
Abstract
The spread of resistance to vancomycin and other last-resort drugs in Enterococcus spp. remains of concern. In Italy, surveillance data for enterococcal bloodstream isolates in humans are scant. The aim of our study was to assess the incidence trends of bacteremias due to Enterococcus species and their prevalence trends of antimicrobial resistance. We retrospectively included all consecutive not-duplicate Enterococcus species isolated from blood cultures, in patients from 11 Italian hospitals (2011–2017). Incidence was defined as the number of isolates per 10,000 patient-days, while resistance prevalence was defined as the number of resistant strains divided by the number of tested strains. We included 4,858 isolates (59%, 36%, and 5% due to Enterococcus faecalis, E. faecium, and other Enterococcus spp., respectively). Over the study period, the incidence of bacteremias due to E. faecalis (incidence rate ratio [IRR]: 1.02, 95% confidence interval [CI]: 1.00–1.04, p = 0.008) and E. faecium increased (IRR: 1.03, 95% CI: 1.01–1.05, p < 0.001) alongside with the whole enterococcal bacteremias trend (IRR: 1.02, 95% CIs: 1.01–1.04, p = 0.002). A progressive increase in vancomycin-resistant E. faecium (VREfm) bacteremias was observed. Resistance to tigecycline and linezolid was rarely reported. The incidence of enterococcal bloodstream isolates is increasing in Italy, together with the prevalence of VREfm. Resistance to linezolid, a cornerstone drug used in the treatment of VRE bloodstream infection, remains negligible.
Introduction
E
Global data trends on vancomycin resistance in Enterococcus faecium are heterogeneous: increasing trends have been reported in Europe and in Eastern Mediterranean regions6,7; decreasing trends have been reported in the United States. 8 In other part of the world, vancomycin resistance in enterococcal infections does not represent a major issue.9–11
In Italy, several microbiology laboratories adhere to a national antibiotic resistance surveillance project (AR-ISS), whose data merge in the European Center for Disease Prevention and Control (ECDC)-coordinated European Antimicrobial Resistance Surveillance Network (EARSS). However, surveillance for antibiotic resistance reporting Italian data on enterococcal isolates from blood cultures is limited to outdated epidemiological reports, particular settings, or single-center experiences.12–15 Furthermore, data regarding the antimicrobial resistance of clinical enterococci are partial and obsolete.16–20
Until 2013 the incidence of vancomycin-resistant enterococci VRE BSIs was decreasing in Italy, but recent data from the last ECDC report showed a worrisome increasing trend of vancomycin-resistance rates in E. faecium21,22; in addition, decreased susceptibility to last-resort drug such as daptomycin, linezolid, and tigecycline is being increasingly reported in other European countries.23–25
Given these worrisome progressions and to investigate the present incidence of enterococcal bacteremia and their antibiotic susceptibility, we performed a multicentric study from 11 Italian hospitals localized in 9 out of 20 Italian regions collecting and analyzing data from Enterococcus species isolated from blood cultures. The primary study objective was to assess the trend in the incidence of bacteremia due to Enterococcus species. The secondary objective was to determine the trend in the prevalence of antimicrobial resistance in Enterococcus spp. isolated from blood cultures.
Materials and Methods
We retrospectively included all consecutive Enterococcus spp. isolated from blood culture, from January 1, 2011 to December 31, 2017, collected in 11 Italian hospitals (Supplementary Table S1). Enterococcal “bacteremia” was defined as the isolation of Enterococcus spp. from blood culture.
Duplicate blood cultures (up to 30 days following the last positive culture for the same Enterococcus spp.) from the same patient were excluded from analyses. Polymicrobial isolates were not excluded.
We extracted the following patient data from the records meeting the inclusion criteria: age, gender, nationality, and patient location (medical or surgical wards, intensive care units, oncology or hematology wards, and outpatient settings).
Species identification of isolates and their antimicrobial susceptibility profiles were obtained with different automated systems, employing gradient diffusion tests when deemed necessary according to every single laboratory protocol (Supplementary Table S1). Results of susceptibility testing for ampicillin, gentamicin, vancomycin, teicoplanin, linezolid, and tigecycline were collected in each single hospital laboratory and interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. 26
Incidence of enterococcal bacteremia was calculated as the number of episodes per 10,000 patient days, whereas the prevalence of antimicrobial resistance was calculated as the number of resistant strains by the total number of tested strains. Changes in the incidence of enterococcal bacteremia during the study period (measured as incidence rate ratio[IRR]) were assessed employing generalized linear mixed models based on Poisson or negative binomial regressions, according to the absence or presence of overdispersion in count data, respectively. Time in 3-month periods was the independent variable in all models, and center was included both as a random intercept and a random slope. Prevalences of resistance, cumulatively considering the entire study period, was assessed descriptively with number and percentages.
In addition, changes in the prevalence of ampicillin resistance, vancomycin resistance, and gentamicin resistance for both Enterococcus faecalis and E. faecium over the study period were assessed using the Cochran–Armitage test for trends in proportions. The analyses were performed using the lme4 and DescTools packages for R Statistical Software 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria). A p-value ≤0.05 was considered to indicate statistical significance.
Our study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethics approval (n° 164/2018) was obtained by the Ethics Committee of the coordinator center (Azienda Sanitaria Universitaria Giuliano Isontina, Trieste, Italy).
Results
From 2011 to 2017, we included 4,858 consecutive nonduplicate blood cultures, with an overall incidence of 3.17 episodes of enterococcal bacteremia per 10,000 patient days. Most enterococcal bacteremias affected male patients (60.7%) with a mean age of 68.6 years (median: 72, interquartile range [IQR]: 60–80 years). Patients were mostly Italian (n = 4,724; 97.2%) and were admitted mainly to medical wards (n = 2,590; 53.3%), followed by intensive care units (n = 1,109; 22.8%), surgical wards (n = 803; 16.5%), oncology and hematology wards (n = 308; 6.3%). The median number of episodes per center was 393 (IQR 207–536).
Results regarding species identification and antimicrobial susceptibility are summarized in Table 1. E. faecalis was isolated from 2,866 blood cultures (59% of all blood cultures), followed by E. faecium (n = 1,739; 35.8%), Enterococcus gallinarum (n = 69), Enterococcus avium (n = 56), Enterococcus casseliflavus/flavescens (n = 53), Enterococcus durans (n = 21), Enterococcus raffinosus (n = 14), and Enterococcus hirae (n = 4). Other less-frequent or unidentified enterococcal species were isolated in 36 cases (0.7%). Resistance to linezolid and tigecycline remained low during the study period. We noticed a high inter-hospital variability both in performed antimicrobial susceptibility tests and in resistance distributions (as shown in Supplementary Table S1, focusing on vancomycin-resistant E. faecium [VREfm]).
Overall Species Identification and Antimicrobial Susceptibility Results (from 2011 to 2017)
a: E. gallinarum and E. casseliflavus/flavescens are intrinsically resistant to vancomycin, but low MIC strains (2–4 mg/L) might have been reported as susceptible by automated antimicrobial susceptibility testing. Percentages are marked in bold.
HD, high dose; i.e., gentamicin MIC >128 mg/L; MIC, minimal inhibitory concentration; R, resistant isolates (n); T, tested isolates (n).
As shown in Table 2, the overall incidences of bacteremia due to E. faecalis and E. faecium were 1.87 and 1.13 episodes per 10,000 patient days, respectively. Table 2 and Fig. 1 also show the trends in the incidence of enterococcal bacteremia during the study period. Both the incidence of enterococcal bacteremia independent of species (IRR: 1.02, 95% confidence intervals [CIs]: 1.01–1.04, p = 0.002) and those of E. faecalis (IRR: 1.02, 95% CI: 1.00–1.04, p = 0.008) and E. faecium (IRR: 1.03, 95% CI: 1.01–1.05, p < 0.001) considered separately increased over the study period, although with the presence of inter-center variability as testified by the results of the random effects component of the model (Table 2).

Incidence rates of bacteremia due to overall Enterococcus spp., E. faecalis, and E. faecium from January 2011 to December 2017. The study period was divided into 3-month periods from January 2011 to December 2017. Dotted lines represent linear trends for descriptive purposes.
Trends in the Incidence of Enterococcal Bacteremia (from 2011 to 2017)
A p-value ≤0.05 was considered statistically significant.
CI, confidence interval; IRR, incidence rate ratio; SD, standard deviation.
As shown in Fig. 2, over the study years the following statistically significant changes (p < 0.05 for trend in resistance proportions) were observed: (1) a decrease in the prevalence of high-level gentamicin resistance for E. faecalis; (2) an increase in the prevalence of vancomycin and ampicillin resistance, and a decrease of high-level gentamicin resistance for E. faecium.
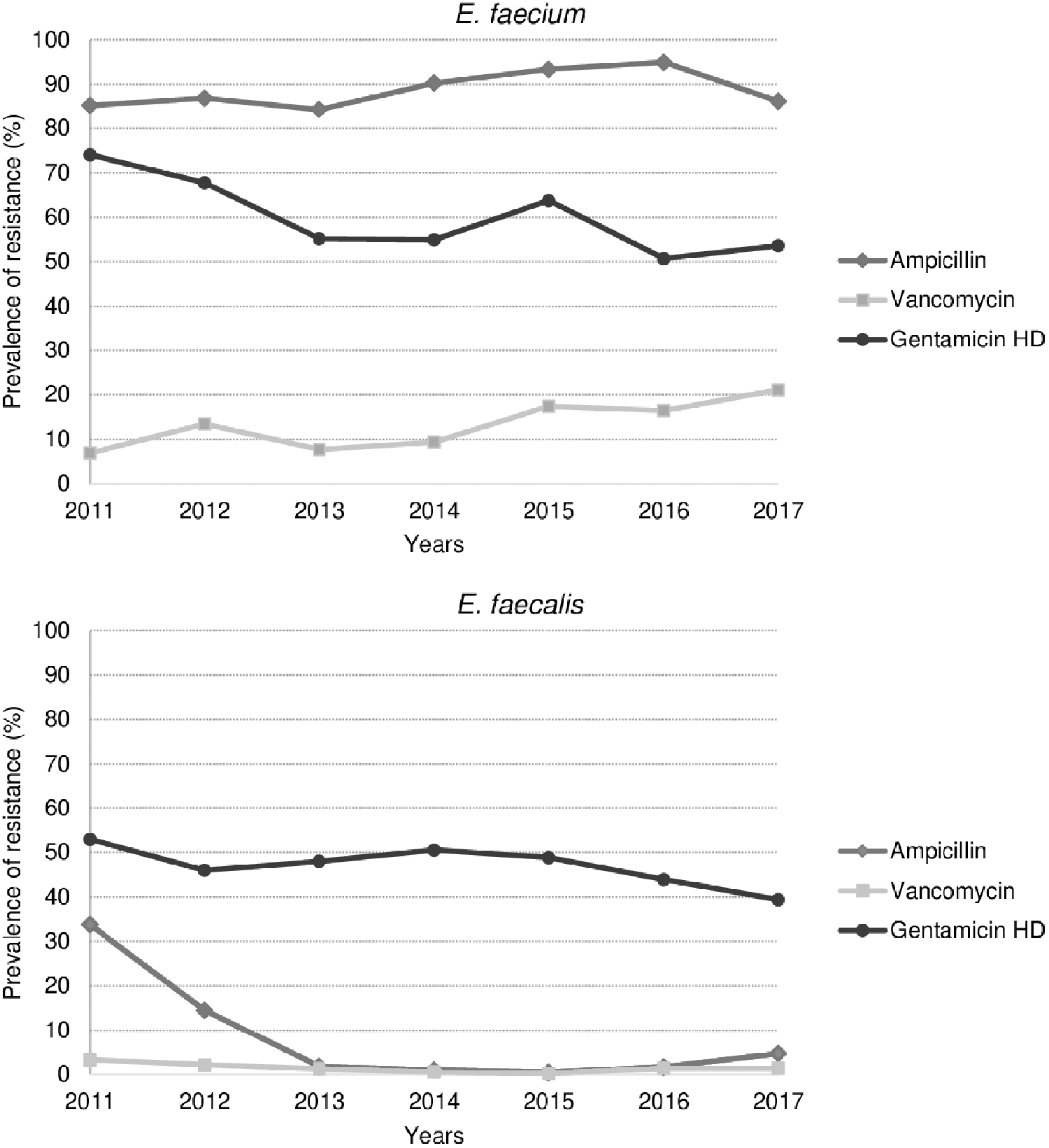
Trends in antibiotic resistance of Enterococcus faecium and Enterococcus faecalis from January 2011 to December 2017. Over the study years, the following statistically significant changes (p < 0.05 for trend in resistance proportions) were observed: (1) a decrease in the prevalence of high-level gentamicin resistance for E. faecalis; (2) an increase in the prevalence of vancomycin and ampicillin resistance, and a decrease of high-level gentamicin resistance for E. faecium. Ampicillin resistance in E. faecalis in 2011–2012 was limited to a single hospital. HD, high dose.
Discussion
Our study shows a steady increase in the incidence of E. faecalis and E. faecium blood culture isolates from 2011 to 2017, similarly to studies conducted in other countries.27,28
During the study period, data on the prevalence of antibiotic resistance of E. faecalis and E. faecium regarding ampicillin, gentamicin, and vancomycin did not differ substantially from data described by the 2017 ECDC report. 29 We observed a progressive decrease of high-level gentamicin-resistant E. faecium and E. faecalis isolates from 2011 to 2017 (74–53%, 54–39%, respectively). These data are mostly in line with ECDC reports over time, with the exception of E. faecium isolates in the period 2011–2012, in which we found a peak of resistant isolates (74% and 69%, in comparison with 54.1% and 61.8% related to ECDC reports). An explanation could be related to the lower number of participating laboratories in our study, in comparison with ECDC Surveillance Network that could have enhanced the inter-laboratory variability.
We reported a significant increasing trend of VREfm, and the percentage of resistant isolated in 2017 (21%) was higher than that reported by ECDC for the same year (14.6%). Regarding antibiotics not described in the ECDC reports, although relatively few enterococcal isolates were tested for linezolid and tigecycline, most enterococcal isolates remained susceptible to these antibiotics. As linezolid is considered a second-line therapy in case of BSIs due to VRE and a first-line therapy for BSIs due to daptomycin-resistant VRE, 30 these data are worthy of further monitoring and investigations.
Regarding other enterococcal species, we observed that intrinsically vancomycin-resistant enterococci (namely E. gallinarum, E. casseliflavus/flavescens) were the third cause of enterococcal bacteremia and consequently should not be overlooked. However, we observed that non-faecalis non-faecium enterococcal species remained susceptible to linezolid and tigecycline, while we confirmed a high prevalence of ampicillin-resistant E. raffinosus. 31 Interestingly, a minority of E. gallinarum and E. casseliflavus/flavescens isolates was reported to be susceptible to vancomycin (7.4% and 7.8%, respectively), as strains with low vancomycin minimal inhibitory concentrations (2–4 mg/L, that is below the EUCAST clinical breakpoint for vancomycin of >4 mg/L) may be erroneously identified as susceptible by automated antimicrobial susceptibility testing. 32 Resistance rates to ampicillin, gentamicin, and glycopeptides regarding other minor enterococcal species were limited.
Our study has some limitations. First, the design of our multicenter study is retrospective and data regarding susceptibility testing of linezolid and tigecycline was not available for all isolates. Moreover, being a retrospective study, we do not have data regarding the molecular characteristics of the isolates, to assess if the increase in the incidence in the cultures of VRE is related to a specific clone. Second, given the lack of a central reference laboratory, we noticed a high inter-hospital variability both in performed antimicrobial susceptibility tests (e.g., daptomycin that we were ultimately unable to reliably explore in this study) and in resistance phenotypes.
Profound differences in antibiotic susceptibility have been detected for most drugs tested depending on the geographic location. Intra-laboratory changes were also apparent within the study period. These fluctuations have been taken for granted in most reports and have received different explanations. Major shifts in the circulation of bacterial clones, unbalanced recruitment of the patients investigated (diverse underlying conditions, age) and modifications of the quantitative and qualitative antibiotic selective pressure may all have contributed to the situation observed. Moreover, the species level was presumptive in isolates other than E. faecalis and E. faecium (suboptimal identification with automated and miniaturized systems). Third, we did not collect clinical features or antibiotic consumption data, and therefore no potential correlation with antibiotic resistance could be evaluated.
Finally, we did not adjust for the number of performed blood cultures that may also have varied across centers. Notwithstanding these limitations, to our knowledge, this is the first study assessing data on resistance to linezolid and tigecycline in clinical isolates of enterococci in Italy and we believe that our data can reasonably represent a cross-section of Italian reality on enterococcal bacteremias.
In conclusion, our study shows a significant increase of E. faecalis and E. faecium blood culture isolates, with a concomitant increase of vancomycin resistance in E. faecium. Resistance to linezolid and tigecycline remained low during the study period.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.