
Abstract
The detection of carbapenemase extended-spectrum β-lactamase (ESBL)-producing Enterobacterales (EB) has become a major issue among critically ill patients, especially due to their impact on appropriate antimicrobial therapy. This study aimed at evaluating the potential contribution of molecular assays to early optimization of empirical antibiotic therapy among critically ill patients with carbapenemase- and/or CTX-M-producing EB pneumonia. The CRE and ESBL ELITe MGB® assays were evaluated directly on 197 bronchoalveolar lavage (BAL) samples obtained from 120 patients. Molecular results were then compared to routine culture-based diagnostic results, and a retrospective analysis of the therapeutic antimicrobial management was performed. Among the 197 clinical specimens, blaKPC-like and blaCTX-M-like were detected in 20 (10.2%) and 12 (6.1%) specimens belonging to 15 and 11 patients, respectively. Positive predictive value (PPV) and negative predictive value (NPV) of the CRE ELITe MGB Kit were 85% [95% confidence interval [CI]: 64.9–94.6] and 100%, respectively. PPV and NPV of the ESBL ELITe MGB Kit were 75% [95% CI: 49.4–90.2] and 100%, respectively. Retrospective analysis of the therapeutic antimicrobial management at the time of BAL collection showed that in ∼50% of patients with carbapenemase- and CTX-M-producing EB pneumonia empirical antibiotic therapy could have been optimized at least 48–72 hr earlier if positive molecular data had been used. The CRE and ESBL ELITe MGB assays might be an interesting tool for expediting optimization of empirical antibiotic therapy in critically ill patients with pneumonia, depending on local epidemiology of antibiotic resistance, patient risk stratification for EB infection, and availability of an antimicrobial stewardship team.
Introduction
Pneumonia requiring care in an Intensive Care Unit (ICU) is associated with considerable morbidity, mortality, length of stay, and high hospital costs, especially in patients with significant comorbidities.1–6 Multidrug resistant (MDR) Gram-negative bacteria are responsible for most bacterial cases of pneumonia among critically ill patients.7,8 Adequate empirical therapy should be based on local epidemiology and patient's risk stratification for MDR pathogens. However, the growing threat of antimicrobial resistance hampers the choice of empirical treatment demanding a rapid turnover of microbiological results. In this regard, the detection of carbapenemase- and extended-spectrum β-lactamase (ESBL)-producing Enterobacterales (EB) has become a major issue among ICU patients, due to their impact on infection control measures and prompt and appropriate antimicrobial therapy.
Conventional phenotypic diagnostics for respiratory samples typically takes 48–72 hr, leading to an inconvenient delay in pathogen identification and load quantification, which compromises targeted therapy and risk reduction for antibiotic resistance selection.
Molecular tests targeting carbapenemase and ESBL encoding genes have been successfully used directly from blood culture9,10 and respiratory samples11–15 but there is limited evidence about their potential impact on early optimization of empirical antimicrobial management among critically ill patients with pneumonia.
The platform ELITe InGenius® (ELITechGroup Molecular Diagnostics, Turin, Italy) is an integrated system that automatically performs nucleic acid extraction, real-time PCR, and interpretation of results in less than 3 hr. The CRE and ESBL ELITe MGB® Kits are two qualitative multiplex real-time PCR assays for the detection of the most prevalent carbapenemase and ESBL encoding genes in EB, respectively. The CRE ELITe MGB Kit can detect blaKPC-like, metallo β-lactamase (i.e., blaNDM-like, blaVIM-like, blaIMP-like), and blaOXA-48-like genes, whereas the ESBL ELITe MGB Kit can identify blaCTX-Ms genes belonging to group 1 (including CTX-M-15) and group 9 (including CTX-M-14).
This study aimed at evaluating the performance of CRE and ESBL ELITe MGB assays on bronchoalveolar lavage (BAL) of critically ill patients. This study also intends to present how molecular assays detecting antibiotic resistance genes would shorten delays to optimal therapy and impact on early optimization of empirical antibiotic therapy among critically ill patients with pneumonia.
Materials and Methods
Routine culture-based microbiological diagnostics
At the Microbiology and Virology Unit of “Azienda Ospedaliero-Universitaria Città della Salute e della Scienza di Torino” (Turin, Italy) BAL samples were subjected to Gram staining and subculture on appropriate solid medium at the time of arrival to the laboratory. Matrix assisted laser desorption ionization time-of-flight mass spectrometry analysis was used for bacterial identification, and antimicrobial susceptibility testing was carried out on overnight subcultures using MicroScan WalkAway plus System (Beckman Coulter, Brea, CA) according to the manufacturer's instructions. Antimicrobial susceptibilities were interpreted according to EUCAST breakpoints as updated in 2019. 16 Furthermore, the Total ESBL Confirm Kit (Rosco, Taastrup, Denmark) was used to identify ESBL production if cefotaxime (CTX) and/or ceftazidime (CAZ) minimal inhibitory concentrations (MICs) were >1 mg/L. MASTDISCS® combi Carba plus disc system (Mast Group Ltd, Bootle, United Kingdom) was used to characterize carbapenemase producers when meropenem (MEM) MIC was >0.125 mg/L. Detection of carbapenem resistance genes was carried out using the Xpert Carba-R assay (Cepheid, Sunnyvale, CA).
Specimen collection and study design
BAL samples included in the study were obtained from critically ill patients and consisted of samples submitted for standard of care bacterial culture, which were prospectively collected for a 6-month period.
The CRE and ESBL ELITe MGB Kits were assayed using InGenius system directly on 197 BAL samples obtained from 120 patients, starting from 200 μL of a 1:2 dilution in dithiothreitol solution (Sputasol, Oxoid Ltd, Basingstoke, United Kingdom) previously heated in a thermoblock at 90°C for 5 min. The ELITe MGB Kits' internal control, as well as positive and negative controls, was used as previously described. 17
Molecular results were then compared to routine culture-based microbiological diagnostic results to estimate the accuracy of genotypic analysis. Molecular results for the CRE and ESBL targets were interpreted as shown in Table 1. All cycles with a Ct value >35 were considered negative for detectable signal. Routine culture-based microbiological diagnostic result was considered positive when carbapenemase- and/or ESBL-producing EB was detected.
Interpretation of Molecular Results on Bronchoalveolar Lavage Samples for the Detection of Carbapenemase and ESBL Encoding Genes
All cycles with a cycle threshold (Ct) value >35 were considered negative.
ESBL, extended-spectrum β-lactamase.
Accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the CRE and ESBL ELITe MGB Kits with 95% confidence interval (95% CI) were computed using the free software MedCalc website.
Subsequently, a retrospective analysis of the therapeutic antimicrobial management of the patients with positive molecular results at the time of the first BAL collection was performed to evaluate the potential contribution of genotypic data to early optimization of empirical antibiotic therapy. Empirical therapy was deemed optimal when causative bacterial strains were susceptible in vitro to at least one prescribed drug and the antibiotics prescribed were in accordance with current evidence and recommendations regarding the treatment of carbapenemase- and/or ESBL-producing EB infections.18–22
Finally, according to the obtained results, an algorithm for the application of molecular assays detecting the main carbapenemases and ESBL encoding genes in critically ill patients with pneumonia was presented, providing a comprehensive microbiological response to clinicians in case of discordance between molecular and conventional phenotypic results.
Results
Detection of carbapenemase and CTX-M encoding genes
Table 2 shows the comparison between molecular and conventional phenotypic results.
Performance of the CRE and ESBL ELITe MGB Kits on 197 Bronchoalveolar Lavage Samples Compared with Conventional Phenotypic Results
NPV, negative predictive value; PPV, positive predictive value.
Accuracy, sensitivity, specificity, PPV, and NPV of the CRE ELITe MGB Kit were 100%, 100% [95% CI: 81.6–100], 98.3% [95% CI: 95.2–99.4], 85% [95% CI: 64.9–94.6], and 100%, respectively.
Among the 197 clinical specimens, the CRE ELITe MGB Kit detected blaKPC-like in 20 (10.2%) specimens collected from 15 patients. Seventeen (85%) blaKPC-like positive specimens had concomitant positive culture results with bacterial load >104 CFU/mL. blaKPC-like was not detected in 177 specimens showing 100% accuracy. The three presumed false positive samples were collected from patients who presented culture positive to KPC-producing Klebsiella pneumoniae in the following 7 days (blood culture = 1, tracheal aspirate = 1, bronchoaspirate = 1). Neither blaNDM-IMP-VIM-like nor blaOXA-like genes were detected by the CRE ELITe MGB Kit, and no samples yielded positive culture results.
Accuracy, sensitivity, specificity, PPV, and NPV of the ESBL ELITe MGB Kit were 100%, 100% [95% CI: 70.1–100], 98.4% [95% CI: 95.4–99.5], 75% [95% CI: 49.4–90.2], and 100%, respectively.
Among the 197 clinical specimens, blaCTX-M-like was detected in 12 (6.1%) specimens belonging to 11 patients by ESBL ELITe MGB Kit. blaCTX-M-like was found in four (2%) positive blaKPC-like positive specimens that were accounted for the blaKPC-like group. Nine (75%) blaCTX-M-like positive specimens also had concordant positive culture results with bacterial load >104 CFU/mL. blaCTX-M-like was not detected in 185 specimens, and all these samples (100%) yielded negative culture results for ESBL-producing EB. The three presumed false positive samples belonged to patients which were on empirical antibiotic therapy theoretically active against ESBL-producing EB at the time of BAL sample collection (piperacillin/tazobactam = 2; ceftolozane/tazobactam = 1).
Potential impact of molecular assays detecting the main carbapenemase and CTX-M encoding genes on early optimization of empirical antibiotic therapy of critically ill patients with pneumonia
Analysis of the empirical antibiotic therapy at the time of the first BAL collection among critically ill patients with carbapenemase- and/or CTX-M-producing EB pneumonia is reported in Table 3.
Analysis of the Empirical Antibiotic Therapy at the Time of the First Bronchoalveolar Lavage Collection Among Critically Ill Patients with Carbapenemase- and/or ESBL-Producing EB Pneumonia
Two patients with negative culture-based results were on empirical antibiotic therapy with PTZ+LVX+LZD (n = 1) and PTZ (n = 1).
Three patients with negative culture-based results were on empirical antibiotic therapy with PTZ (n = 2) and CZT (n = 1).
CRO, ceftriaxone; CST, colistin; CZA, ceftazidime/avibactam; CZT, ceftolozane/tazobactam; DAP, daptomycin; EB, Enterobacterales; ETP, ertapenem; FEP, cefepime; FOS, fosfomycin; GEN, gentamycin; LVX, levofloxacin; LZD, linezolid; MEM, meropenem; PTZ, piperacillin/tazobactam; SXT, trimethoprim–sulfamethoxazole; TGC, tigecycline; VAN, vancomycin.
Among patients with KPC-producing EB pneumonia (n = 15), 3 and 12 patients were on optimal and nonoptimal empirical antibiotic therapy, respectively, while in 2 patients the culture-based approach yielded negative results.
Among patients with CTX-M-producing EB pneumonia (n = 11), five and three patients were on optimal and nonoptimal empirical antibiotic therapy, respectively, while in three patients the culture-based approach yielded negative results.
Overall, in ∼50% of patients (13/26 or 13/21 if excluding patients with negative culture-based results) empirical antibiotic therapy could have been optimized at least 48–72 hr earlier if positive molecular data had been used.
Algorithm for the application of molecular assays detecting the main carbapenemase and CTX-M encoding genes in critically ill patients with pneumonia
The use of molecular assays detecting the main carbapenemase and CTX-M encoding genes on BAL could be implemented to early optimize empirical antibiotic therapy and infection control practices in critically ill patients with pneumonia, as shown in Fig. 1.
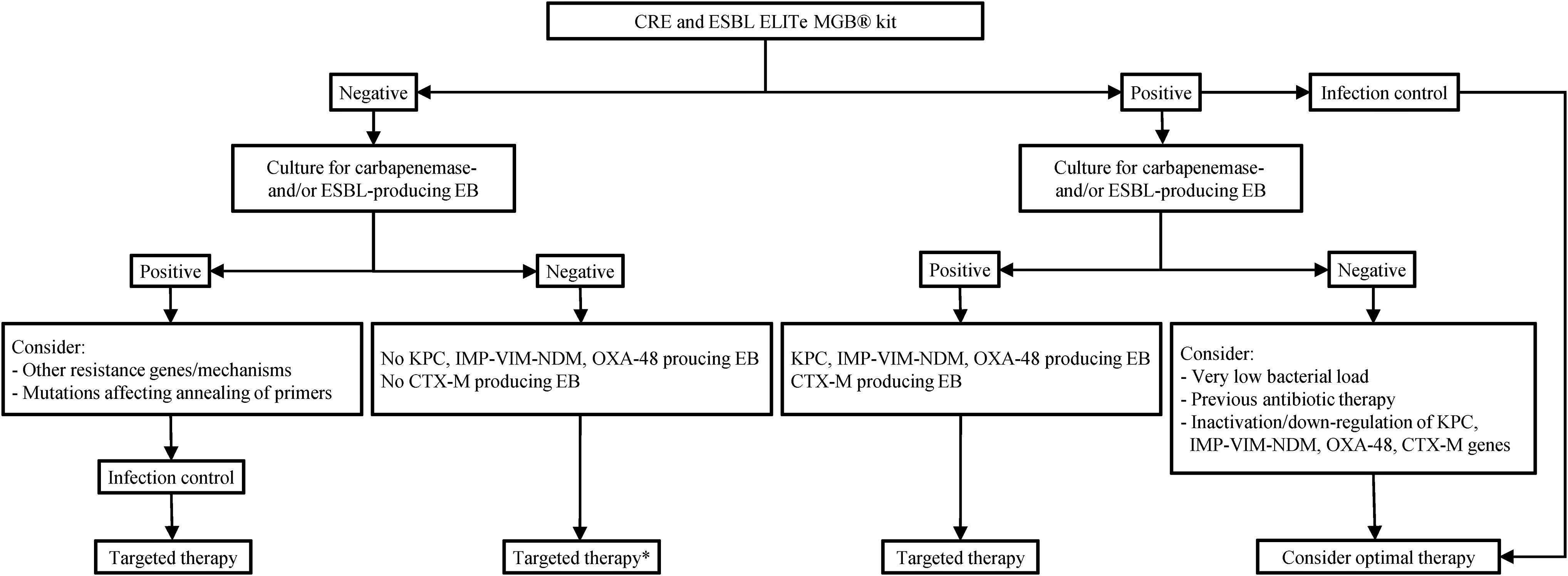
Algorithm for the application of molecular assays detecting the main carbapenemase and ESBL encoding genes directly from bronchoalveolar lavage of critically ill patients with pneumonia. *Targeted therapy toward isolated pathogens expressing resistance genes undetectable by ELITe MGB® assays or without Targeted therapy toward isolated pathogens expressing resistance genes undetectable by ELITe MGB assays or without β-lactam resistance mechanisms. EB, Enterobacterales; ESBL, extended-spectrum β-lactamase.
In case of a positive result on either CRE or ESBL ELITe MGB Kits, infection control measures should be strengthened and optimal therapy considered. If a positive molecular result is confirmed by the conventional phenotypic approach, targeted therapy would then be recommended. Conversely, if the positive molecular result is not confirmed by conventional phenotypic methods, extremely low bacterial load, previous antibiotic therapy, and inactivation or downregulation of antibiotic resistance genes should be borne in mind and optimal therapy considered.
In case of a negative result on CRE and ESBL ELITe MGB Kits together with a positive conventional phenotypic result, other resistance genes or mechanisms, as well as mutations affecting annealing of primers, should be considered. However, infection control measures should be strengthened and targeted therapy considered. Conversely, if the molecular negative result was confirmed by conventional phenotypic approach, targeted therapy toward isolated pathogens expressing resistance genes undetectable by ELITe MGB assays or without β-lactam resistance mechanisms would then be recommended.
Discussion
Current guidelines for the management of MDR Gram-negative pneumonia23,24 provide highly sensitive and insufficiently specific clinical recommendations, while empirical antibiotic therapy is to be mostly guided by the patient's hemodynamic status, leading to excessive broad spectrum empirical therapy.25,26 Although genotypic methods are not currently recommended by international guidelines for the microbiological diagnosis of pneumonia in critically ill patients and evidence regarding their impact on therapeutic management is still undefined, the role of molecular assays in clinical practice is broadly shared,27–29 especially in high MDR endemicity settings and in solid organ transplant recipients. 20
In the European scenario where carbapenemases and CTX-M variants are the major drivers of carbapenem resistance and ESBL production, 30 respectively, the use of molecular assays detecting the most widespread antibiotic resistance genes among EB directly from BAL sample seems to be reasonable and highly warranted.
In this study, the CRE and ESBL ELITe MGB Kits showed high NPV and more variable PPV.
Despite NPV suggesting a strong correlation with negative conventional culture, the antibiotic resistance genes, which were tested, are limited and do not include other less common mechanisms that could play a role in such resistance. For this reason, negative CRE and ESBL ELITe MGB assay results do not allow definite exclusion of resistance toward main beta-lactam classes. Conversely, PPV showed wide confidence intervals because the ELITe MGB Kits provided in six samples a positive molecular result despite negative conventional culture. However, among these presumed false positive samples, three were collected from patients who eventually became culture positive in the next 7 days and the other three were collected from patients who were on appropriate empirical therapy before BAL collection. All these findings may allow us to presume that confidence intervals of sensitivity and PPV were probably narrower and that molecular data could, in some cases, reveal the positive conventional culture result a few days in advance.
This study also provides an interesting view on the potential contribution of molecular results in the early optimization of empirical therapy and/or prevents dissemination at least 48 hr prior to the availability of conventional culture-based results. Indeed, in ∼50% of patients empirical antimicrobial therapy could have been optimized on the same day of bronchofibroscopy execution, contributing theoretically to reduce time of inappropriate therapy, longer antibiotic courses, use of second-line antibiotic regimens, risk of antibiotic resistance selection, and poor clinical outcomes. Given that molecular results together with knowledge of local epidemiology susceptibility patterns and antibiotic stewardship programs could be used to expedite optimization of empirical antibiotic therapy and infection control practices,11,31 the algorithm proposed in this study showed the potential for the use of CRE, ESBL ELITe MGB Kits in clinical practice when managing critically ill patients with higher risk for MDR EB pneumonia. However, conventional culture-based antimicrobial susceptibility testing continues to be required to confirm molecular results and to detect other antibiotic resistance mechanisms.
One of the limitations of this study was the lack of prospective assessment of direct implications of molecular results on antimicrobial stewardship, clinical outcomes, and cost effectiveness. Furthermore, it was not known how molecular data could have impacted on clinicians' confidence to change antibiotic therapy, especially to de-escalation since the main resistance mechanisms of Pseudomonas aeruginosa and Acinetobacter baumannii cannot be detected by the ELITe MGB Kits. Unfortunately, we did not evaluate the CRE and ESBL ELITe MGB assays on BAL samples with metallo β-lactamase- and OXA-48-like-producing EB, as they were not present during the study period.
In conclusion, the ELITe MGB assays showed high accuracy for the detection of the main carbapenemases and ESBL encoding genes from BAL of critically ill patients with pneumonia caused by EB. These assays might be an interesting tool for expediting optimization of empirical antibiotic therapy and infection control practices, depending on local epidemiology of antibiotic resistance, patient risk factors associated with MDR EB infection, and availability of an antimicrobial stewardship team with well-established fast track diagnostics. However, further studies are required to confirm these results, assessing the clinical impact of the ELITe MGB assays on antimicrobial stewardship, patient outcome, and infection control programs and determining their cost effectiveness.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. Formal ethical approval was obtained by our Center's institutional review board (Protocol No. 0029345).
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.