
Abstract
This updated systematic review and meta-analysis followed two objectives: (1) to determine Helicobacter pylori antibiotic resistance in Iran during 2010–2020 and (2) to assess the trend of resistance from 1997 to 2020. A systematic search in multiple databases, including ISI Web of Knowledge, PubMed, Scopus, Google Scholar, and the Scientific Information Database (SID), was performed using MeSH-extracted keywords. Meta-analysis was done on extracted data from a total of 27 included citations published between 2010 and January 20, 2020. The overall mean prevalence of H. pylori resistance was 64.9% for metronidazole, 25.3% for clarithromycin, 20.7% for amoxicillin, 16.1% for tetracycline, 21.9% for levofloxacin, 22.8% for rifampicin, 27.2% for furazolidone, 32.3% for ciprofloxacin, and 38.7% for erythromycin. In addition, the prevalence of multidrug-resistant strains of H. pylori was 26.5% in Iran. The pooled prevalence of point mutations A2143G, A2142G, and A2142C associated with clarithromycin resistance were 46.6%, 37.2%, and 5.5%, respectively; mutations in frxA and rdxA genes associated with metronidazole resistance were 46.4% and 19.7%, respectively; gyrA and gyrB genes mutations among fluoroquinolone-resistant strains were 55.3% and 48.2%, respectively; and resistance associated with integrons was 47%. According to the present findings, resistance of H. pylori to antibiotics used for eradication therapy has reached an alarming level in Iran. Furthermore, the trend of H. pylori resistance has increased between 1997 and 2020. Hence, continuous surveillance on resistance patterns, logical prescription and appropriate consumption of antibiotics, and selecting effective therapeutic regimens in accordance with local resistance patterns are required to prevent further spread of resistance and ensuing treatment failures.
Introduction
Gastritis, peptic and duodenal ulcers, adenocarcinoma, and mucosa-associated lymphoid tissue lymphoma are important diseases associated with a spiral-shaped gram-negative bacterium called Helicobacter pylori, which is colonized in stomach of ∼4.4 billion individuals worldwide.1–3 In Iran, H. pylori is highly prevalent (ranged from 40% to 90%). 4 Due to global differences in the prevalence of H. pylori infection, there is no single therapy guideline applicable to all populations. 5 Although complete elimination of H. pylori is not possible with the current regimens, some combination treatment regimens are more effective and recommended against H. pylori, including first-line therapies (1) clarithromycin triple therapy for 14 days in regions with low clarithromycin resistance, including a proton pump inhibitor (PPI) plus 2 antibiotics such as clarithromycin and amoxicillin or either metronidazole or tinidazole, (2) nonbismuth quadruple therapy, including a PPI plus 3 antibiotics (clarithromycin, amoxicillin, and metronidazole or tinidazole) in either sequential therapy or concomitant therapy, and (3) bismuth quadruple therapy for 10–14 days when resistance to clarithromycin is high, including a PPI, bismuth salt, tetracycline, and metronidazole.5,6 Second-line therapies, including bismuth quadruple therapy or levofloxacin triple therapy (PPI plus levofloxacin and amoxicillin for 14 days), have been used after the failure of the first-line therapy, and third-line therapy includes a bismuth-based levofloxacin quadruple therapy or rifabutin-containing triple therapy (PPI plus rifabutin and amoxicillin).5,6 Antibiotic selection for third-line therapy of H. pylori infections depends on the local resistance rates and should be based on antimicrobial susceptibility testing. 5 However, factors such as microbial pathogenicity (e.g., antibiotic resistance of the microorganism), host immune response, and improper treatment (e.g., administration of antibiotics for the infections other than H. pylori, inaccurate use of antibiotics or patient noncompliance) could negatively impact the efficacy of these regimens and eventually lead to treatment failure. 7 Recently, the World Health Organization (WHO) has announced that there is a wide emergence of H. pylori strains resistant to clarithromycin, which necessitates development of novel antibiotics. As the prevalence of antibiotic resistance is changing over time, continuous monitoring of H. pylori resistance is of great importance. 8
Previously, we evaluated H. pylori antibiotic resistance in Iran within the time span of 1997–2010, but additional data are now available in the recent decade. 9 This updated systematic review and meta-analysis sought two objectives: the primary aim was to determine the antibiotic resistance prevalence during 2010–2020, and the secondary aim was to evaluate the trend of resistance from 1997 to 2020 in Iran.
Methods
Data sources and searches
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) protocols were used to perform an updated systematic review and meta-analysis on the H. pylori antibiotic resistance in Iran. 10 Between 2010 and January 20, 2020, a two-step full electronic search was done by the authors in national and international databases as well as in the references lists of included studies to search for any published literatures in Persian and English languages. For this purpose, necessary keywords, such as “prevalence” OR “frequency” OR “epidemiology” OR “incidence” AND “Helicobacter pylori” OR “H. pylori” AND “drug resistance” OR “antibiotic resistance” OR “antimicrobial resistance” AND “Iran”, were extracted from MeSH along with connectors (AND/OR) used in ISI Web of Knowledge, PubMed, Scopus, Google Scholar, and the Scientific Information Database (SID) search engines. Missing relevant publications in the initial search strategy were also assessed manually during final search in the reference lists of included studies.
Data selection criteria and quality assessment
The title of cross-sectional studies published in English and Persian followed by abstracts and full review of articles were initially assessed to determine suitability in terms of predefined inclusion and exclusion criteria. Our inclusion criteria were articles reporting the prevalence of H. pylori antibiotic resistance, published articles between 2010 and January 20, 2020, articles reporting the prevalence of H. pylori antibiotic resistance in clinical specimens, and data limited to Iran. The exclusion criteria were nonoriginal articles, abstracts from conferences, articles published as duplicate in both English and Persian languages, articles assessing H. pylori drug resistance on the same samples, articles with insufficient information, articles assessing antibiotic susceptibility patterns via molecular tests, as these methods are not approved for defining H. pylori resistance by the United States Food and Drug Administration (FDA), studies reporting the prevalence, treatment, and virulence genes of H. pylori, and articles without study date. Article quality assessment was performed using the Joanna Briggs Institute (JBI) critical appraisal checklist and articles were accordingly classified into three groups; high quality (>5 scores), low quality (<4 scores), and medium quality (4–5 scores). 11
Data extraction
As shown in Table 1, the following data were extracted from each eligible study; first author's surname, year of publication, region of study, study date, age of patients, number of tested isolates, methods used for assessing bacterial antibiotic susceptibility, the prevalence of H. pylori resistance to different antibiotics, and the prevalence of antibiotic resistance genes.
Extracted Information from Eligible Studies Included in the Meta-Analysis
MTZ, metronidazole; CLR, clarithromycin; AMX, amoxicillin; TET, tetracycline; LVX, levofloxacin; RIF, rifampicin; FRZ, furazolidone; CIP, ciprofloxacin; ERY, erythromycin; MDR, multiple drug-resistant; AST, antimicrobial susceptibility testing; ND, not determined.
Data analysis
We analyzed the extracted data on the H. pylori antibiotic resistance by Comprehensive Meta-Analysis (CMA) software (Biostat, Englewood, NJ) based on the presence of heterogeneity. The results were presented as percentage and 95% confidence intervals (95% CIs). Heterogeneity among included studies was checked by I2 statistic and the chi-square test with the Cochrane Q statistic. Heterogeneity was considered high when I2 was ≥25%; random-effects model and low when I2 was <25%; fixed-effects model. Funnel plots were used to assess the existence of publication bias.
Results
A total of 27 out of 1,478 initial articles searched in electronic databases from 2010 to 2020 met the eligibility criteria and included in the meta-analysis (Fig. 1). These articles, with a quality score between 4 and 8 included 12 studies from Tehran, 3 studies from Shiraz, 2 studies from Ahvaz, 2 studies from Rasht, 2 studies from Sari, and 1 study from cities of Isfahan, Tabriz, Yazd, Kashan, Chaharmahal va Bakhtiari, and Lahijan. Disk diffusion, E-test, agar, and broth dilution were the most common methods applied to determine H. pylori antibiotic resistance in Iran.

Flowchart of literature search results.
In the current study, total prevalence of H. pylori resistance to metronidazole antibiotic in Iran was 64.9% (95% CI: 59.6–69.8), which is calculated by random-effects model due to existence of significant heterogeneity (I 2 = 82%; Q = 116.7; p = 0.00). As shown in Table 2, the highest and lowest prevalence of metronidazole-resistant H. pylori strains in different cities of Iran was found in Yazd (77.8%) and Lahijan (43.7%), respectively. Furthermore, Fig. 2 demonstrates a gentle rise in metronidazole-resistant strains during 2010–2020 (64.9%) in comparison with 1997–2010 (61.6%) in Iran. Similarly, clarithromycin-resistant strains showed an increasing pattern in Iran from 1997 to 2020 (Fig. 2). Between 2010 and 2020, the prevalence of clarithromycin-resistant H. pylori strains in Iran was 25.3% (95% CI: 19–32.9) (Fig. 3) versus 22.4% from 1997 to 2010. Meta-analysis of data addressing clarithromycin resistance showed a significant heterogeneity among the included studies (I 2 = 93.1%; Q = 347.8; p = 0.00). Based on the subgroup analyses, the prevalence of clarithromycin-resistant strains was highest (63.6%) in Chaharmahal va Bakhtiari and lowest (5.5%) in Rasht, Iran. The amoxicillin resistance rate from 2010 to 2020 was 20.7% (95% CI: 12.8–31.8; I2 = 95.3%; Q = 322.7; p = 0.00) compared to 16% during 1997– 2010 in Iran. The highest resistance rate was found in Chaharmahal va Bakhtiari (62.9%) and the lowest was seen in Lahijan (0%). In random-effect meta-analysis of data, the prevalence of tetracycline-resistant H. pylori strains was 16.1% (95% CI: 11.4–22.4; I2 = 84.7%; Q = 91.5; p = 0.00) from 2010 to 2020 in Iran, which was higher than our previous report from 1997 to 2010 (12.2%). The highest tetracycline-resistance rate was observed in Rasht (23.8%) and the lowest rate was in Lahijan (0%). Levofloxacin-resistance rate was 21.9% (95% CI: 14–32.5; I2 = 87.5%; Q = 56.2; p = 0.00), which is higher than 1997–2010 period (5.3%). Lahijan (37.5%) and Sari (3.3%) showed the highest and the lowest resistance rate among Iranian cities, respectively. Frequency of H. pylori resistance to other antibiotics were as follows: rifampicin 22.8% (95% CI: 16.9–30; I2 = 64.1%; Q = 11.1; p = 0.02), furazolidone 27.2% (95% CI: 16.5–41.4; I2 = 85.7%; Q = 35; p = 0.00), ciprofloxacin 32.3% (95% CI: 23.9–41.9; I2 = 92.6%; Q = 150.1; p = 0.00), and erythromycin 38.7% (95% CI: 19.1–62.8; I2 = 96.1%; Q = 77.9; p = 0.00). As shown in Fig. 2, furazolidone resistance (21.6–27.2%) and ciprofloxacin resistance (21–32.3%) followed an increasing annual trend from 1997 through 2020. In addition, the prevalence of multidrug-resistant (MDR) strains of H. pylori, which is defined as strains with simultaneous resistant to ≥3 different classes of antibiotics, was 26.5% (95% CI: 14.3–43.9; I2 = 95.7%; Q = 164.1; p = 0.00) in Iran.
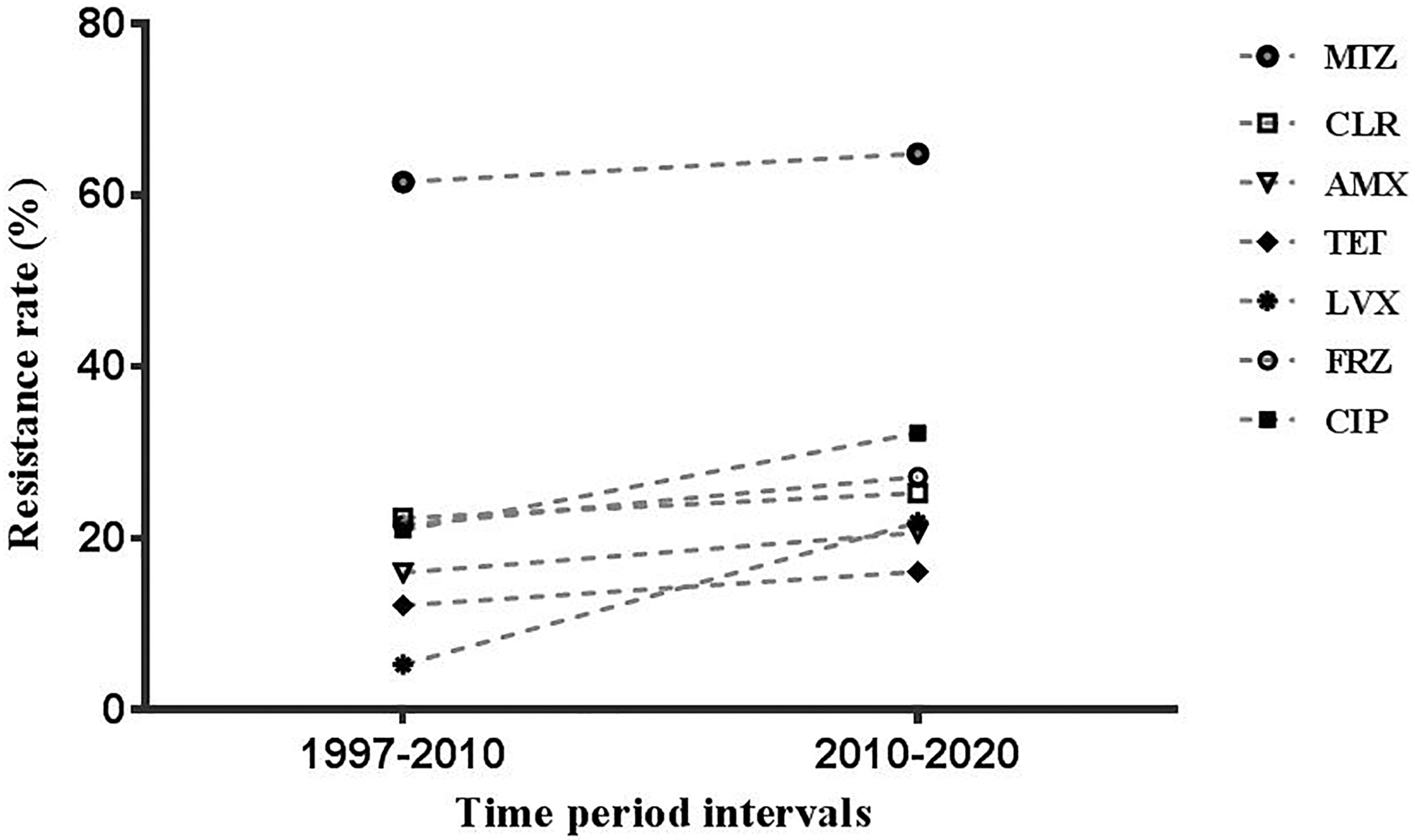
Antimicrobial resistance trends of Helicobacter pylori strains to different medications in Iran from 1997 to 2020.
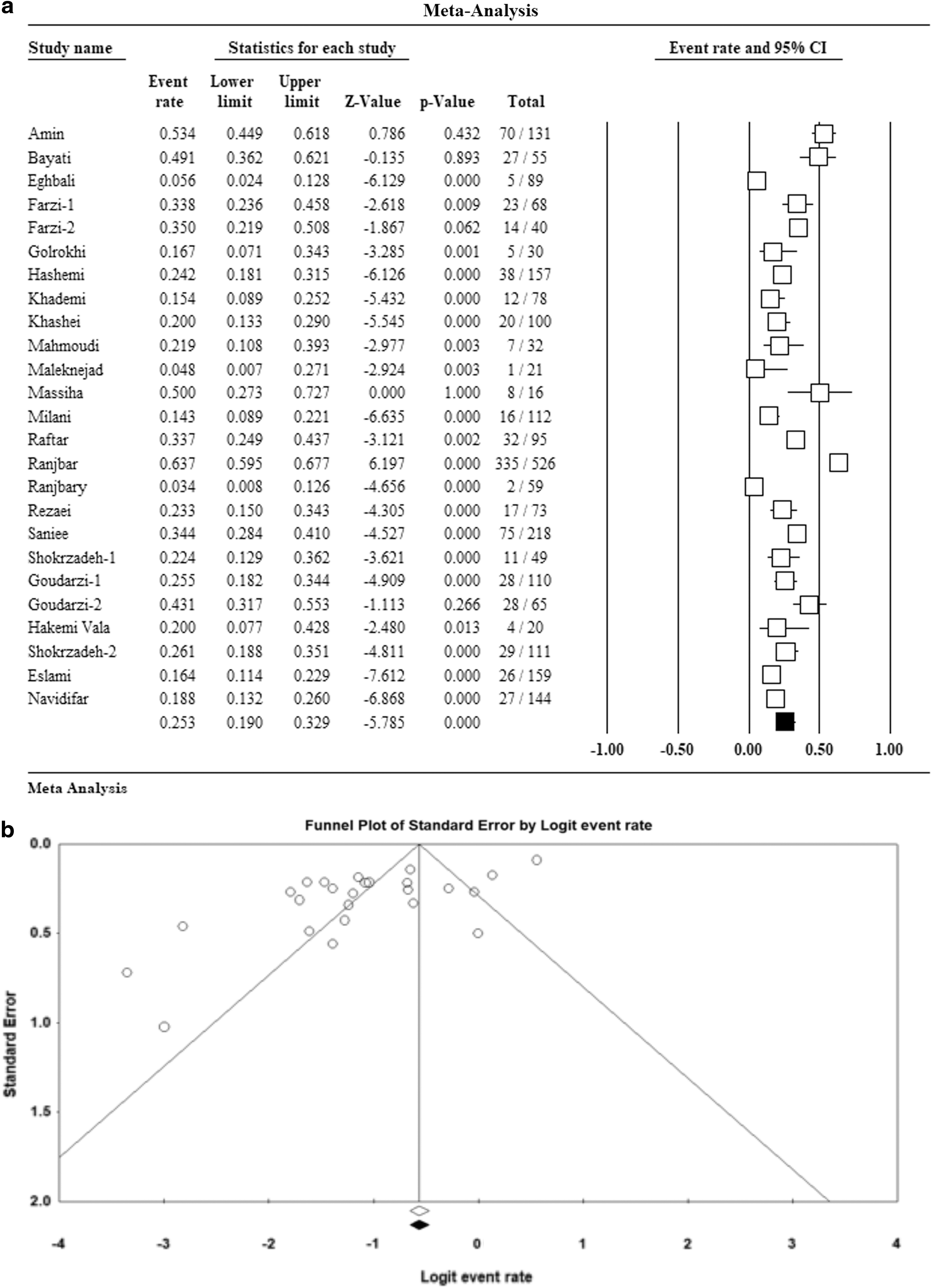
Forest plot
Helicobacter pylori Antibiotic Resistance Profiles in Different Cities of Iran
MTZ, metronidazole; CLR, clarithromycin; AMX, amoxicillin; TET, tetracycline; LVX, levofloxacin; RIF, rifampicin; FRZ, furazolidone; CIP, ciprofloxacin; ERY, erythromycin; MDR, multiple drug-resistant; ND, not determined.
Included studies also evaluated antibiotic resistance-associated genes such as 23S rRNA, frxA, rdxA, gyrA, gyrB, and integrons (Table 1). Point mutations in the peptidyl transferase region of domain V in 23S rRNA gene confer H. pylori resistance to clarithromycin. In Iran, A2143G (46.6%; 95% CI: 27.9–66.3; I2 = 81.7%; Q = 49.3; p = 0.00), A2142G (37.2%; 95% CI: 16.6–63.7; I2 = 86.4%; Q = 44.2; p = 0.00), and A2142C (5.5%; 95% CI: 2.5–11.4; I2 = 0.0%; Q = 2.9; p = 0.4) point mutations were more common among H. pylori strains. Similarly, mutations in frxA and rdxA genes result in metronidazole resistance in H. pylori. In the current study, the prevalence of frxA and rdxA mutations associated with metronidazole resistance were 46.4% (95% CI: 37.9–55.2; I2 = 0.0%; Q = 0.1; p = 0.71) and 19.7% (95% CI: 3.6–61.4; I2 = 94.9%; Q = 79.4; p = 0.00), respectively; frequency of gyrA and gyrB genes among fluoroquinolone-resistant strains were 55.3% and 48.2%, respectively; and distribution of integrons in H. pylori isolates was 47% (95% CI: 26.2–68.9; I2 = 87.9%; Q = 8.3; p = 0.00) in Iran.
Discussion
The incidence of resistance to antibiotics is regionally variable depending on the administered dose and duration of treatment, socioeconomic conditions, and excessive use of antibiotics in other infections. Therefore, continuous monitoring of H. pylori resistance trend through systematic reviews and meta-analyses is especially important and can guide the choice of treatment regimens to achieve a successful eradication of H. pylori.18,39
Clarithromycin is a bacterial protein synthesis inhibitor and clarithromycin-based triple therapy was considered as the standard treatment for H. pylori infections until 2004. However, clarithromycin resistance was the main culprit for triple therapy failure. 40 It has been shown that H. pylori resistance to clarithromycin along with metronidazole and levofloxacin could decrease the efficacy of treatment. 6 Clarithromycin-based therapy is not recommended when resistance rate is more than 15%. 6 From 2011 to 2017, resistance to clarithromycin in various countries were as follows: China 73%, Bulgaria 28%, Turkey 21%, Italy 72%, South Korea 37%, India 58%, United States 16%, and Portugal 50%. 40 Our previous study showed that 22.4% of H. pylori strains were resistant to clarithromycin during 1997–2010, and the prevalence has reached 25.3% from 2010 to 2020. H. pylori infection is not commonly treated with clarithromycin in Iran; hence, rising trend of H. pylori resistance to clarithromycin could be attributed to the extensive use of this antibiotic for respiratory infections especially in children, or cross-reactivity with other macrolides.12,18 The resistance rate to another macrolide (i.e., erythromycin) was much higher in Iran (38.7%). The use of clarithromycin triple therapy or other clarithromycin-containing regimens are not recommended in individuals who had a previous exposure to macrolides because it will be lead to treatment failure. 5 According to these findings, clarithromycin-based therapy is not recommended for treatment of H. pylori in Iran. The rRNA point mutations were a common predisposing factor for the emergence of clarithromycin-resistance H. pylori strains. A2143G, A2142G, and A2142C were the most significant point mutations detected from H. pylori strains isolated in Iran.
Depending on the geographic location, previous treatment history and antimicrobial susceptibility testing, bismuth quadruple therapy, and levofloxacin triple therapy are recommended when clarithromycin-based therapy fails.5,6 Metronidazole, a nitroimidazole, is a component of bismuth quadruple and clarithromycin triple therapies against H. pylori infections, and acts via the formation of nitro-anion radicals and bacterial DNA damage. 7 However, the prevalence of metronidazole-resistant H. pylori strains is much more common than other drugs. 7 Based on the previous studies, H. pylori strains resistance rate to metronidazole varies in different regions of the world as follows; Asia 46.5%, South America 52.8%, North America 30.5%, Europe 31.1%, and Africa 75%. 7 In the present study, H. pylori resistance to metronidazole was 64.9% in Iran. Moreover, the trend of metronidazole resistance in H. pylori strains in Iran showed a rather mild increase from 61.6% during 1997–2010 to 64.9% during 2010–2020. Frequent administration of metronidazole for parasitic, gynecologic, and oral infections could have caused this high resistance rate. 12 Moreover, several resistance mechanisms to metronidazole were identified in H. pylori, including the existence of efflux pumps or DNA repair enzymes. 7 Our results showed that metronidazole resistance of H. pylori strains in Iran was related to mutations in NADPH nitroreductase (rdxA) and NADPH-flavin-oxidoreductase (frxA) genes.
Amoxicillin, a cell wall synthesis inhibitor, is a substantial component of clarithromycin, levofloxacin, and rifabutin (PPI, amoxicillin and rifabutin)-based triple therapies especially in metronidazole-resistant cases.6,7 According to the previous literature, resistance to anti-H. pylori medications such as amoxicillin, tetracycline, and rifabutin is rare. 6 The prevalence of amoxicillin resistance in Asia, South America, North America, Europe, and Africa were 23.6%, 6.5%, 2, 0.3%, and 40.8%, respectively. 7 Findings of the present study indicated a gradual rise in H. pylori resistance to amoxicillin in Iran from 16% during 1997–2010 to 20.7% during 2010–2020.
Tetracycline is another component of bismuth quadruple therapy and a protein synthesis inhibitor. H. pylori resistance to tetracycline in Asia is 7.3%, 0% in South America and North America, 1.1% in Europe, and 50% in Africa. 7 In Iran, tetracycline resistance rate showed an increasing trend from 1997–2010 (12.2%) to 2010–2020 (16.1%).
In this study, 22.8% of H. pylori strains were resistant to rifampicin. Overuse or misuse of amoxicillin and tetracycline antibiotics is responsible for the development of resistance in H. pylori strains. 33 Other factors such as production of β-lactamase enzymes, point mutations in pbp1 gene encoding penicillin-binding protein in amoxicillin-resistant strains, and mutations in 16S rRNA gene in tetracycline-resistant strains were also identified 33 ; however, these factors were not assessed in the included articles in this study.
Levofloxacin-based triple therapy is the treatment of choice when first-line therapies, that is, bismuth quadruple and clarithromycin triple therapies against H. pylori are not applicable. 6 While the worldwide resistance rate to levofloxacin is relatively low, prevalence of mean overall resistance to levofloxacin was 21.9% in Iran during 2010–2020, which is higher than those reported from Austria (11%), Bulgaria (10%), Croatia (2%), France (15%), Germany (18%), Italy (5%), United Kingdom (5%), and Australia (5%) and also lower than Belgium (29%), Turkey (30%), Bangladesh (66%), Indonesia (31%), and China (33%).2,7 In addition, overall levofloxacin resistance increased from 5.3% before 2010 to 21.9% during 2010 to 2020. Resistance to another fluoroquinolone, ciprofloxacin, was 32.3% in Iran. This high resistance can be attributed to the extensive use of quinolones in some coinfections such as urinary tract infections or respiratory diseases as well as mutational changes in gyrA and gyrB genes.30,41
Another nitrofuran such as metronidazole which is used for H. pylori eradication, particularly in combination with bismuth, is furazolidone. 42 Low resistance rate, cost-effectiveness, and wide availability have led to the use of furazolidone for treatment of different infections such as diarrheal diseases in many countries such as Iran. However, the current study showed that the rate of furazolidone-resistant H. pylori strains increased in Iran from 21.6% before 2010 to 27.2% during 2010 to 2020. 42 Frequencies of furazolidone resistance in Asia and South America were 23% and 0%, respectively. 7 Resistance to furazolidone has not been determined in some regions such as the United States, Europe, and Africa, since the drug is not available in many western countries after 2002 when the FDA prohibited its use in agriculture and food-producing animals. 42
A concerning finding in the current study, which is also a global health concern, was the prevalence of MDR H. pylori strains in Iran. Nevertheless, only few studies have reported the rate of emerging MDR H. pylori strains in Iran and in the world. 36 The prevalence of MDR H. pylori strains in Iran was 26.5% during 2010–2020, which is higher than that reported from Cameroon, but lower than those of Taiwan and Mexico.36,43 It was proposed that long-term and uncontrolled use of antibiotics and self-treatment of infections by patients in countries such as Iran with higher rates of H. pylori infection could have led to the emergence MDR H. pylori strains. In addition, different resistance mechanisms, including mutational changes in 23S rRNA, rdxA, frxA, gyrA, and gyrB genes, and overexpression of efflux pumps are other factors involved in the emergence of MDR H. pylori. 13
Conclusion
This systematic review and meta-analysis was an updated study to help increasing awareness on antibiotic resistance trends in H. pylori strains during 2010–2020 compared to 1997–2010, as the prevalence of antimicrobial resistance varies during the years. According to the present findings, resistance of H. pylori to antibiotics used for eradication therapy and MDR strains are evolving rapidly in Iran. There is also an overall increasing trend in antibiotic-resistant H. pylori strains during the years of 1997–2020. We can conclude that none of the recommended traditional therapies for H. pylori eradication is an effective treatment regimen in Iran. Therefore, to boost the efficacy of treatment and to prevent further spread of resistance, the following approaches could be recommended: (1) logical prescription of antibiotics to treat diseases other than H. pylori by physicians, (2) selection of effective therapeutic regimens against H. pylori in accordance with local resistance patterns, (3) providing educational programs for appropriate use of antibiotics by patients, (4) continuous monitoring of antibiotic sensitivity of this fastidious organism through reliable methods, and (5) development of novel molecular techniques to determine the mechanism of resistance and to facilitate more accurate, efficient, and rapid assessment of drug resistance rate.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.