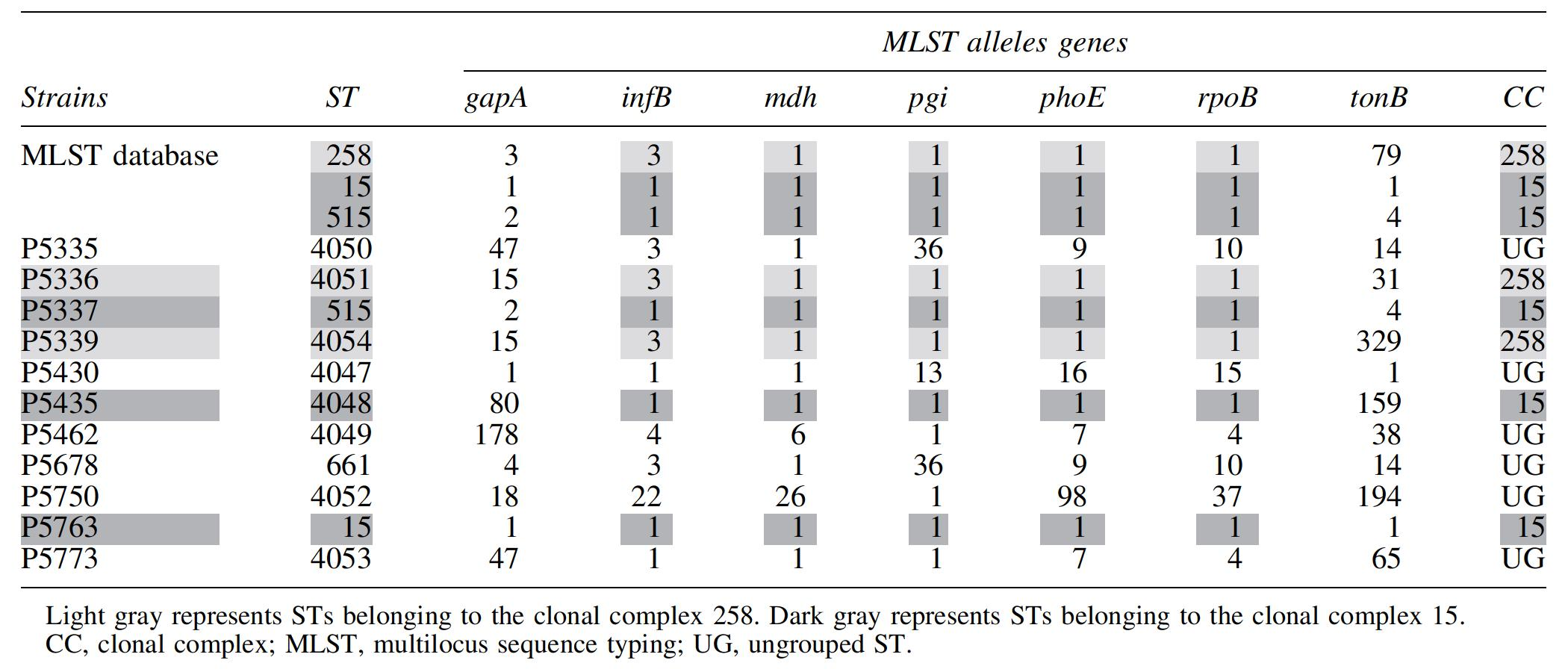
NDM-positive strain genotypic analysis was investigated according to the Klebsiella Sequence Typing by Pasteur Institute MLST Database. Housekeeping gene (gapA, infB, mdh, pgi, phoE, rpoB, and tonB) amplifications were performed as previously described and sequenced with fluorescent terminators (BigDye; Applied Biosystems, Foster City, CA) on an Applied Biosystems ABI Prism 3730 Genetic Analyzer in duplicate39. The sequences were submitted to the MLST database to determine the allelic numbers and ST. Novel STs were assigned when necessary.
Results
Antimicrobial susceptibility, resistance genes, and MLST profiles
Out of the 631 colonies suggestive of CRKP, 108 isolates were phenotypically identified as carbapenemase-producing K. pneumoniae (99% identified by the Vitek II), 103 of these were confirmed as K. pneumoniae by 16S–23S rDNA internal transcribed spacer PCR. These 103 isolates showed resistance to all β-lactam antimicrobials (tazobactam/piperacillin, sulbactam/amoxicillin, cefepime, cefoxitin, ceftazidime, ceftriaxone, and cefuroxime), including carbapenems (ertapenem, imipenem, and meropenem), suggesting carbapenemase production. Ninety-four percent (97/103) of the isolates were resistant to ciprofloxacin, 84% (87/103) to tigecycline, 77% (79/103) to gentamicin, 62% (64/103) to amikacin, and 35% (36/103) to colistin.
Among the 103 isolates, 11% (11/103) showed the NDM gene and were grouped in three resistance profiles and four resistance genotypes (Table 1). Nine isolates of K. pneumoniae were classified as MDR, one as extensively drug resistant (XDR) and one as pandrug resistant (PDR) with high percentages of β-lactam resistance, including carbapenems, as well as ciprofloxacin 90% (10/11), tigecycline 82% (9/11), gentamicin 73% (8/11), and amikacin 18% (2/11) (Table 1). Furthermore, two isolates (P5335 and P5336) exhibited resistance to colistin, but did not carry mcr-related genes. It is worthy to note that one of these isolates (P5335) was resistant to all antimicrobials analyzed. Twenty-seven percent (3/11) of NDM-harboring K. pneumoniae revealed co-occurrence with KPC, OXA-48, and VIM type, 46% (5/11) with KPC and VIM, and 18% (2/11) with VIM. The blaBKC, blaSPM, and blaIMP genes were not detected.
Characterization of NDM-Producing Klebsiella pneumoniae Strains
New ST.
AK, amikacin; CIP, ciprofloxacin; COL, colistin; GEN, gentamicin; MDR, multidrug resistant; NI, not informed; PDR, pandrug resistant;
MLST analysis of the 11 isolates harboring the blaNDM gene revealed 11 different STs, 8 being (ST4047, ST4048, ST4049, ST4050, ST4051, ST4052, ST4053, and ST4054) novel and 3 (ST15, ST515, and ST661) previously described (Table 1). Two clonal complexes (CCs) were found in this study, including CC258 with two strains and CC15 with three strains. CC grouping was based on two different ST sharing at least 5 identical alleles (Table 2 and Fig. 1).

ST distribution among geographic location. CC, clonal complex. Color images are available online.
Clonal Complex Grouping Proposition of Strains Sharing Five or More Alleles Among ST
Discussion
Gastrointestinal colonization is considered a significant reservoir of CRKP, which has been considered a major public health problem. For this purpose, it is necessary to conduct active surveillance cultures in health centers, especially in ICU patients.18,54 In addition, CRKP is an important bacterial pathogen responsible for hospital outbreaks worldwide and has been emerging in Brazilian hospitals. 55
Our study showed that all 11 NDM-producing K. pneumoniae were resistant to other antimicrobial classes, including gentamicin, ciprofloxacin, and tigecycline. The high rates of aminoglycoside resistance exhibited by K. pneumoniae can be attributed to the excessive use of gentamicin, beyond the possibility of the presence of aac(3)-II gene in the same mobile genetic element carrying the carbapenemase genes. 56 In contrast, another study reported a CRKP susceptible to different aminoglycosides, such as gentamicin, 57 which could be related to the stability of plasmids in the presence or absence of selective pressure.58,59 Regarding the treatment, the use of gentamicin alone or in combination with tigecycline has been used to reduce mortality from sepsis caused by CRE. 60 Of note, in our study, the high percentages of CRKP were resistant to both gentamicin and tigecycline.
During the past decades, carbapenem resistance among K. pneumoniae has been typically caused by the emergence of transmissible carbapenemases, such as KPC and NDM. The NDM especially comprises one of the most rapidly growing group of metallo-β-lactamases.36,61 They have been increasingly detected in different countries, suggesting a worldwide dissemination.56,61 Thus, carbapenem antimicrobials are becoming increasingly ineffective and only a few therapeutic options are available, such as colistin. 62
According to Nordmann et al., the majority of NDM-producing bacteria also carry a diversity of other resistance mechanisms, including ESBLs (especially CTX-M-15) and different carbapenemases (e.g., OXA-48, VIM, and KPC types). 63 The coexistence phenomenon of multidrug resistance determinants in a single strain has become commonplace.64–66 On the other hand, another study that evaluated the genetic relationship and molecular determinants of carbapenem resistance in clinical strains, revealed that none of the 100 CRKP harbored either KPC or VIM genes. Furthermore, they exhibited a prevalence of OXA-48 and NDM, as well as an increase in the colistin resistance rate. 67 The existence of at least two carbapenemase genes in CRKP also has been reported worldwide, including KPC and VIM in Italy,1,26,68 KPC-2 and VIM-24 in Colombia, 69 NDM-1 and KPC-2 in Brazil, 70 and NDM-1 and OXA-181 in Singapore. 71 Other studies generally characterize the CRKP carrying a single carbapenemase. However, we report for the first time K. pneumoniae co-harboring up to four carbapenemase genes (NDM, KPC, OXA-48, and VIM) from surveillance cultures belonging to ST515.
Molecular epidemiology data based on MLST showed the variety of K. pneumoniae ST associated with drug resistance genes, such as ST258, which is the most common carbapenem-resistant genotype in the United States, Brazil, Italy, Norway, and Greece55,72,73 (Fig. 1). A study carried out in Russia also showed that ST340 was associated with K. pneumoniae producing NDM. 74 Meanwhile, recent evidence showed that global epidemiology is changing, with the rise of new lineages such as KpV_S_1 and KpV_S_2 isolates belonging to ST661 and ST307, respectively. Both STs have been recently reported as responsible for outbreaks in several European countries. Furthermore, the detection of blaVIM-1 gene in nonpredominant K. pneumoniae clones in a hospital setting is strong evidence of the changing epidemiology in Italy. 75 In Argentina, ST258 is no longer the absolute clone among KPC-Kp isolates with the rise of more virulent lineages such as the hypermucoviscous ST25 and the emergence of the high-risk clone ST307. 76
In this study, the 11 NDM-producing K. pneumoniae were grouped into 11 different STs, with 8 new and 3 previously described (ST515, ST661, and ST15). Six of the eight new STs were associated with MDR strains, in addition to a PDR isolate belonging to ST4050. According to the MLST database, ST661 is a rare lineage isolated only in China and United States, and has been implicated in an outbreak in the United Kingdom, which involved both the clonal spread of a KPC-producing K. pneumoniae and the dissemination of pKpQIL-D2-KPC-2 plasmid. 77 In turn, ST15 is a worldwide spread genotype, but has never been reported as a source of hospital outbreaks of CRKP. As previously reported,78–81 the ST15 strain isolated in this study presented an MDR profile associated with VIM and NDM genes, suggesting a high capacity of horizontal transfer of resistance genes. 82 Indeed, whole-genome sequencing of K. pneumoniae ST15 strains revealed high antimicrobial resistance sharing a common ancestor with 140 globally disseminated K. pneumoniae strains. 83 Another genotype found in this study, ST515, has been reported in Poland and Vietnam as a sporadic infection agent. It is worthy of note that ST515 and ST15 share 5 MLST alleles (Table 2), suggesting that these two STs may be grouped into the same CC15 that is settling among healthy carriers and patients either in the hospital environment or outside health facilities. The STs 4051 and 4054 are closely related to antimicrobial resistance-associated ST258, sharing 5 alleles, and could be grouped into CC258 (Table 2). Strains from these two STs harbored blaKPC, blaNDM, and blaVIM genes, besides high resistance to β-lactams, ciprofloxacin, tigecycline, and gentamicin (Table 1).
Conclusion
In conclusion, our data reveal new multiresistant CRKP clones from surveillance cultures that may represent a concern for health authorities regarding the spread of antibiotic resistance. Notably, of the eight new STs described in this study, two are resistant to colistin with no mcr allele (1 to 8), but showing co-production of KPC, NDM, and VIM. Indeed, the presence of NDM in the 11 different STs may reflect the possibility of plasmid transfer carrying several carbapenemases genes, as has been reported worldwide. This event can have serious consequences for public health, leading to an increased spread of antimicrobial genes and MDR microorganisms turning treatment against bacterial pathogens difficult.
The active surveillance culture program could be considered an essential approach to fight the threat of antimicrobial resistance. Moreover, the disclosure of our data must be shared both with the scientific community and with the main stakeholders, including the population and government decision makers.
Footnotes
Acknowledgments
We thank the hospital microbiology laboratory staff for providing the K. pneumoniae strain surveillance data. This publication made use of the Multi Locus Sequence Typing website sited at the University of Oxford. The development of this site has been funded by the Welcome Trust. The authors are grateful to the Sequencing core “Plataforma Genômica de Sequenciamento de DNA/PDTIS-FIOCRUZ.”
Disclosure Statement
No competing financial interests exist.
Funding Information
We also thank INCQS/Fiocruz and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for financial support.