
Abstract
Background:
Prevalence of extended-spectrum beta-lactamase-producing Escherichia coli (ESBL-E. coli) is increasing worldwide, but greatly varies geographically. We compared the prevalence of ESBL-E. coli infections at four distinct health care facilities in San Francisco, California.
Methods:
Antimicrobial susceptibility reports were obtained for E. coli isolates from (1) a county hospital, (2) a public skilled nursing facility, (3) a university hospital, and (4) a Veterans Affairs (VA) Medical Center. We compared change in frequency of ESBL-E. coli and antimicrobial resistance to trimethoprim-sulfamethoxazole between 2012 and 2018.
Results:
From 2012 to 2018, frequency of ESBL-E. coli increased in urine and nonurine isolates from the county hospital (urine: 1.1% per year, 95% confidence interval [CI]: 0.5–1.6, p < 0.01; nonurine: 1.9% per year, 95% CI: 0.9–2.9, p < 0.01) and in urine isolates from the VA hospital (0.9% per year, 95% CI: 0.3–1.4, p < 0.01). The frequency of trimethoprim-sulfamethoxazole resistance fluctuated in all facilities.
Conclusions:
At the skilled nursing facility, the prevalence of ESBL-E. coli was highest, but remained stable over time, while the prevalence of ESBL-E. coli increased among urine and nonurine isolates at the county hospital and urine isolates at the VA hospital. The temporal trend of ESBL-E. coli infections, even within one city, varied by health care facility.
Introduction
E
There are multiple definitions for ESBL. 1 Broadly, the phenotypic definition of ESBL is resistance to third-generation cephalosporins and aztreonam, but inhibition by clavulanic acid. 1 The Clinical and Laboratory Standards Institute (CLSI) changed its guidelines for identification of ESBL and no longer recommends confirmatory testing for ESBL. 14 Although ESBL-E. coli first appeared in long-term care facilities, community-acquired ESBL-E. coli infections have been increasing over the last decade worldwide.7,15–19 Geographic differences in prevalence of ESBL-E. coli have been recognized, which may reflect differences in local antibiotic prescribing practices, antibiotic use, and types of at-risk patients studied. These differences have been demonstrated among inpatient and outpatient settings within the same city.20,21 Since extended-spectrum cephalosporins are generally not used to treat community-onset infections (e.g., UTI), the increasing trend in community-onset ESBL-E. coli infections may reflect a “spillover” effect from health care institutions. In addition, fluoroquinolones, used to treat complicated UTIs among other infections, can co-select for ESBL- E. coli; 22 trends in treatment with fluoroquinolones could affect trends in reported ESBL production. Moreover, skilled nursing facilities have been identified as possible reservoirs for ESBL-E. coli, which are spread by patient transfer between different types of health care facilities and the community.21,23 Thus, types of health care facilities located in a community may also influence the prevalence and trend over time of ESBL-E. coli infections in a particular community.
In the United States, studies on prevalence of infections caused by ESBL-E. coli are limited in number. Among them, the highest prevalence has been reported from skilled nursing facilities in California. 24 The majority of reports are based on observations made at single centers and only few studies compare health care settings within the same city.21,24–28 In this study, we compared temporal trends in infections caused by ESBL-E. coli in four distinct types of health care institutions in one city. Understanding health care facility factors associated with temporal changes in ESBL-E. coli infection prevalence could not only improve antibiotic stewardship efforts but also reduce or prevent the spread of these infections in community settings.
Materials and Methods
Study design and settings
This is a retrospective study based on annual clinical microbiology laboratory antimicrobial susceptibility reports from 2012 to 2018. We collected reports from four health care facilities located in San Francisco, California: (1) Zuckerberg San Francisco General Hospital, a public safety-net community health care facility that includes a 397-bed hospital and 15 San Francisco Health Network outpatient clinics distributed throughout the city (county hospital), (2) Laguna Honda Hospital, a 766-bed public skilled nursing and rehabilitation center, (3) University of California, San Francisco Medical Center, a 796-bed university-affiliated hospital, and (4) San Francisco Veterans Affairs (VA) Medical Center, a 124-bed hospital with 6 outpatient clinics in the greater Bay Area. Reports for the county and the VA hospitals combined isolates from inpatient and their affiliated outpatient services and did not separate the susceptibility reports by these services. Reports from the university hospital included isolates from inpatient services only. Reports from the skilled nursing facility were not available for the years 2017 and 2018.
Data collection
We abstracted E. coli antimicrobial susceptibility data and their clinical sources from the respective clinical microbiology reports. The isolate source data were separated as urine and nonurine isolates for the county hospital, the skilled nursing facility, and the VA hospital, but not for the university hospital for years 2012 and 2018. Nonurine isolates included blood and other sources, but reports did not further distinguish antimicrobial susceptibility by unique sources. Reports were generated based on the first isolate per patient per year.
Antimicrobial susceptibility testing
All facilities followed the most up-to-date CLSI guidelines for antimicrobial susceptibility testing (AST), including tests for ceftriaxone and trimethoprim-sulfamethoxazole for each year. The county hospital also processes laboratory isolates from the skilled nursing facility, and performs AST with Microscan and disk diffusion tests. The VA hospital performs AST with a VITEK system and the university hospital uses a Trek Sensititre system. In this study, we define ESBL-E. coli as E. coli strains reported by the clinical laboratories as ESBL producers or those resistant to ceftriaxone. Resistance to the antimicrobial agents is based on the reports provided by the respective clinical microbiology laboratories. All hospitals, except the university hospital, reported ESBL-E. coli as E. coli strains resistant to either ceftazidime or cefotaxime and inhibited by clavulanic acid. The university hospital did not specifically report frequency of ESBL-E. coli isolates. As of 2016, CLSI no longer requires confirmatory testing for ESBL production. 14
Statistical data analysis
The outcomes of interest were annual percent of ESBL-E. coli defined by ceftriaxone resistance, ESBL-E. coli defined by third-generation cephalosporin and inhibition to clavulanic acid, as well as resistance to trimethoprim-sulfamethoxazole. We included percent resistance to trimethoprim-sulfamethoxazole as a comparison for overall antimicrobial resistance trends. Data were tabulated for each antimicrobial agent per year and by site. Linear regression models were performed to determine change in percent antimicrobial resistance per year for each health care system when data were available for more than 2 consecutive years.
Results
From 2012 to 2018, the respective clinical microbiology laboratories reported antimicrobial susceptibility test results for 10,262 urine and 1349 nonurine E. coli isolates from the county hospital, 535 urine and 84 nonurine E. coli isolates from the skilled nursing facility (reports available up to 2016), 5993 total E. coli isolates from the university hospital, and 2326 urine and 473 nonurine E. coli isolates from the VA hospital, representing more than half of total hospital beds in San Francisco (Table 1). We analyzed trends in time in percent ESBL-E. coli and resistance to trimethoprim-sulfamethoxazole in each health care facility (Table 1 and Fig. 1). While there were less isolates from the skilled nursing facility, frequency of resistance to all antibiotics was highest at this institution.
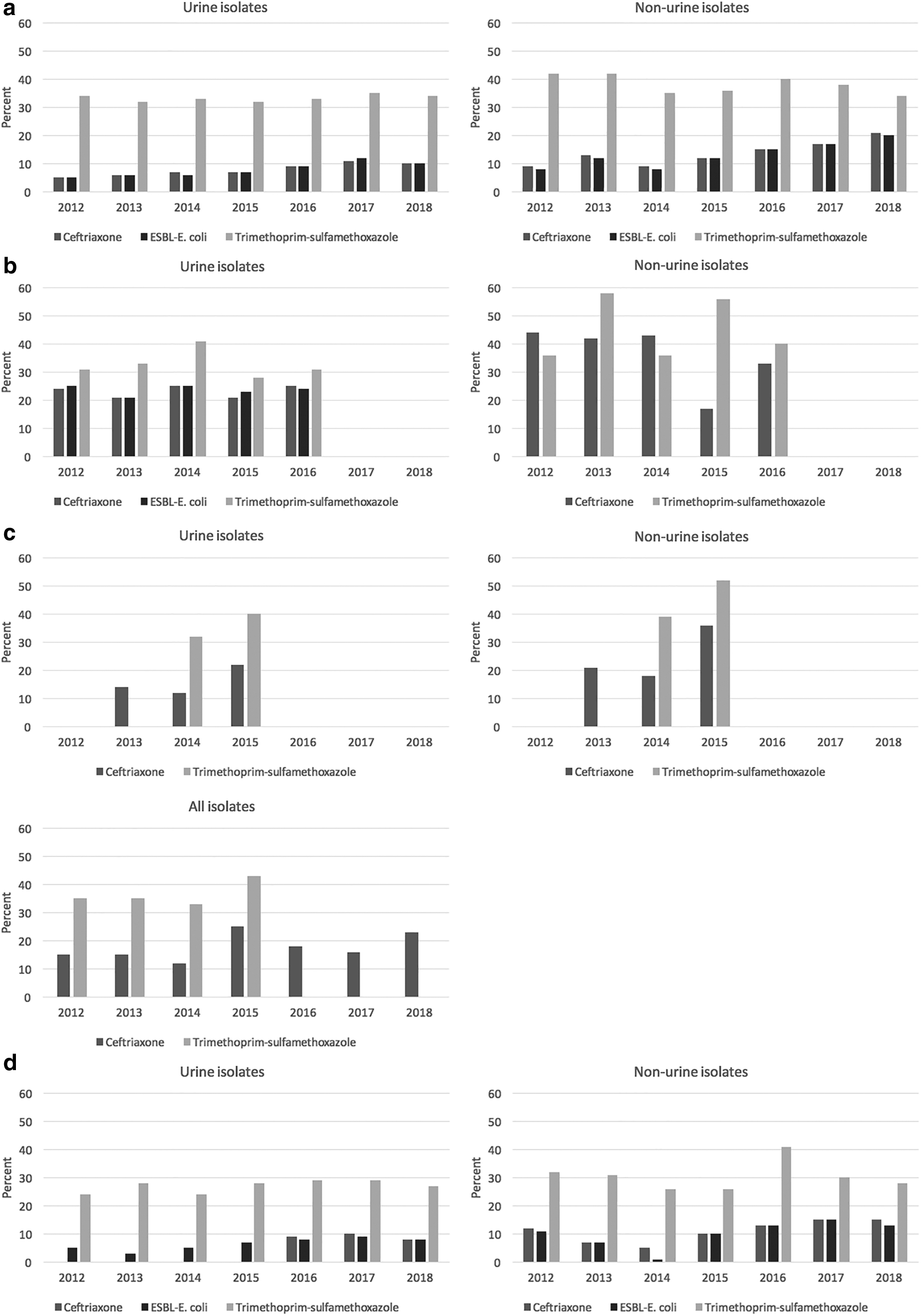
Percent of Escherichia coli isolates resistant to ceftriaxone and producing ESBL, by hospital, 2012–2016.
Extended-Spectrum Beta-Lactamase-Production and Resistance to Cephalosporins and Trimethoprim-Sulfamethoxazole of Urine, Nonurine, and Total Escherichia coli Isolates, by Hospital, 2012–2018
Data from annual microbiology laboratory antimicrobial susceptibility reports.
p < 0.01.
CI, confidence interval; ESBL, extended-spectrum beta-lactamase.
Frequency of ESBL-E. coli defined by ceftriaxone resistance only steadily increased from 5% in 2012 to 10% in 2018, increasing by 1.0% per year (95% confidence interval [CI]: 0.6–1.3, p < 0.01) in urine isolates from the county hospital. Ceftriaxone resistance in nonurine isolates at the county hospital increased from 9% to 21% from 2012 to 2018, increasing by 1.8% per year (95% CI: 0.7–2.9, p < 0.01) (Fig. 1). Frequency of ceftriaxone resistance in the skilled nursing facility fluctuated in urine and nonurine isolates from 2012 to 2016 (urine: between 21% and 25%, 0.2% per year, 95% CI: −2.1 to 2.6, p = 0.8 and nonurine: between 17% and 44%, −4.7% per year, 95% CI: −14.7 to 5.3, p = 0.2) (Fig. 1). Frequency of resistance to ceftriaxone fluctuated in urine and nonurine isolates in the university hospital from 2013 to 2015 (urine: between 12% and 22%, 4% per year, 95% CI: −40 to 48, p = 0.5 and nonurine: between 18% and 36%, 7.5% per year, 95% CI: −69.5 to 84.5, p = 0.4) and in all isolates from 2012 to 2018 (between 12% and 25%, 1.1% per year, 95% CI: −1.0 to 3.3, p = 0.2). In the VA hospital, frequency of resistance to ceftriaxone also fluctuated in urine (between 8% and 10% from 2016 to 2018, −0.5% per year, 95% CI: −11.5 to 10.5, p = 0.7) and nonurine isolates (between 5% and 15% from 2012 to 2018, 1.2% per year, 95% CI: −0.4 to 2.7, p = 0.1) (Fig. 1).
Frequency of ESBL-E. coli defined as strains resistant to third-generation cephalosporin and inhibited by clavulanic acid increased in the county hospital from 2012 to 2018 in urine isolates (5–10%, 1.1% per year, 95% CI: 0.5–1.6, p < 0.01) and in nonurine isolates (between 8% and 20%, 1.9% per year, 95% CI: 0.9–2.9, p < 0.01) (Fig. 1). In the skilled nursing facility, frequency of ESBL-E. coli in urine isolates fluctuated (between 21% and 25% from 2012 to 2016, 0% per year, 95% CI: −1.9 to 1.9, p = 1). In the VA hospital, from 2012 to 2018, frequency of ESBL-E. coli increased in urine (5–8%, 0.9% per year, 95% CI: 0.3–1.4, p < 0.01) and fluctuated in nonurine isolates (between 1% and 15%, 1.2% per year, 95% CI: −0.9 to 3.3, p = 0.2).
From 2012 to 2018, frequency of resistance to trimethoprim-sulfamethoxazole in the county hospital fluctuated in urine and nonurine isolates (urine: between 32% and 35%, 0.2% per year, 95% CI: −0.3 to 0.8, p = 0.3 and nonurine: between 34% and 42%, −1.0% per year, 95% CI: −2.3 to 0.4, p = 0.1). Frequency of trimethoprim-sulfamethoxazole resistance in the skilled nursing facility fluctuated in urine and nonurine isolates from 2012 to 2016 (urine: between 28% and 41%, −0.5% per year, 95% CI: −6.1 to 5.1, p = 0.2 and nonurine: between 36% and 58%, 0.6% per year, 95% CI: −12 to 13.2, p = 0.9). In the university hospital, frequency of resistance to trimethoprim-sulfamethoxazole was available from years 2014 to 2015, with an increase in urine, nonurine, and all isolates (urine: 32–40%, nonurine: 39–52%, and all isolates: 33–43%). In the VA hospital, frequency of resistance to trimethoprim-sulfamethoxazole fluctuated in urine and nonurine isolates from 2012 to 2018 (urine: between 24% and 29%, 0.6% per year, 95% CI: −0.4 to 1.5, p = 0.2 and nonurine: between 26% and 41%, 0.04% per year, 95% CI: −2.7 to 2.8, p = 1).
Discussion
Between 2012 and 2018, the prevalence and trend over time of ESBL-E. coli increased in urine isolates from the county hospital and the VA hospital, while it increased among nonurine isolates only in the county hospital. The frequency of ESBL-E. coli fluctuated among both urine and nonurine isolates at the other health care facilities (Fig. 1). On the other hand, trimethoprim-sulfamethoxazole resistance among urine and nonurine isolates fluctuated between 24% and 58% at all institutions. We found that E. coli isolates from the skilled nursing facility had the highest frequency of ESBL-E. coli (21–25%), similar to levels reported from high-prevalence countries such as Jordan, Korea, Italy, and the United Kingdom, and other skilled nursing facilities in the United States.2,3,23,24,29
High prevalence of ESBL-producing organisms in long-term care facility residents has been well documented worldwide for the last 30 years.3,23,30–32 Indeed, the first outbreak in the United States due to bacteria harboring plasmid-encoded ESBL genes occurred in a long-term care facility in Massachusetts in 1990. 33 Colonization frequency with ESBL-producing Enterobacteriaceae in residents of U.S. long-term care facilities has ranged from 3.4% to 46%.24,34–37 Residents of long-term care facilities have multiple comorbidities and therefore are at increased risk of acquiring multidrug-resistant pathogens.30,38 About half of all medications prescribed in long-term care facilities are antibiotics, most commonly used to treat UTI. 38 While antibiotic stewardship programs have been developed in long-term care facilities, studies have suggested that up to 70% of antibiotic prescriptions are not appropriate. 38 Exposure to the microflora of other residents and health care providers may also contribute to spread of antimicrobial-resistant organisms within a long-term care facility. 1 In addition, instrumentation such as urinary catheterization or percutaneous endoscopic gastrostomy, as well as decubitus ulcer management, poor nutrition, and immunocompromised state of the residents, increase the risk of recurrent antimicrobial-resistant pathogen colonization and infection. 30 Long-term care facilities have been shown to serve as reservoirs for antimicrobial-resistant pathogens, including ESBL-E. coli that spread to acute-care institutions.6,36,38
Interestingly, however, we found in our study that despite the high prevalence of ESBL-E. coli infections in the skilled nursing facility, it remained relatively stable over the 5 years. This suggests effectiveness of the facility's antibiotic stewardship program, or limited ESBL-E. coli strain types circulating in the facility. ESBL-E. coli prevalence fluctuated in nonurine isolates, but increased in urine isolates from the VA hospital and their affiliated clinics. While the county hospital provides health care largely to safety-net and low-income community patients, the VA hospital serves a population with risks that differ from the general population. The E. coli isolates tested at the county hospital and the VA hospital include those collected from patients examined at outpatient clinics located in different neighborhoods in San Francisco and in the greater Bay Area. The county hospital also receives patients transferred from the skilled nursing facility, but the progressive increase in prevalence of ESBL-E. coli in the urine isolates in this hospital cannot be explained solely by these transferred patients since prevalence was stable in the skilled nursing facility. The stable frequency of resistance to trimethoprim-sulfamethoxazole of the urine isolates from the county and the VA hospitals over the 7 years suggests that the increase in frequency of ESBL-E. coli UTIs is a true increase not affected by sampling differences.
In this study, we found that trends over time in ESBL-E. coli defined by third-generation cephalosporin resistance only in E. coli isolates were similar to those of ESBL-E. coli defined with inhibition to clavulanic acid, except in nonurine E. coli isolates from the county health care facility and urine E. coli isolates from the skilled nursing facility. Those divergent trends may be explained by the presence of strains that express plasmid-encoded AmpC cephamycinase (CMY), or carbapenemase, which will exhibit similar spectrum of resistance mediated by ESBL. 39 Such strains are more likely to be recovered from nonurine isolates or from patients residing in skilled nursing facilities, as observed in this study.
There are several limitations to our study. First, we based our analyses on compiled annual antimicrobial susceptibility reports. Nevertheless, we were able to detect differences between health care sites by using these reports representative of all E. coli isolates. Second, these reports did not differentiate clinical settings (inpatient vs. outpatient) in which the patients were examined. Hence, we were not able to assess trend according to community-acquired versus health care-associated ESBL-E. coli infections for county and VA hospital patients. The largest proportion of the isolates was urine isolates from the county hospital. If most of them represent isolates from cases of community-acquired urinary tract infections (CA-UTI), the observed increase in ESBL-E. coli is a concern. Interestingly, such an increase was not observed for E. coli strains resistant to trimethoprim-sulfamethoxazole, a drug commonly used to treat CA-UTI. We did not have access to reports from the skilled nursing facility beyond 2016 and thus were not able to evaluate trends over a longer period of time. While ESBL-E. coli was first identified in 1988 in the United States, 40 the microbiology laboratories at these sites started to report ESBL-E. coli only in 2011. Beta-lactamases are complex, and the definition used in our study was not comprehensive or uniform, limited by the techniques employed by each health care system laboratory. The clinical microbiology laboratories reported ESBL production based on either commercial (e.g.: VITEK) or CLSI reference methods, which may miss certain types of ESBLs. However, we compared temporal trends within, not across, each health care system, which should not affect our conclusions. Finally, there may be duplication of bacterial isolate information, especially since some of the patients from the skilled nursing facility may be acutely hospitalized at the county hospital.
Prevalence and temporal trend of ESBL-E. coli infections differ by health care institutions, suggesting differences in patient exposure, demographic factors, underlying patient clinical conditions, as well as institutional antibiotic stewardship practices, and other unrecognized factors. These observations demonstrate that even within one city, ESBL-E. coli infection prevalence and trend can vary greatly, and that the reported geographic differences may be affected by health care institutional patient population types. Most antibiotic stewardship programs in hospitals rely on facility-specific data to make recommendations regarding empirical antibiotic use. 41 We propose that, in addition to understanding antimicrobial resistance patterns within a facility, the creation of a collaborative tool mapping interfacility and community patterns of resistance may contribute to more effective stewardship programs.
Footnotes
Authors' Contributions
E.R. and H.F.C. devised the study. E.R. analyzed and interpreted the data on prevalence of antimicrobial resistance by health care institutions. E.R. drafted the article. All authors read and approved the final article.
Acknowledgments
The authors thank Maria Glymour and Rita Hamad for their valuable feedback on the article and Shivani Mahuvakar for her help with data collection. We also thank the UCSF Primary Care Research Fellowship for their valuable input for early drafts of the article.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
E.R. is supported by T32HP19025.