
Abstract
Objectives:
Outbreak and endemic isolates of Acinetobacter baumannii are known to be polyclonal. In an ongoing study, we hypothesized that the patient gut was the source of the polyclonality where genetic exchanges take place. To test the hypothesis, we collected 270 serial rectal isolates from 32 adult intensive care unit patients over 16 months and investigated their drug resistance profiles.
Methods:
Antimicrobial susceptibility was determined according to recommended methods. The blaIMP, blaVIM, blaSIM, blaOXA-23, blaOXA-24/40, blaOXA-51, blaOXA-48, blaKPC, blaGES, blaNDM and blaOXA-58 were sought by PCR. A subset of 42 isolates were studied for plasmid-mediated resistance.
Results:
Most of the 270 isolates were multidrug resistant (MDR; with resistances to meropenem of 85.18% and imipenem of 87.04%), but susceptible to colistin and trimethoprim/sulfamethoxazole. There was no correlation between the pattern of resistance and antibiotics administered to treat infections. There was no consistent pattern of resistance or content of carbapenemase genes in serial rectal isolates suggesting polyclonality of the isolates. Genes mediating production of OXA-23, OXA-24/40, IMP, and GES enzymes were carried on plasmids and they mediated resistance to all carbapenems in conjugation studies.
Conclusion:
A. baumannii colonizing the rectum were polyclonal, MDR, and carbapenem resistance genes were found on plasmids and some plasmids were transferable.
Introduction
Multidrug-resistant (MDR) Acinetobacter baumannii is an opportunistic pathogen that can lead to serious outcomes in vulnerable patients. Outbreaks of A. baumannii infection in intensive care units (ICUs) are frequent in many parts of the world, including in Kuwait. 1 Implementation of infection control measures such as ICU closure and disinfection had only limited success in containing the outbreaks. Investigation of outbreaks has shown that the isolates are polyclonal. 2 Even the isolates causing endemic infections are polyclonal. 3 In an ongoing study, we hypothesized that the patient gut was the source of the polyclonality, where genetic exchanges can take place among bacterial isolates. To test the hypothesis, we collected serial isolates colonizing the rectum of adult ICU patients (data under analysis). In the current study, these isolates were characterized for their susceptibility to a wide spectrum of antimicrobial agents, specific resistance genes, and their locations on plasmids as well as their transferability. The results are reported in this communication.
Materials and Methods
Study design
This prospective cohort study was performed in the adult ICU of Mubarak Al Kabeer Hospital, which is a teaching hospital in Kuwait with 850 beds in non-ICU units and 30 beds in the adult ICU. The period of study was from March 2015 to June 2016. The catchment area of this hospital has a population of ∼700,000 people. Rectal swabs were collected from all consecutive, newly admitted patients. Swabs were taken on the day of admission, on the third day of admission, and then twice weekly until the patient was either discharged or dead. Only patients with five or more positive cultures were included in the study.
Patient chart review
The hospital medical records of patients from whom samples were collected were reviewed. Relevant information collected included age, gender, nationality, diagnosis and comorbidity, antibiotic therapy, and live discharge or death. A. baumannii infection was defined as the isolation of the organism from a specific site in a patient presenting with associated symptoms, such as fever, leukocytosis, increased levels of inflammatory markers, hypotension, etc., and who responded to therapy characterized by resolution of fever, decreased levels of inflammatory markers, and improvement in general wellbeing.
Isolation and identification of A. baumannii isolates
Rectal swabs were inoculated in an enrichment broth containing acetate and incubated aerobically, with shaking, at 37°C for 48 hr. 4 It was then subcultured onto Acinetobacter CHROMagar (DRG International, Springfield, NJ) and incubated at 37°C for 48 hr. Different morphotypes of typical large red colonies were selected. The colonies were further identified by API NE20 (bioMérieux, Marcy, l'Etoile, France) and confirmed by a duplex PCR assay for gyrB gene. The primers used were: sp4F (5′-CACGCCGTAAGAGTGCATTA), sp4R (5′-AACGGAGCTTGTCAGGGTTA), and sp2F (5′-GTTCCTGATCCGAAATTCTCG) with cycling conditions of 94°C for 2 min, then 25 cycles of 94°C for 1 min, 60°C for 30 sec, and 72°C for 1 min, with a final extension at 72°C for 10 min. The amplified products were visualized by ultraviolet (UV) light illumination after electrophoresis on a 2% agarose gel (Invitrogen, Camarillo, CA) with 0.5 μg/mL ethidium bromide at a voltage of 130 amps for 30 min. The yield of two bands of 294-bp (amplified by sp4F to sp4R) and 490-bp (amplified by sp2F to sp4R) identified A. baumannii, whereas a single band of 294-bp identified Acinetobacter genomic species 13TU. 5
Antibiotic susceptibility testing
For susceptibility testing, we selected 16 antibiotics that are commonly used for the treatment of A. baumannii infection. Susceptibility test was performed by E-test method (bioMerieux) and interpreted according to Clinical and Laboratory Standards Institute (CLSI) susceptibility criteria. 6 Susceptibility to tigecycline was determined according to the criteria of Talaga et al. 7 Susceptibility to colistin was performed by agar dilution method and interpreted by CLSI criteria. 6
Detection of carbapenem-resistant genes
A multiplex PCR was performed for the detection of all the genes. 8 DNA was extracted by boiling method from a 24 hr culture on blood agar. The primers used for amplification of genes, blaIMP, blaVIM, blaSIM, blaOXA-23, blaOXA-24/40, blaOXA-51 and blaOXA-58 were those of Mostachio et al. 8 ; primers for blaOXA-48 were those of Srinivasan et al. 9 ; primers for blaKPC gene were those of Poirel et al. 10 ; primers for blaGES were those of Hong et al. 11 ; and primers for blaNDM gene were those of Routray et al. 12 The PCR conditions were: initial denaturation at 95°C for 15 min, then 30 cycles of denaturation at 95°C for 30 sec, primer annealing at 50°C for 30 sec and primer extension at 72°C for 1 min, followed by final extension at 72°C for 10 min. The amplified products were visualized by UV light illumination after electrophoresis on a 2% agarose gel with ethidium bromide 0.5 μg/mL at a voltage of 120 amps for 45 min.
Conjugation studies for resistance transfer
Mating-out assays were done using A. baumannii isolates from patients as donors and A. baumannii BM 4547 as the recipient. 13 Both donor and recipient were cultured on blood agar plate at 37°C for 20 hr. One colony was taken from each donor and recipient and cultured in brain heart infusion broth (Oxoid, Basingstoke, Hants, United Kingdom) in a shaker incubator (100 agitations per minute) at 37°C for 1 hr. Conjugation was done by mixing 200 μL of the donor with 800 μL of the recipient and incubation in the shaker incubator at 37°C for 3 hr. From the conjugation mixture, 200 μL was plated on Tryptone Soya agar (Oxoid) containing ticarcillin (100 μg/mL) and rifampin (50 μg/mL) and examined for transconjugant colonies after incubation at 37°C for 24 hr. When required, transconjugants were tested for antimicrobial susceptibility as above.
Plasmid extraction
After a 24-hr aerobic growth of A. baumannii or transconjugant on blood agar at 37°C, plasmid extraction was performed according to Kado and Liu method. 14 Colonies were disrupted by lysing solution and DNA was extracted with phenol/chloroform. Water phase containing plasmids was further studied. Visualization of plasmids was done by mixing 25 μL of plasmid solution with 5 μL of gel loading buffer and agarose gel electrophoresis using 0.8% agarose gel containing 0.5 μg/mL ethidium bromide, at 120 mV for 3 hr. Bands were visualized under UV light. Plasmids from Escherichia coli V157 were used as molecular sizemarkers.
Plasmid purification from agarose gel
Gel containing plasmid was cut under UV light and placed in an Eppendorf vial. Plasmid extraction from the agarose gel was performed using the QIAquick Gel Extraction Kit according to the manufacturer's instructions (Qiagen, Hilden, Germany). After elution of the plasmid, 10 μL of the eluted plasmid solution was mixed with 2 μL of loading buffer for agarose gel electrophoresis. Electrophoresis was conducted on 0.8% agarose gel containing 0.5 μg/mL of ethidium bromide at 120 mV for 3 hr and then visualized under UV light. Plasmids from E. coli strain V157 were used as molecular size markers.
PCR for plasmid-mediated colistin resistance
PCR amplification of the plasmid-associated colistin resistance gene, mcr-1, was performed using the primers, CLR5-F (5′-CGGTCAGTCCGTTTGTTC-3′) and CLR5-R (5′-CTTGGTCGGTCTGTA GGG-3′) 15 with amplification conditions of 94°C for 15 min; followed by 25 cycles of 94°C for 30 sec; 58°C for 90 sec; 72°C for 60 sec with a final extension at 72°C for 10 min. The amplified product was run on a 2% agarose gel with 0.5 μg/mL ethidium bromide at 110 V for 2 hr. The gel was examined under UV light for a 309-bp product, which is indicative of plasmid-mediated colistin resistance. 16 An E. coli containing colistin-resistant plasmid (E. coli MRC1) provided by Professor Tibor Pal, University of United Arab Emirates (Al-Ain, UAE) was used as a positive control.
Statistical analysis
Median, interquartile range, 95% confidence interval, and difference of proportions were calculated by SPSS statistics, version 26 (IBM, Armonk, NY). A p-value of ≤0.05 was considered significant.
Results
A total of 493 patients were screened from March 2015 to June 2016. The prevalence of rectal colonization by A. baumannii was 23.73% (117/493). We then selected patients from whom A. baumannii was isolated on five consecutive occasions or more. A total of 32 patients (numbered as A, B, C, D, E, F, G, H, I, J, K, L, M, N, O, P, Q, R, S, T, U, V, W, X, Y, Z, AA, AB, AC, AD, AE, AF), colonized by 270 isolates of A. baumannii, met this selection criterion. The duration of monitoring the patients varied from 14 to 343 days (Supplementary Table S1).
Clinical and demographic data of patients
The clinical and demographic data of the 32 patients are shown in Table 1. Their median age was 65 years with an interquartile range of 69.75–50.25 years. The male to female ratio was 1:1. The majority of patients were Kuwaitis (21/32, 65.6%) and the remainder were expatriates: 3 patients (9.37%) each from India and Bangladesh, 2 patients (6.25%) from Iran, and 1 patient (3.12%) each from the Philippines, Syria, and Turkey. The median day before A. baumannii colonization was 4 days with a range of 1–35 days. Most of the patients had underlying diseases such as respiratory disease (14/32, 43.8%), cerebrovascular accident (6/32, 18.7%), or cardiac arrest (3/32, 9.4%). All patients received multiple antibiotics during their stay in the ICU. Ceftriaxone, meropenem, piperacillin/tazobactam, and colistin were the most commonly used antibiotics. These antibiotics were given as empirical treatment or in response to infections. The mortality rate was 56.2% (18/32). Seven patients (B, D, F, J, Q, Y, and AF) (Table 1) had only rectal colonization with no clinically proven infection with A. baumannii. The remaining 25 patients had infection with A. baumannii in addition to colonization of the rectum. In these patients, the organism was also cultured from 23 (71.9%) endotracheal secretion, 15 (46.9%) blood, 13 (40.6%) urine, 10 (31.2%) central line tip, and 1 (3.1%) peritoneal fluid specimens. All of these patients received colistin for the treatment of A. baumannii infection.
Clinical and Epidemiological Data of the 32 Patients Colonized by Acinetobacter baumannii
Interquartile range for age.
95% CI, 95% confidence interval.
Antibiogram of isolates
The antibiotic resistance data are summarized in Table 2. The prevalence of resistance to most antibiotics was very high. Imipenem, meropenem, piperacillin/tazobactam and tigecycline had very poor activities against the isolates with resistance rates of 87.04%, 85.18%, 91.11%, and 94.40%, respectively. The resistance rates against colistin and trimethoprim/sulfamethoxazole were 2.96% and 31.11%, respectively. Most of the isolates, 234 (86.7%), were MDR (resistant to ≥3 antibiotic classes). Detailed data are given in Supplementary Table S2. There was no consistent pattern of resistance in serial isolates nor was there any relationship with antimicrobial agents used to treat infections.
Minimum Inhibitory Concentrations of Tested Antibiotics Against Rectal Isolates of Acinetobacter baumannii from Intensive Care Unit Patients
MICs, minimum inhibitory concentrations.
Detection of carbapenem resistance genes
PCR analysis of 270 isolates showed that all the isolates harbored blaOXA-51. Also, 230 (85.1%), 35 (13.0%), 34 (12.6%), 15 (5.5%), 2 (0.7%), and 2 (0.7%) of the isolates carried blaOXA-23, blaIMP, blaOXA-24/40, blaGES, blaOXA-48, and blaOXA-58, respectively. The blaKPC, blaVIM, blaSIM, and blaNDM were not found (Fig. 1).
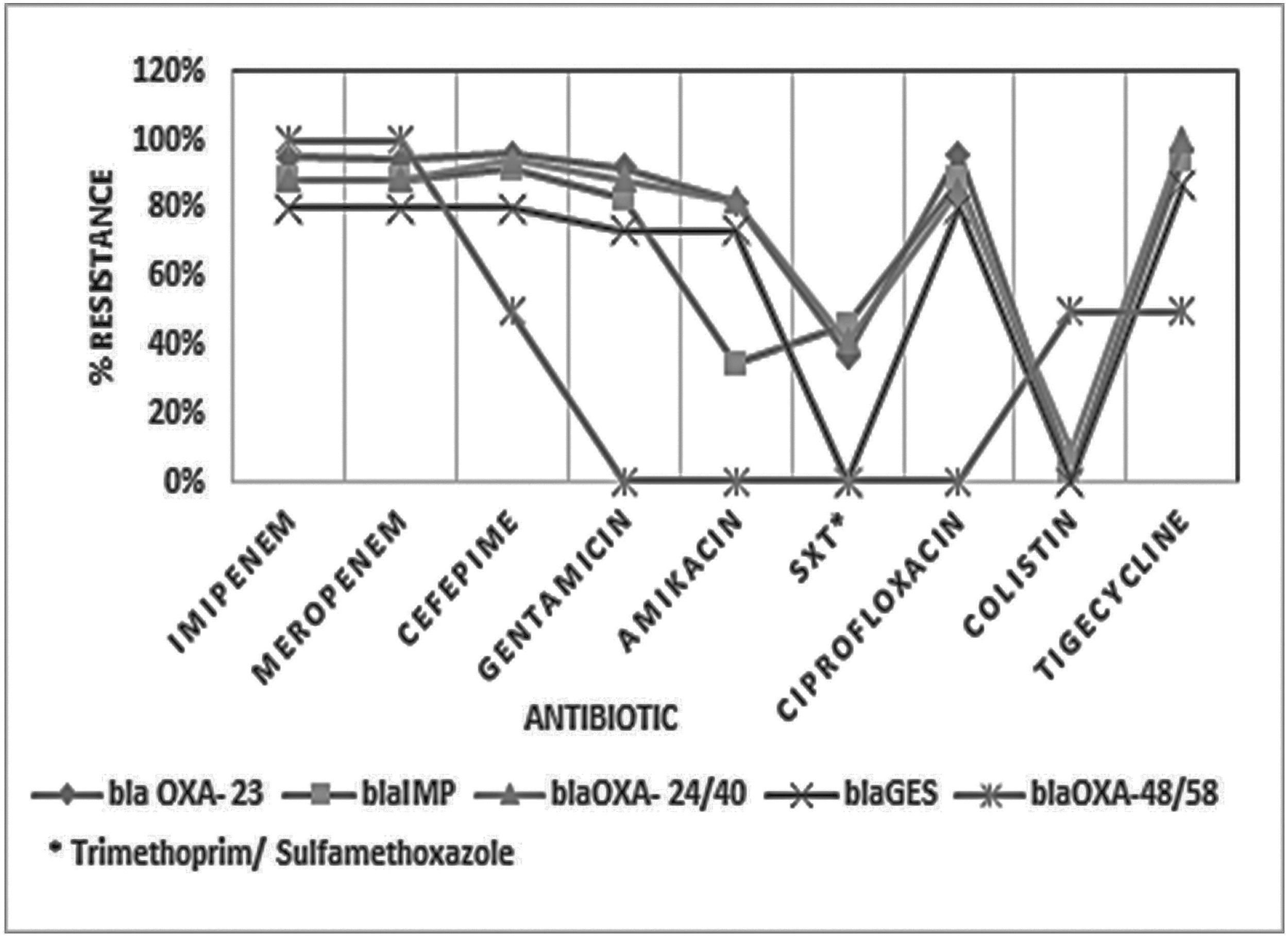
Prevalence of carbapenemase genes and resistance to antibiotics. The two isolates that possessed both blaOXA-48 and blaOXA-58 had identical antibiograms. Therefore, the corresponding resistance lines appear as a single line.
We considered an A. baumannii isolate carrying any carbapenemase gene as carbapenem-resistant A. baumannii (CRAB). The susceptibility of CRAB and carbapenem-susceptible A. baumannii (CSAB) to selected non-β-lactam antibiotics is shown in Table 3. There were significantly more isolates among CSAB that were susceptible to all antibiotics than CRAB isolates (p < 0.0001) (Table 3).
Susceptibility to Non-β-Lactam Antibiotics in Both Carbapenem-Resistant Isolates (Carbapenem-Resistant Acinetobacter baumannii) and Carbapenem-Susceptible Isolates (Carbapenem-Susceptible Acinetobacter baumannii)
Trimethoprim/sulfamethoxazole.
CRAB, carbapenem-resistant A. baumannii; CSAB, carbapenem-susceptible A. baumannii.
Plasmid profiling
Since the prevalence of A. baumannii harboring blaOXA-23, blaOXA-24/40, blaIMP, and blaGES were relatively high, 10 isolates positive for each of these genes were picked from different patients. The methods of selection of isolates for plasmid screening are described below. One or more isolates from all 32 patients were positive for blaOXA-23 representing a total of 238 isolates. The 238 isolates were written on small pieces of paper. The pieces of paper were rolled and mixed in a small box. Each piece was blindly picked one at a time. We wanted to select 10 isolates with 1 isolate from each of any 10 of 32 patients. If more than one isolate was picked from any patient, that pick was discarded until the pick came from a different patient. Thus, the picks were for isolates B1, E1, H3, L6, M2, P4, T5, R2, Z9, and AB3b. Some isolates from 10 patients (A, C, D, F, G, H, O, P, Q, Z) were positive for blaOxa-24/40. However, on the initial screening, isolates from patients, C and P were missed for the gene. Therefore, we selected a total of 10 isolates from the remaining 8 patients whose isolates tested positive on initial screening. The selected isolates were A5, D1, F2, F5, G1a, H4, O3, O6, Q1, and Z2a. Some isolates from 10 patients (A, C, I, O, P, R, U, V, Z, AB) were positive for blaIMP gene. However, on initial screening, the single isolate from patient U was missed for the gene. Therefore, a total of 10 isolates (A2, C2, I4, I8, O5, P1, R1, V1, Z2b, and AB2b) were selected from the remaining 9 patients. A single isolate from patient S, 8 isolates from patient W, and 6 isolates from patient AA were positive for blaGES gene, and a total of 10 isolates (S1, W3, W4a, W5a, W6, AA3a, AA3c, AA4a, AA4c, AA5) were selected. A total of four isolates (O1, O2, S5, S6) from two patients were positive for both blaOXA-48 and blaOXA-58 genes. However, on initial screening, both isolates from patient O were missed. Therefore, both isolates (S5, S6) from patient S were selected. Thus, a total of 42 isolates were selected for plasmid extraction studies (see Supplementary Table S2 for selection of patients marked in boldface letters). Plasmid extraction showed that A. baumannii carrying blaOXA-23 or blaOXA-24/40 had three plasmids of 35.8, 24, and 3 kbp each. Isolates with blaGES had two plasmids of 24 and 3 kbp, whereas isolates with blaIMP had a single plasmid of 35.8 kbp (Fig. 2). Those positive for blaOXA-48 or blaOXA-58 did not carry any plasmid. None of the plasmids from the 42 isolates carried blaOXA-51.
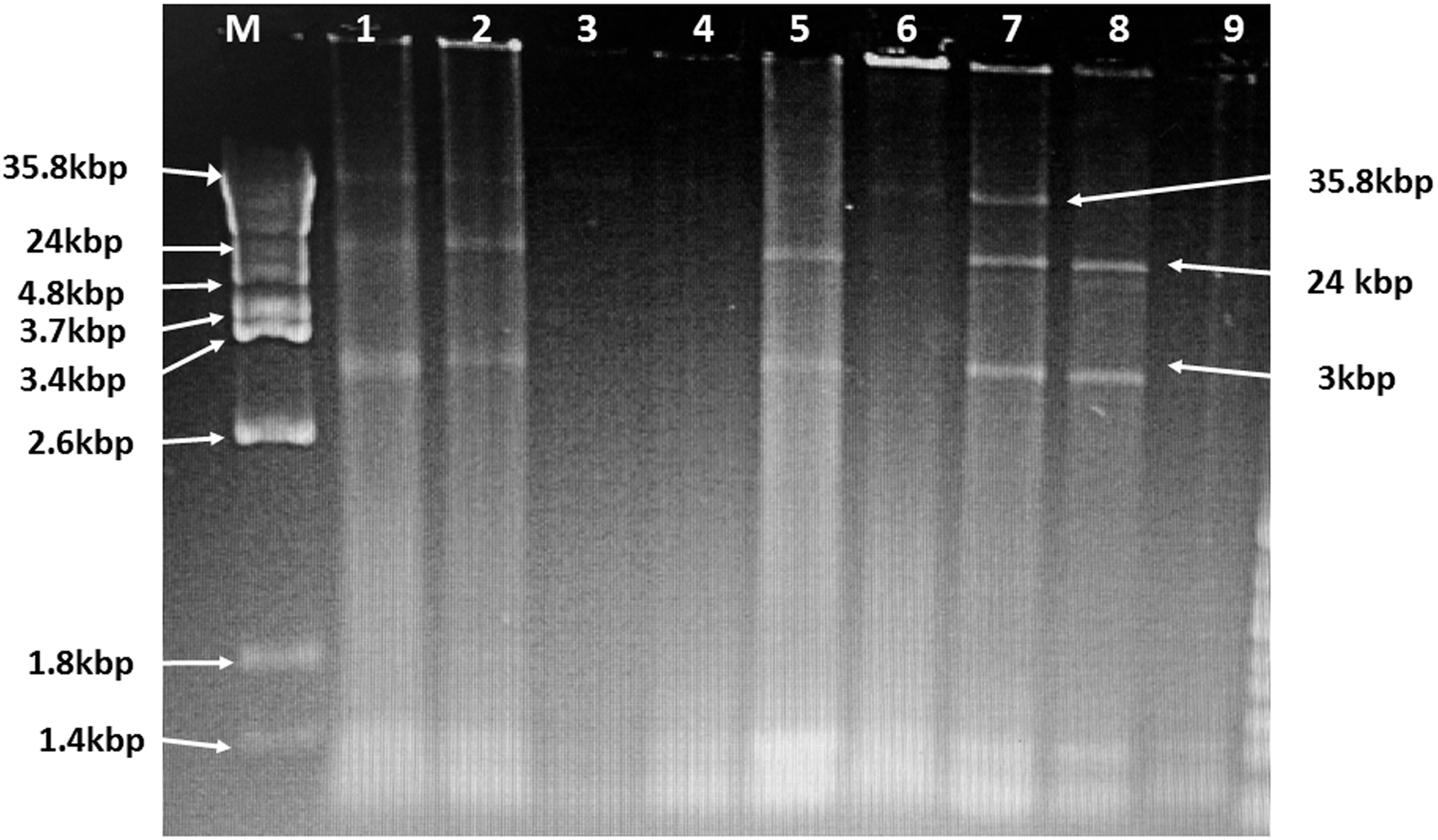
Gel electrophoresis of plasmids extracted from Acinetobacter baumannii isolates. Lanes 1 (blaOXA-23), 2 (blaOXA-23), 5 (blaOXA-24/40), and 7 (blaOXA-24/40) have 3 plasmids of 35.8, 24, and 3 kbp. Lane 8 (blaGES) has 2 plasmids of 24 and 3 kbp. Lanes 3 (blaIMP) and 6 (blaIMP) have a single plasmid each of 35.8 kbp, and lanes 4 (blaOXA-58) and 9 (blaOXA-48) have no plasmids.
Resistance transfer studies
Conjugation studies were performed on 12 isolates of A. baumannii, with a high-level resistance against the carbapenems, each carrying blaOXA-23 (3 isolates [B1, Z9, and R2]), blaOXA-24/40 (3 isolates [F2, O3, and H4]), blaIMP (3 isolates [Z2b, AB2b, and V1]) or blaGES (3 isolates [AA4a, AA5, and W5a]). All these 12 isolates were CRAB colistin susceptible. Plasmid transfer was obtained from isolates carrying blaOXA-23, blaOXA-24/40, blaGES, and blaIMP. The number of plasmids transferred from isolates varied from none to three. A. baumannii carrying blaOXA-23 and blaOXA24/40 had three plasmids of 35.8, 24, and 3 kbp and transferred all three of them. Isolates harboring blaGES carried two plasmids of 24 and 3 kbp sizes and transferred both of them. The single plasmid of 35.8 kbp size in the isolates harboring blaIMP was transferrable. Isolates positive for blaOXA-48 or blaOXA-58 gene did not carry any plasmids and hence were not used in conjugation studies. Transfer studies were also done using eight CRAB colistin-resistant A. baumannii as donors. These strains had three plasmids corresponding to blaOXA-23/blaOXA-24/40 or a single plasmid corresponding to blaIMP. PCR assay of transconjugants with mcr-1 primers did not result in a product for colistin resistance gene. Moreover, all transconjugants were susceptible to colistin (Table 4). The minimum inhibitory concentrations (MICs) of the above 12 colistin-susceptible and 8 colistin-resistant donor strains and their transconjugants were determined. The MICs of donors possessing the same resistance genes had identical MICs to their transconjugants for carbapenem and cephalosporin resistances, which were transferrable. The MICs of antibiotics tested against the donors harboring each gene type and their transconjugants are shown in Table 4.
Minimum Inhibitory Concentrations of Donor Strains and Transconjugants of Acinetobacter baumannii
Transconjugants obtained with all the tested donor strains possessing a particular resistance plasmid gave similar MIC levels for the tested antibiotics.
PCR amplification of extracted plasmids from donors and transconjugants
PCR amplification of extracted plasmids from all the isolates of A. baumannii carrying resistant genes, blaOXA-23 and blaOXA-24/40, showed that these genes resided in both large plasmids, 35.8 and 24 kbp. The small plasmid, 3 kbp did not carry any of these genes. For blaIMP and blaGES positive isolates, the gene was carried on the single large plasmid, 35.8 and 24 kbp, respectively.
Discussion
A. baumannii can cause serious infections in immunosuppressed patients and other vulnerable patients with chronic diseases, such as diabetes mellitus, hypertension, chronic respiratory disease, coronary artery disease, and cerebrovascular accident. 15 All the ICU patients in our study had chronic diseases that predisposed them to A. baumannii infection/colonization. The prevalence of A. baumannii colonization of the rectum of adult ICU patients in our study was 23.73%, which is similar to published data from other countries.17–19 Mortality rate among colonized/infected patients in our study was 56.2% compared with 61.6% in Israel. 20 Mean time to colonization was 4 days after admission in our study, which is similar to the previously published data. 21
Most of our isolates were MDR. Serial isolates from individual patients did not show any consistent resistance patterns. There was also no relationship to resistance against antibiotics administered to patients for treatment of infections. Reports of MDR A. baumannii are on the increase from hospitals in North and South America, Europe, and East Asia. 22 Resistance to carbapenems, glycylcyclines (tigecycline), polymyxin E (colistin), and trimethoprim/sulfamethoxazole is of interest as these drugs have been considered effective therapeutic agents in the past. Two decades ago, carbapenems were the drug of choice for treating A. baumannii infections, but are no longer effective due to acquisition of resistance by the organism. Imipenem resistance of rectal isolates in our study was 87% compared with 86.5% in Saudi Arabia, 23 and 91.3% in Turkey, 24 in clinical isolates. Similarly, meropenem resistance was 85.18% compared with 88.2% in Saudi Arabia, 23 and 91.30% in Turkey. 24 Resistance to tigecycline was very high in our study (94.4%) in contrast to an earlier report of 13.6% in clinical isolates from Kuwait by Al-Sweih et al. 25 Activity of tigecycline against clinical isolates in the past, even in outbreak situations, had been excellent. 2 A decade later, almost all the isolates, recovered from rectal swabs of patients in the same hospital setting, demonstrated a very poor activity against the drug.
In our present study, the prevalence of colistin resistance was about 3%, which is much lower than resistance rate of 12% reported in an earlier study from Kuwait. 26 This difference may be attributable to the method of susceptibility testing by E-test used in the earlier study as against the recommended agar dilution method. 6 In recent reports, no resistance to colistin was found in clinical isolates from Saudi Arabia 23 and Turkey. 24 The prevalence of 31% resistance to trimethoprim/sulfamethoxazole, in our study, was moderately high, but much lower than the high prevalence of 69.3% reported in Saudi Arabia 21 and 95.6% in Turkey. 24
In our study, characterization of the resistance genes demonstrated an abundance of carbapenem-hydrolyzing class D β-lactamase of the blaOXA-23 variety in a very high percentage of the isolates almost similar to the reports of 92% in Iraq 27 and 91% of pooled isolates from Saudi Arabia, United Arab Emirates, Kuwait, Qatar, Oman, and Bahrain. 28 blaOXA-24/40 was found in 13% of our isolates compared with the reported prevalence of 62.1% in Iran 29 and complete absence in Saudi Arabia. 28 blaOXA-58 was found in less than 1% of our isolates. Similarly, a rarity of this gene has been reported in Iran, 29 Iraq, 27 and Saudi Arabia. 28 Detection rate of class B metallo-β-lactamase genes was much lower than the class D genes. In this study, blaIMP was detected in 13% of our isolates similar to the 12% reported in Iran. 29 blaKPC, a class A β-lactamase gene and other class B genes, such as blaVIM, blaSIM, and blaNDM were not found in our study as well as in the collections from Saudi Arabia. 28 blaGES was detected in a relatively low single digit in our isolates, compared with only a single case so far in Saudi Arabia. 28 In an earlier study conducted on 65 invasive isolates from patients in the same unit of our hospital, the prevalence of this gene was 100%. 30
Carbapenem resistance was mediated by genes, such as the blaOXA-51, blaOXA-23, blaOXA-24/40, blaOXA-48, blaOXA-58, blaIMP, and blaGES (Fig. 1). Similar data exist with regard to blaOXA-51, blaOXA-23, and blaOXA-24/40 for many countries in the Gulf region, 28 Turkey, 24 and Egypt. 31 Carbapenem resistance mediated by blaOXA-58 and blaGES was also reported in Egypt 31 and Turkey. 24 Resistance mediated by blaOXA-48 has been reported in Iran 29 and Egypt. 31 Resistance mediated by blaIMP was found in other countries, including Hong Kong 32 and South Korea. 33
In our study, CRAB isolates were more resistant to non-β-lactam drugs than the CSAB isolates. This was consistent with the findings of other studies. 17 Plasmid-mediated antibiotic resistance in A. baumannii encoded by blaOXA-23, blaOXA-24/40, blaOXA-58, and. blaOXA-48 genes has been previously published. 34 Similarly, transferable resistance mediated by other genes, such as blaKPC, blaGES,30, blaNDM and blaVIM, 35 blaIMP, 36 and blaSIM 37 has been reported earlier. Conjugation experiments showed the transferability of blaOXA-23, blaOXA-24/40, blaIMP, and blaGES genes. Transferability was also reported for blaGES, blaOXA-23, blaIMP, and blaOXA-24/40. 38 In our study, none to three plasmids were carried by isolates, which was also described by Hamidian and Hall. 39 Plasmid carrying blaOXA-23 and blaOXA-24/40 were of 35.8 and 24 kbp, blaGES was carried on a 24 kbp plasmid, and blaIMP on a 35.8 kbp plasmid. The plasmid of 3 kbp did not carry any genes. Plasmid size carrying blaOXA-23, blaOXA-24/40, blaIMP, and blaGES ranged from 2 to >79.6 kb. 40
mrc-1 gene-mediated colistin resistance was not found among our colistin-resistant isolates even though, this was recently demonstrated in a single A. baumannii isolate from Pakistan. 41 As there is movement of people from Pakistan to Kuwait, this may lead to the introduction of this plasmid in the hospitals in Kuwait.
In conclusion, the study demonstrated that most of the isolates were MDR. However, the majority of the isolates were susceptible to colistin and nearly two-thirds susceptible to trimethoprim/sulfamethoxazole. There was no consistent pattern of resistance in serial isolates nor did the resistance bear any relationship to antibiotics administered to patients for treatment of infections. The strains carrying carbapenemase genes were MDR. Significantly, a greater number of CRAB isolates were resistant to non-β-lactam antibiotics compared with CSAB isolates. The four carbapenemase resistance genes studied, blaOXA-23, blaOXA-24/40, blaIMP, and. blaGES genes were carried on plasmids and they mediated resistance to all carbapenems in conjugation studies. Plasmid-mediated resistance to carbapenems is of concern because of the propensity to spread fast. Since resistance to colistin and trimethoprim/sulfamethoxazole is at a lower rate now, these can be reserved for treatment MDR A. baumannii infection.
Footnotes
Authors' Contributions
V.R. and M.A. developed the concept of the project; G.A. performed the work; G.A., M.A., and V.R. analyzed and interpreted the results; G.A. wrote the first draft of the article, and M.A. and V.R. edited the article.
Ethics Approval and Consent to Participate
Approval for the study was granted by the Ethics Review Committee of the Health Sciences Center/Ministry of Health (Approval No. 112). All patients gave informed written consent for rectal swab collection and data collection.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Kuwait University grant (No. YM03/15).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.