
Abstract
Microbial Drug Resistance
officially retracts the paper entitled, “Does Fluoroquinolones and Third-Generation Cephalosporins Restriction Reverse Extended-Spectrum β-Lactamases Klebsiella pneumoniae Resistance Rates?” by Mirjana Stanić Benić, Dora Palčevski, Romina Milanič, Nataša Skočibušić, Maja Abram, and Vera Vlahović-Palčevski (Microb Drug Resist 27:1159–1166, 2021; DOI:10.1089/mdr.2020.0301), at the authors' request.
The Editor-in-Chief of the journal received correspondence from the corresponding author, Dr. Mirjana Stanić Benić, requesting a retraction of the published article due to “shortcomings in statistical methodology. After the manuscript was published we, the authors, have received benevolent criticism from the readers who are senior and experienced experts, about the methodology that could have been more accurately handled (e.g. ‘Considering the small number of data points/months, there would have been better methods to analyze the effect of interventions, but multivariate time series analysis could not and should not have been used.’) We appreciate the constructive criticism we have received and would like to correct the methodological mistake and improve the manuscript. [sic]”
Dr. Stanić Benić indicated in her message to the Editor-in-Chief that she and her team would resubmit a new manuscript “with the same data but with revised analysis by using an adequate methodology. As our intervention was partly successful, we would still like to share our experience.”
If such a submission is received by the journal, it will undergo full and proper peer review as per the journal's standard procedures.
The Editor and Publisher of Microbial Drug Resistance are committed to preserving the integrity of the scientific literature and the community it serves.
Introduction
The emergence of antibiotic resistance is an increasing global concern and is recognized as a worldwide crisis in modern medicine. Antibiotic-resistant bacteria cause hospital outbreaks of infections and are associated with therapeutic failures and increased morbidity and mortality. 1
Klebsiella pneumoniae (KP) is one of the most concerning multidrug-resistant pathogens in human medicine. At the European Union/The European Economic Area level, more than one third (37.2%) of the KP isolates reported to European Antimicrobial Resistance Surveillance Network for 2018 were resistant to at least one of the antimicrobial groups under regular surveillance, that is, fluoroquinolones, third-generation cephalosporins (3GCs), aminoglycosides, and carbapenems. 2
KP belongs to Enterobacteriaceae that form part of gut microbiota in humans. Despite constituting normal flora, they carry a variety of virulence genes and under antibiotic selective pressure can acquire a versatile armament of antibiotic resistance genes. KP is a major pathogen causing health care-associated infections, mainly intra-abdominal, pneumonia, urinary tract infection, and primary bacteremia. 3 There are very few therapeutic options left to treat these patients, and invasive infections are associated with high mortality rates. 4
Wider interest in exploring antibiotic resistance in Enterobacteriaceae started in the 2000s with the increasing number of strains producing extended-spectrum β-lactamases (ESBL). 5 As resistance to β-lactam antimicrobials spread, the empirical treatment has shifted toward carbapenems. 6 Consequently, increased use of carbapenems led to the emergence of carbapenem resistance, owing to carbapenemase production. 3 At present, carbapenemases that are mostly plasmid-encoded in Enterobacteriaceae, are mainly found in KP and prevalently in hospital settings. They are able to hydrolyse nearly all β-lactam antibiotics, including carbapenems. 5 Alternative therapeutic options include fluoroquinolones, which carry a risk of developing a fluoroquinolone resistance in ESBL-producing Gram-negative bacilli, mostly owing to chromosomal genetic mutations in the quinolone-resistance determining regions, and colistin, with a risk of developing colistin resistance in KP as well as in other Gram-negative bacteria like multidrug-resistant Acinetobacter baumannii. 3 With the spread of resistance to multiple classes of antibiotics and lack of new antibiotics, one of the attempts to overcome the problem is the restriction of the use of known antibiotics. 7
At the Clinical Hospital Center Rijeka, Croatia, there was an increase in the rates of ertapenem-resistant phenotype among ESBL-producing KP isolates from 30% in November 2011 to 73% in May 2012. In an attempt to slow down the increasing resistance or even reverse it, the hospital Infection Control Committee together with hospital Drug and Therapeutic Committee decided to temporarily restrict the use of 3GCs and fluoroquinolones.
The objective of this study was to determine whether restriction of the use of 3GCs and fluoroquinolones may reverse the resistance rates of KP to different antimicrobial classes, and if so, to assess the long-run effects.
Methods
Setting
Clinical Hospital Centre Rijeka is a 1,069-bed tertiary care facility providing specialty services in internal medicine, surgery, gynecology and obstetrics, pediatrics, anesthesiology and intensive care, infectious diseases, oncology, neurology, psychiatry, urology, dermatology, ophthalmology, and otorhinolaryngology. It is a referral hospital for 300,000 inhabitants, including 15,000 tourists and incorporates 20,000–25,000 patient-days monthly.
Restrictive policy intervention concerned limitation of fluoroquinolones and 3GCs use during 9 months in 2012–2013. They could have been prescribed only based on consultation with a clinical pharmacologist or clinical microbiologist. Other reserve antibiotics could have been dispensed if authorized by a senior physician.
KP isolates
Nonduplicate KP strains were consecutively collected from blood culture, urine, and lower respiratory tract specimens of adult hospitalized patients during a period of 21 months (November 2011 to July 2013), 6 months before the intervention, 9 months during the intervention, and 6 months after the intervention, and monthly (12) in 2018. Bacterial identification was performed by the Vitek 2 compact (bioMérieux, France) system using GN ID (Identification Gram-negative bacteria) cards. Disk diffusion and E test methods were used to determine the susceptibility of KP and isolates were categorized as follows: susceptible, intermediate susceptible, and resistant according to EUCAST recommendations. Double-disk synergy test and combination disk test were used for phenotypic determination of ESBL production. The ESBL producer was defined as an organism showing a visible distortion or extension of the edge of the inhibition zone of cephalosporins (ceftazidime, cefotaxime, and cefepime) toward amoxicillin/clavulanate, and an increase in zone diameter of ≥5 mm in the presence of clavulanic acid than ceftazidime or cefotaxime alone. The detection of AmpC β-lactamases was carried out based on disk diffusion zones of cefoxitin <18 mm. Ertapenem disk was used to screen carbapenem resistance. All ertapenem-nonsusceptible KP isolates were sent to the Croatian national reference laboratory and were tested for five common carbapenemase genes (IMP, VIM, KPC, NDM-1, and OXA-48).
ESBL-KP isolates are presented as the ratio of all Klebsiella strains. Ertapenem-resistant ESBL-KP and fluoroquinolone-resistant ESBL-KP isolates are defined as the ratio of all ESBL-KP isolates.
Antibiotic consumption data
Information on antibiotic consumption was generated from the hospital administrative system. It was based on pharmacy records on antibiotics dispensed to wards and departments. Data on 3GCs (ATC group J01DD), fluoroquinolones (ATC group J01MA), and carbapenems (ATC group J01DH) consumption in respective period were retrieved. The consumption was expressed as the number of defined daily doses (DDDs) per 100 occupied bed-days (OBD) as a standard quantitative metric. 8 ATC classification index with DDDs 2019 was used. 9
Construction of autoregressive integrated moving average model
For the comparison of continuous variables (consumption data and resistance rates) in different periods, Student t test was used.
To determine the association of antibiotic consumption to antibiotic resistance, including a restriction of antibiotic use, autoregressive integrated moving average (ARIMA) models were constructed. The models were constructed using the strategy developed by Box and Jenkins, which includes a three-step iterative cycle of model identification, estimation, and diagnosis. 10
Antibiotic consumption rates for fluoroquinolones, 3GCs, and carbapenems expressed as DDD/100 OBD were used as independent variables (IVs). ESBL-KP isolates resistant to ertapenem and fluoroquinolones expressed as percentages of the total of ESBL-KP for a given month were used as dependent variables (DVs).
As the first step, univariate ARIMA models for IVs and DVs were constructed. In the identification phase, sequence charts were used to assess the need for differencing and transformations to achieve a stationary series. Autocorrelation (ACF) and partial autocorrelation (PACF) functions were then examined to determine the appropriate AR and MA components of the model. In the estimation phase, models with various AR and MA components were tested for significance. Competing models were compared based on significance of the parameters, normalized Bayesian information criterion (BIC), and the coefficient of determination (R 2 ). In the diagnostic phase, residual scores were examined to determine if there were still patterns in the data; however, no AR or MA components were identified in the estimation phase for any of the IVs and DVs.
In the second step, possible relationships between IVs and DVs were examined by constructing transfer function (TF) models, following the modeling strategy proposed by Haugh. 11 Cross-correlation functions (CCFs) between residuals of constructed univariate ARIMA models were computed for all six combinations of three IVs and two DVs. Based on CCFs, adequate lags to be introduced in the TF models were identified. TF models were then constructed using the Box-Jenkins strategy of iterative identification, estimation, and diagnosis. Competing models were again compared based on the significance of the parameters, BIC and R2.
The data were analyzed using the SPSS software (IBM Corp. Released in 2017. IBM SPSS Statistics for Windows, Version 25.0, IBM Corp., Armonk, NY).
Univariate ARIMA models
Sequential charts of the consumption rates of fluoroquinolones and 3GCs throughout the period of 21 months revealed a linear trend requiring differencing. An integrated component (d = 1) was introduced into the models. After differencing, the series had a stationary mean and variance. ACF and PACF functions pointed to no AR and MA components. Fluoroquinolone and 3GC consumption were modeled with ARIMA (0, 1, 0) model. Time series for consumption rates of carbapenems and resistances to ertapenem and fluoroquinolones did not require differencing or transformations to achieve stationarity. ACF and PACF functions pointed to no AR and MA components as well, resulting in ARIMA (0, 0, 0) models. Table 1 provides model parameters (constants only), significance tests, normalized BICs, and coefficients of determination.
Parameters, Parameter Significance and Diagnostics for Univariate Autoregressive Integrated Moving Average Models
nBIC, normalized Bayesian information criterion; SE, standard error.
Transfer functions
CCFs were obtained from residuals of previous univariate ARIMA models. Lags up to 3 months were examined. Larger lags would exclude too much data from the analysis because pre- and postintervention periods were 6 months long. Carbapenems consumption residuals had a significant correlation with residuals of resistance to fluoroquinolones at the lag of 1 month (parameter: −0.472, standard error: 0.224). Cross-correlations for other variables were not significant.
The construction of models for all combinations of IVs and DVs began by specifying the TF as an ARIMA (0, 0, 0) model to obtain the residuals for the construction of ACF and PACF functions, which were then analyzed for further model specification. Models were specified until residuals corresponded to white noise.
Results
Antibiotic consumption data for fluoroquinolones, 3GCs, and carbapenems
Comparing preintervention (6 months) and intervention (9 months) period, as well as preintervention and postintervention period (6 months each), consumption of 3GCs statistically significantly decreased (p < 0.001). Use of fluoroquinolones also decreased comparing preintervention and intervention period, but increase was observed in postintervention period in comparison with intervention period, although statistical significance was not reached for both fluoroquinolone analyses (Table 2). Overall, a trend of decreased antibiotic consumption was observed comparing pre- and postintervention period (44.45 DDD/100 OBD vs. 39.65 DDD/100 OBD; p = 0.324).
Average Antibiotic Consumption Data (Defined Daily Doses/100 Occupied Bed-Days) for the 6 Months of Preintervention, 9 Months During the Intervention, and 6 Months of Postintervention Period
Statistical significance for the comparison of data of preintrevention to intervention period.
Statistical significance for the comparison of data of preintrevention to postintervention period.
DDD, defined daily dose; OBD, occupied bed-days.
In 2018, consumption of 3GCs, fluoroquinolones, and carbapenems increased significantly compared with the 2011–2013 period. For 3GCs, it was 5.38 versus 3.02 DDD/100 OBD monthly (p < 0.001), for fluoroquinolones it was 7.6 versus 0.77 DDD/100 OBD monthly (p < 0.00001), and for carbapenems it was 5.72 versus 1.74 DDD/100 OBD (p < 0.001).
ESBL-KP resistant to ertapenem isolates rates
In the period of 21 months (November 2011 to July 2013), rates of ESBL-KP resistant to ertapenem ranged widely. The minimum rate was observed in the last month of postintervention period (0%), whereas the maximum rate was detected in the first month after the restriction policy was introduced (72%) (Fig. 1). Overall resistance rate (defined as the ratio of the summed resistance rates and the number of months involved) was 43.6% in the preintervention period, 42.6% during the intervention period, and 26% in the postintervention period. There was no statistical difference in the rates from both 6 months before and after the intervention (p = 0.144). Common carbapenemase genes (IMP, VIM, KPC, NDM-1, and OXA-48) were not detected in KP isolates.
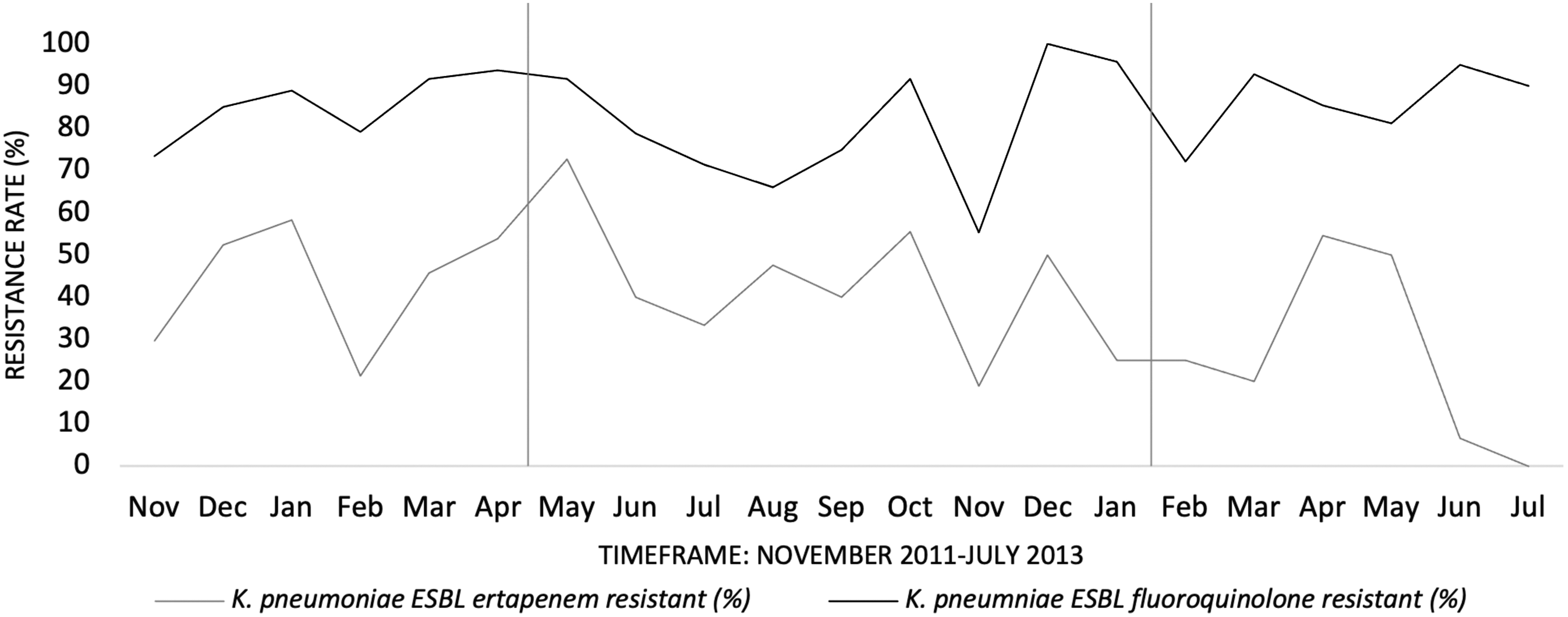
Resistance rates of ESBL KP to ertapenem and fluoroquinolones during the period of 21 months (November 2011 to July 2013; expressed as ratio of all ESBL KP isolates). *Vertical line indicates preintervention period (6 months), intervention period (9 months), and postintervention period (6 months). ESBL, extended-spectrum β-lactamases; KP, Klebsiella pneumoniae.
In 2018 resistance rates ranged from 0% to 11.11% (Fig. 2). Statistically significant decrease in resistance rate was observed in comparison of the period 2011–2013 and year 2018 (p < 0.001).

Resistance rates of ESBL KP to ertapenem and fluoroquinolones in 2018 (expressed as ratio of all ESBL KP isolates).
ESBL-KP resistant to fluoroquinolone isolates rates
Both minimum and maximum resistance rates of the ESBL-KP resistant to fluoroquinolones were detected during the intervention period, 55% and 100%, respectively (Fig. 1). Overall resistance rates in the preintervention, intervention, and postintervention period were 85.3%, 80.6%, and 86.1%, respectively. There was no statistical difference when comparing rates from both 6 months before and after the intervention (p = 0.869).
The resistance rates in 2018 were similar to observed resistance rates in the 2011–2013 period, ranging from 69% to 100% (Fig. 2).
ARIMA model
ACF and PACF functions of the base model for the prediction of the percentage of ertapenem-resistant isolates by fluoroquinolone use displayed patterns indicating a lack of AR and MA components and run models did not have better diagnostics than the base model. ARIMA (0, 0, 0) was kept as the final model. Fluoroquinolone use did not significantly predict percentage of ertapenem-resistant isolates (b = −0.206, p = 0.473).
The TF model for the prediction of the percentage of ertapenem-resistant isolates by 3GC use also remained specified as ARIMA (0, 0, 0). 3GCs use did not significantly predict percentage of ertapenem-resistant isolates (b = 0.141, p = 0.958).
The TF model for the prediction of the percentage of ertapenem-resistant isolates by carbapenem use remained specified as ARIMA (0, 0, 0). Carbapenem use did not significantly predict percentage of ertapenem-resistant isolates (b = 1.165, p = 0.910).
Residuals from the base model for the prediction of fluoroquinolone-resistant isolates by fluoroquinolone use displayed a pattern indicating an MA component. ARIMA (0, 0, 1) model was specified. Fluoroquinolone use significantly predicted the percentage of fluoroquinolone-resistant isolates, with an increase of 1 DDD of fluoroquinolone per 100 OBD corresponding to a 0.32% increase in the percentage of fluoroquinolone-resistant isolates (p = 0.008). The effect, together with the MA1 component, explained 23% of the variance in the results of the percentage of fluoroquinolone-resistant isolates.
The TF model for the prediction of the percentage of fluoroquinolone-resistant isolates by 3GCs use remained specified as ARIMA (0, 0, 0). Cephalosporin use did not significantly predict the percentage of fluoroquinolone-resistant isolates (b = 1.743, p = 0.290).
The base model for the prediction of fluoroquinolone-resistant isolates by carbapenem use had an included 1-month delay because of the significant CCF. ACF and PACF functions of the residuals indicated an AR component. AR4 proved significant, and previous AR lags were added to the model as well. ARIMA (4, 0, 0) was specified. An increase of 1 DDD of carbapenem/100 OBD 1 month earlier resulted in a 16.94% decrease in percentage of fluoroquinolone-resistant isolates (p = 0.007). The effect, together with the AR components, explained 45% of the variance in the results of the percentage of fluoroquinolone-resistant isolates. Table 3 contains model parameters, significance tests, normalized BICs, and coefficients of determination.
Parameters, Parameter Significance and Diagnostics for Transfer Functions
AR, autoregressive; MA, moving average; TF, transfer function.
Discussion
The restrictive policy intervention for 3GCs and fluoroquinolones was introduced at Clinical Hospital Centre Rijeka following the emergence of increased rates of ertapenem-resistant isolates among ESBL-KP. We found that fluoroquinolone use significantly predicted the percentage of fluoroquinolone-resistant isolates. In addition, the intervention succeeded in decreasing significantly the consumption of 3GCs and the rate of ertapenem-resistant ESBL-KP. Contrary to our expectations, the elaboration of the data by ARIMA models did not show a statistically significant association between the consumption of two restricted antibiotic classes and rates of ertapenem-resistant ESBL-KP.
The increasing trend and peak of resistant rates of KP to 3GCs, fluoroquinolones, and carbapenems in European countries were observed in 2012–2013, similar to our hospital. 12 From 2013 up to 2018, resistance rates of KP tended to stabilize, and were not significantly different compared with the previous period. It is also shown that the temporal curve of bacterial resistance rates depends on the data of antibiotic consumption and the authors concluded that stabilizing the trend of antibiotic consumption data resulted in a stabilizing trend of bacterial resistance rates. 12 We observed the same dynamics in the period of restrictive policy intervention.
In 2018, we recorded a statistically significant increase in consumption of 3GCs, fluoroquinolones, and carbapenems compared with the 2011–2013 period followed by a statistically significant decrease in resistance rates of the ertapenem-resistant KP isolates. Except for restrictive policy intervention of antibiotic use, local antibiotic guidelines published in 2011/2012 and 2015/2016, appreciably probably influenced decreasing resistance rates of ertapenem-resistant ESBL-KP. 13
Although the restriction of fluoroquinolone use resulted in their decreased consumption in the intervention period, an increased trend was shown in the period of 6 months after the intervention. In the study by Trautner et al. reduction in antibiotic use persisted after the stewardship program finished, but we did not observe the same. 14 More specifically, responsible use of ciprofloxacin seems to be a treatment challenge to the clinicians. 15 When evaluating adherence to the local antibiotic guidelines in our hospital, the highest level of noncompliance was observed when cefuroxime, ceftriaxone, and ciprofloxacin were prescribed and it is confirmed in this study. 13 Increased use of restricted antibiotics and partial success of the restrictive antibiotic intervention is described worldwide.16–18
Fluoroquinolones and carbapenems represent treatment options for ESBL-KP. Carbapenems are preferable over the fluoroquinolones. Carbapenems were reserve list antibiotics, but not involved within restrictive policy. We included data on their consumption owing to the possibility of rebound phenomena to 3GC restriction. Data for carbapenems and fluoroquinolones use showed a similar increasing trend in the pre- and postintervention period that is consistent with the report of Muller et al. who showed that a reduction in fluoroquinolone use is independently associated with the higher probability of reduction in carbapenem use. 19 In addition, an increase in carbapenems use owing to 3GC restriction could be accompanied by the increase in carbapenem resistance.20–22 Some evidence suggests that the association of carbapenem use and resistance to carbapenems is stronger where the prevalence of resistant isolates is higher.23,24 Although the rate of ertapenem-resistant ESBL-KP ranged from 26% to 43.6% in our setting, we did not find a significant association between carbapenem use and rates of ertapenem-resistant ESBL-KP in the pre- and postintervention period. Although nonsusceptibility to ertapenem is deemed a sensitive indicator for potential carbapenemase production in the Enterobacteriaceae, in this study common carbapenemase genes (IMP, VIM, KPC, NDM-1, and OXA-48) were not detected. Resistance was most probably because of the combination of porin alteration and ESBL activity.
Candevir et al. reported that restriction of 3GCs use may effectively reduce carbapenem-resistant KP. 25 We observed that a significant reduction of 3GCs use resulted in a 17.5% decrease of the rate of ertapenem-resistant KP isolate. Contrary to our results, the study by Nadrah et al. did not find a significant impact of the restriction of cephalosporins on the incidence of ESBL-KP. 7
The role of fluoroquinolone in the treatment of ESBL-producing infections remains unclear.3,26 Fluoroquinolone use, among other antibiotics, possess the unique antibiotic pressure and could have a notable impact on mortality.27–30 Our finding that fluoroquinolone-resistant ESBL-KP was significantly directly proportionally related to the use of fluoroquinolones and inversely proportionally related to the carbapenems use data highlighted the role of responsible antibiotic use. An increased carbapenem consumption concomitantly influenced decreased use of fluoroquinolones, leading to a decrease in fluoroquinolone-resistant ESBL-KP. “Squeezing the balloon phenomenon” is a well-known phenomenon within antibiotic restrictive policy. Kuziemski et al. underlined a complex relationship between the quantity of antibiotic consumption and rates of resistant bacterial isolates. 31
The limitation of our study is that we did not investigate possible rebound phenomena to other classes of antibiotics except for carbapenems. In addition, if the pre- and postintervention periods had been longer, it would have been easier to detect changes in the association of antibiotic consumption to KP resistance rates. Because of technical issues regarding the electronic data collection system, it was not possible to gather the data for a longer period.
Reports addressing the association between quantity of antibiotic use and bacterial resistance rates vary widely, as do study designs, statistical methods, specific classes of antibiotics, and resistance profile of bacteria monitored, making it difficult to appropriately compare results and conclusions. We used ARIMA models that have been shown as an optimal tool to investigate the association of antibiotic consumption data and bacterial resistance rates in real life.24,32,33
The reason why an association between data on antibiotic use and resistance rates of ESBL-KP by ARIMA models was not established could be because of the fact that our intervention was mainly based on antibiotic restriction policy. Some authors reported that antibiotic restrictive intervention alone could result in a decrease in resistance rates of ESBL-KP, but others had shown that only restrictive interventions are not sufficient to reduce bacterial-resistant strains. In addition, infection control education, better hygienic measures, and improvement of the living standard should also be involved.20,22,24,34–38
Although some of our results were contrary to our expectations, it is worthy to communicate complete results. The relationship between antibiotic use data and bacterial resistance rates is one big puzzle, and reporting a complete, not only preferred and expected results, should be encouraged aiming to get the better understanding of the dynamics of bacterial resistance to antimicrobials.
Footnotes
Acknowledgments
Partial results of this study have been presented as a poster and oral presentation at Central European Symposium on Antimicrobials and Antimicrobial REsistance (CESAR), which took place in Šibenik, Croatia from September 23 to 26, 2015.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study received no specific grant from any funding sources.