
Abstract
Objectives:
To identify the changing trends of uropathogens over the years 2010–2017 and examine the incidence of both antibiotic resistance and extended spectrum beta lactamases (ESBL)-producing Enterobacteriaceae in urine cultures from pediatric patients.
Study Design:
Electronic medical records of 1,056 children, admitted to the Poriya Medical Center in Israel, between 2010 and 2017 with positive urine cultures, were reviewed for bacterial species and antibiotics resistance.
Results:
The leading pathogen was Escherichia coli (76%), followed by Klebsiella (7%), Enterococcus (5.8%), and Proteus (4%). Statistically significant gender-specific and ethnicity-specific differences in the distribution of uropathogens were found. E. coli was more common in females compared to males. Escherichia coli constituted most (92.3%) of the ESBL-positive cultures, while only 4.6% isolates carried Klebsiella, 1.5% carried Enterobacter spp., and 1.5% carried Morganella. Prevalence of ESBL-producing E. coli increased throughout the study period. Increasing prevalence over time was noted for ceftriaxone, cefuroxime, amoxicillin/clavulanate, and ampicillin resistance.
Conclusions:
Gender and ethnic background should be taken into consideration when choosing empiric antibiotic therapy for urinary tract infections in children. Similarly, the continuous increase in resistance to cefuroxime and amoxicillin/clavulanate should be considered when prescribing therapy in Israel. Ceftriaxone and gentamicin are still the antibiotics of choice for inpatient parenteral empiric treatment.
Introduction
Gram-negative bacteria constitute the most common cause of urinary tract infections (UTIs) in children. 1 In a 2013 study that examined more than 25,000 urinary isolates, Escherichia coli was the leading pathogen in urinary samples of pediatric UTI patients, with a prevalence of 83% in girls and 50% in boys. Additional common species among boys with UTI were the Gram-positive Enterococcus spp. (17%) and the Gram-negative rods Proteus mirabilis (11%) and Klebsiella spp. (10%). 2
The distribution of uropathogens and their antibiotic susceptibility can change with time and geographic area.3–6 In 2016, the American Academy of Pediatrics (AAP) UTI clinical guidelines reaffirmed that empiric therapy for UTIs should be based on local antimicrobial susceptibilities. The recommended oral treatment is first- or second-generation cephalosporins, amoxicillin/clavulanate, and trimethoprim-sulfamethoxazole (TMP-SMX). As for parenteral treatment, antibiotics such as third-generation cephalosporins, gentamicin, or piperacillin are suggested, until the treatment is adjusted to the identified uropathogen and its antimicrobial susceptibilities.7,8 In 2014, the Israeli Medical Association UTI guidelines recommended empiric therapy with first-generation cephalosporins for lower UTIs and first- and second-generation cephalosporins or amoxicillin/clavulanate for upper UTIs. 9
In light of the high resistance rates that have developed in recent years, the American and European societies suggested that initial empiric therapy for infectious diseases should only be given if the local antibiotic resistance is lower than 20%. 10 Subsequent assessments found that ampicillin and TMP-SMX are unsuitable for first-line treatment in several OECD countries. 11
In a study performed in 2013 in the USA, E. coli isolated from pediatric urine cultures showed high rates of antibiotic resistance, that is, 24% for TMP-SMX, 1% for nitrofurantoin, and 15% for cephalothin. In comparison to resistance rates in 2002, the 2013 E. coli resistance rates increased for TMP-SMX (from 23% to 31% in males and from 20% to 23% in females) and ciprofloxacin (from 1% to 10% and from 0.6% to 4%, respectively). 2 One of the common resistance mechanisms is mediated by extended spectrum beta lactamases (ESBL) enzymes, which confer resistance to cephalosporin and penicillin, and has been shown to extend hospital stay and require a change of treatment in many cases. 12 In Shaare Zedek Medical Center, Jerusalem, the prevalence of UTI caused by ESBL-producing bacteria has increased from 2% to 3.8% during a 10-year study period (between 2003 and 2013). 13 This study aimed to identify the trends in uropathogen distribution and their antibiotic susceptibilities among the northern pediatric population in Israel, and to determine optimal empiric therapy for UTI in the region.
Materials and Methods
Study design
This retrospective study reviewed the electronic records of children 0–15 years of age (10 days–14.7 years), admitted between January 2010 and December 2017 to the Baruch Padeh-Poriya Medical Center, Galilee region, northern Israel, with a positive urine culture that was later affirmed in the institute. It is important to note that the study examined urine cultures of children, which were identified as positive by the clinical microbiology laboratory at the medical center, however, not necessarily diagnosed with UTI. Data collected included age, gender, season of birth, ethnic background, type of settlement, and the season in which the culture was taken.
This study was authorized by the institutional review board and requirement for informed consent was waived (POR 0038-17).
Urine culture
To confirm bacterial infection, urine samples were sent to the clinical microbiology laboratory at the medical center. Samples (10 μL [suprapubic aspiration (SPA)] or 1 μL [all other samples]) were inoculated on MacConkey and Orientation agar (Hy Laboratories Ltd., Rehovot, Israel), at 36 ± 1°C, in 5% CO2, for 24–48 hours. Samples were then assessed according to the laboratory's routine protocol that defines a positive urine culture in the event of
Any bacterial growth for SPA
Over 105 colony-forming units (CFU) for urethral catheterization
Over 105 CFU for two midstream or urine bag collections (although urine bags are not considered a proper collection method these days, in certain situations, it was the only possible route of urine collection).
Cultures with fewer CFUs, mixed growth, or two isolates of different pathogens were not included in the study. Repeat urine cultures obtained during the same admission were excluded, unless they revealed a change in pathogen.
Pathogen identification and antibiotic susceptibility testing
Bacterial identification was carried out using Matrix-assisted laser desorption/ionization time-of-flight systems (Bruker Daltonics, Bremen, Germany). Following identification, several colonies were suspended in saline to a turbidity of 0.5 McFarland. For antibiotic susceptibility testing (AST), the suspension was then loaded onto an automated VITEK2® (bioMérieux SA, France) and assessed according to the standards of the Clinical and Laboratory Standards Institute (CLSI). Susceptibility to the following antibiotics was tested: gentamicin, TMP-SMX, amoxicillin/clavulanate, ampicillin, nitrofurantoin, and cephalosporins. Testing for ESBL was also performed. For quality control the E. coli ATCC25922, Klebsiella pneumoniae ATCC700603, Pseudomonas aeruginosa ATCC27853, Enterococcus faecalis ATCC29213, and Staphylococcus aureus ATCC29213 were was used.
Statistical analysis
All measured variables and derived parameters were tabulated by descriptive statistics. For categorical variables, summary tables provide sample size, and absolute and relative frequencies. The Chi-square test was applied to analyze the differences in proportions between the years and between demographic characteristics.
A general linear regression model was applied to determine p-value for trends over time. Logistic regression was applied to analyze the distribution of the types of bacteria over time. All tests were two tailed, and a p-value of ≤5% was considered statistically significant. The data were analyzed using SAS® version 9.3 (SAS Institute, Cary, NC).
Results
A total of 1,056 positive urinary culture records were included in the study, with the following yearly distribution: 112 during 2010, 108 during 2011, 133 during 2012, 154 during 2013, 153 during 2014, 134 during 2015, 139 during 2016, and 123 during 2017 (Table 1). Patients were between the ages of 10 days and 14.7 years and most were female (82.4%). Ethnic backgrounds were primarily Jewish (48.4%) and Arab (47.2%) and most lived in urban areas (42%) or in villages (39.2%) (Table 1). Samples were collected from mid-stream urine (n = 405; 38.4%), a urine bag (n = 55; 5.2%), transurethral catheter (n = 474; 44.9%), SPA (n = 120; 11.3%), or nephrostome (n = 2; 0.2%).
Demographic and Baseline Data
The leading pathogen with a prevalence of 76% was E. coli, followed by Klebsiella spp. (7%), Enterococcus spp. (5.8%), P. mirabilis (4%), P. aeruginosa (2.8%), and others (4.4%), including Acinetobacter spp., Citrobacter spp., Enterobacter spp., Morganella morganii, and S. aureus (Table 2).
Distribution of Pathogens During the Years 2010–2017
A statistically significant gender-specific difference in pathogen prevalence was observed (p < 0.0001), with E. coli being more common among females compared to males (81% vs. 53.2%, respectively). Klebsiella spp. (12.4%) and Enterococcus spp. (17.2%) were more prevalent in males compared to females (6.0% and 3.3%, respectively) (Fig. 1). Uropathogen prevalence also exhibited distinct distribution patterns between the different ethnic groups (p = 0.0064) (Fig. 2). Escherichia coli was more common in Arab compared to Jewish children (78.7% vs. 72.2%, respectively), while Jewish children more commonly carried Enterococcus spp. (7.2%), P. mirabilis (5.5%), and P. aeruginosa (3.5%) compared to Arab children (4.8%, 2.4%, and 1.8%, respectively).
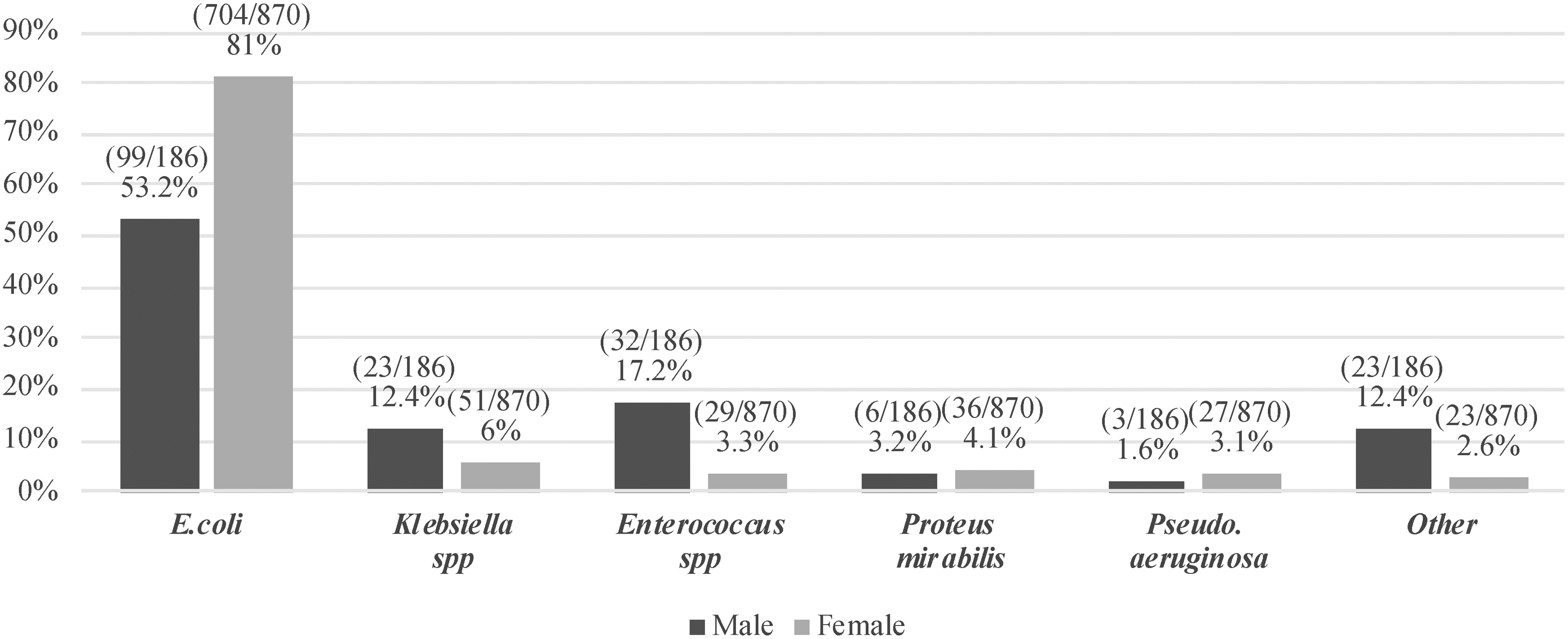
Pathogen distribution in relationship to gender (p < 0.0001).

Pathogen distribution according to ethnic groups (p = 0.0064).
No statistically significant differences were found in pathogen prevalence in relationship to type of settlement or the season in which the urine culture was collected (data not shown). Among the 65 ESBL-positive cultures, 60 (92.3%) carried E. coli, 3 (4.6%) carried K. pneumoniae (1 case per year [2011, 2012, 2017]), 1 (1.5%) carried Enterobacter spp., and 1 (1.5%) carried M. morganii (2017). A trend of increasing prevalence of ESBL-positive E. coli samples was noted along the study years (p < 0.0001, Fig. 3), from 1.1% in 2010 up to 19.4% of all E. coli-positive isolates in 2016 (19/98). No significant difference was found in the prevalence of ESBL-producing bacteria in relationship to gender, ethnic background, type of settlement, season of birth, or season of culture.

Percentage of ESBL-producing Escherichia coli from total E. coli isolates (p < 0.0001, p-value for trend over time). Linear line represents increasing trend. ESBL, extended spectrum beta lactamases.
An increase in antibiotic resistance over time was noted in the study period (Table 3). Resistance to ceftriaxone increased from 2% in 2011 to 14.7% in 2016 (p = 0.0025) and resistance rates to cefuroxime were as high as 18.2% in 2016 versus 4% in 2010 (p = 0.0031). Resistance to amoxicillin/clavulanate increased from 9.6% in 2012 to 34.4% in 2016 (p < 0.0001). During the years 2010–2017, over 30% of the isolated bacteria were resistant to ampicillin, with 33% showing resistance in 2010 and 76.4% showing resistance in 2014 (p = 0.0044). While no change in cephalothin resistance rates were noted during the study period (p = 0.22), a high resistance of 36.9% was recorded in 2016. Similarly, no significant changes in resistance to TMP-SMX, gentamicin, and nitrofurantoin were seen over time. Overall, with the exception of 2017, TMP-SMX resistance exceeded 20% each year, with a peak rate of 39.5% recorded in 2016.
Percentage of Antibiotic Resistance to Antibiotics During the Years 2010–2017
p-value for trend over time. Bold represents statistically significant p-value.
TMP-SMX, trimethoprim-sulfamethoxazole.
Discussion
UTI is one of the most common bacterial infections in children. Initiation of appropriate empirical therapy for pediatric patients is very important to avoid complications, such as renal scarring. However, owing to the increasing rates of resistant bacteria and their significant influence on the guidelines for initial empiric therapy for UTIs, periodic determination of local resistance trends is necessary. In this study, we examined pathogen distribution and trends in antibiotic resistance in pediatric urine cultures collected in the northern region of Israel over an 8-year period (2010–2017). Escherichia coli was found to be the most common pathogen in urine cultures, with an overall prevalence of 76%. This finding is consistent with those reported in Israel in 2014, when E. coli prevalence was as high as 80.5%, 14 higher than rates reported in North America during this period (47–58%),15–17 but similar to rates reported in Europe (48–86%). 17
The second most common pathogen in our study was Klebsiella spp. (7%), followed by Enterococcus spp. (5.8%), P. mirabilis (4%), and P. aeruginosa (2.8%). An Israeli study published in 2015 found similar rates of K. pneumoniae (5.9%), E. faecalis (3.9%), P. mirabilis (3.5%), and P. aeruginosa (1.5%) in children with a first episode of UTI. 14 An analysis of Omani children with their first documented UTI between 2008 and 2012 identified K. pneumoniae in 17% of samples, which was reported to be a causative organism for UTI in other reports18–20 as well. Our analysis demonstrated that patient gender should be taken into consideration when choosing empiric treatment for UTI. A statistically significant (p < 0.0001) gender-specific pathogen distribution was noted, with a higher prevalence of E. coli among females compared to males (80.9% vs. 53.2%, respectively), while Klebsiella spp. (12.4% compared to 5.9%), Enterococcus spp. (17.2% compared to 3.3%), and P. aeruginosa (3.1% compared to 1.6%) were more common in males compared to females. Similar associations between E. coli infections and females or P. aeruginosa infections and males were seen in other works.1,21,22 As P. aeruginosa is an opportunistic uropathogen in community-acquired UTI 23 and also resistant to first-line empiric antibiotics, 20 characterization of groups at risk for P. aeruginosa UTI may improve treatment decision-making processes. Such data were published in other studies stating male gender as a risk factor along with other host characteristics as well. 21
Differences in pathogen distribution were also seen in relationship to different ethnic backgrounds; E. coli was more common among children of Arab origin (78.7% compared to 72.2% in Jewish origin), while Enterococcus spp. (7.2% compared to 4.8%), P. mirabilis (5.5% compared to 2.4%), and P. aeruginosa (3.5% compared to 1.8%) were more common among Jewish children. An Israeli study published in 2017, comparing uropathogens isolated from a Bedouin population versus those isolated from the general population in southern Israel, showed similar pathogen distribution in both populations. However, the substantial percentage of pathogens that were resistant to standard first-line antibiotics demanded a change in the empiric therapy for the Bedouin population hospitalized for UTIs. 24 The implications of ethnic background on empiric antibiotic therapy in our region will require further investigation.
Cefuroxime resistance rates increased over time (p = 0.0031), peaking at 18.2% in 2016 compared to 4% in 2010. A similar increase was noted for amoxicillin/clavulanate (p < 0.0001), with 10.9% of samples showing resistance in 2010, versus 34.4% in 2016. In an earlier analysis, performed by the same group, of uropathogen distribution in samples collected between 2003 and 2015, a similar increase in the resistance rate to ampicillin/clavulanate (10–38.17%) was noted. 14 In a meta-analysis published in 2016, covering more than 77,000 E. coli-positive urine isolates in OECD countries, resistance to amoxicillin/clavulanate was recorded in 8.2% of samples, while 60.3% of samples collected in countries outside the OECD showed resistance to amoxicillin/clavulanate. 11 Cefuroxime and amoxicillin/clavulanate are common outpatient antibiotics prescribed in Israel. Although our results showed a continuous increase in resistance, our study population comprised children admitted to the emergency room; therefore, no conclusion can be drawn about antibiotic resistance and empiric therapy for the general outpatient population. For TMP-SMX, with the exception of 2017, bacterial resistance exceeded 20% every year, peaking at 39.5% in 2016. While cephalothin resistance remained constant throughout the study period (p = 0.22), resistance rates were as high as 36.9% in 2016.
The tested antibiotics were commonly administered in the previous decade, but have since been found inadequate for empiric therapy. A retrospective study performed in 2017 in Israel, on 829 pediatric urinary isolates, found that the resistance rate of E. coli to ampicillin and first-generation cephalosporins reached ∼60% and to amoxicillin/clavulanate and TMP-SMX, nearly 30%. 25 During the years 2010–2017, over 30% of the isolated bacteria were resistant to ampicillin, with an increasing trend (p = 0.0044) from 33.3% in 2010 to a peak resistance rate of 76.4% in 2014. According to our results, ampicillin should remain as a treatment, specifically for UTIs caused by Enterococcus spp.
As for inpatients, ceftriaxone and gentamicin are the antibiotics of choice for parenteral empiric treatment. An increasing trend in bacterial resistance to ceftriaxone was noted (p = 0.0025), but never exceeding 20%. Another study performed in Israel during the years 2007–2014 reported ceftriaxone resistance rates of common pathogens to be ≤4.2%. 25 Similarly, a study published in 2013 in the USA reported on a resistance rate of less than 2% among 25,418 outpatient urinary isolates. 2 In our study, the yearly resistance rates to gentamicin remained stable and never exceeded 9%. Similar results regarding bacteria resistance to gentamicin were seen in the latter two publications, with the exception of P. mirabilis (16%) in the Israeli study. In contrast, an 11-year analysis of changing patterns of E. coli antibiotic resistance in 38,530 community UTIs between 1999 and 2009 in Dublin noted that E. coli. resistance to gentamicin increased from 0.4% in 1999 to 4.8% in 2009, with a resistance rate change of 0.4% per year over that period. 26 Considering our results and the other mentioned publications, we still find these antibiotics the most relevant for empiric parenteral treatment. Nevertheless, continued monitoring of resistance trends is of critical importance, as is avoidance of overuse.
This study recorded an increasing prevalence of ESBL-producing E. coli bacteria over time (p < 0.0001), and a large majority of E. coli (92.3%, 60/65) versus low prevalence of Klebsiella spp. (4.6%, 3/65) in ESBL-positive samples. An article published in 2016, reporting on analysis of 7,374 cases of UTIs in children, found that 14% (1 of 7) were caused by ESBL-producing Enterobacteriaceae. 12 In a study conducted in northern Israel between the years 2008 and 2011, community-acquired ESBL-positive UTI (CA-ESBL-UTI) was evident among children in every year of the study, with a yearly incidence of 1.2–5.8% and a significant increase in incidence over time. 27 Our study showed a continuation of this trend during the years 2010–2017. Moreover, the latter study indicated a higher resistance rate (48%) of these bacteria to gentamicin when compared to our study (29.2%, 19/65). To overcome the difficulty of choosing an appropriate empiric regimen for pyelonephritis, considering that ampicillin plus gentamicin is a common empiric protocol for pyelonephritis, they decided to change the regimen to ampicillin plus amikacin for children admitted with febrile UTI, and considered to be at risk for CA-ESBL-UTI (recent hospitalization, previous UTI episodes, urinary tract anomalies, receipt of cephalosporin UTI antimicrobial prophylaxis, and UTI with Klebsiella spp.). 27 Our department will reconsider our empiric therapy regimen in such cases and continue investigating this phenomenon.
An interesting find in our study was that, in contrast to the rising prevalence of ESBL-producing E. coli, the prevalence of other ESBL-producing bacteria, specifically Klebsiella spp., showed no increase at all, and never exceeded more than a single case per year of the study period. In a systematic review and meta-analysis studying the prevalence of ESBL-producing Enterobacteriaceae (ESBL-PE) in pediatric UTIs, a multivariate analysis of data from 385 UTI cases showed that the most common ESBL-PE isolates were E. coli (64.4%) and Klebsiella spp. (31.9%). 12 Studies performed in Israel showed significantly higher proportions of Klebsiella spp. in the ESBL-UTIs. A study performed in Jerusalem (published in 2014) found K. pneumoniae to be the causal pathogen in 15% (out of total 80 cases) of CA-ESBL-UTI cases, 13 while in our Galilee region study, an even higher prevalence of 24% of all CA-ESBL-UTIs was recorded. 27 It should be restated that our study examined positive urine cultures that were not necessarily collected from UTI patients. The significantly lower incidences of ESBL-producing Klebsiella spp. in our study should be further investigated.
In conclusion, there were significantly distinct gender-specific and ethnic background-specific distributions of uropathogens among children in northern Israel. The findings reported in this study should be considered when choosing appropriate empiric therapy for UTI. Cefuroxime and amoxicillin/clavulanate are commonly administered in the outpatient setting for UTI, yet, due to the population included in this study, no conclusion can be drawn about antibiotic resistance and empiric therapy for outpatient populations. As for inpatients, ceftriaxone and gentamicin are still the antibiotics of choice for parenteral empiric treatment. Ampicillin should remain as treatment specifically for UTIs caused by Enterococcus species. Due to the increasing prevalence of ESBL-producing E. coli bacteria in the past few years, we should reconsider our empiric therapy regimens in specific risk groups. On the other hand, no increase in the prevalence of ESBL-producing Klebsiella spp. was noted during the years of our study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.