
Abstract
Staphylococcus pseudintermedius is usually a commensal bacterium of microbiota of dogs and cats that can become pathogenic in these animals. In the past two decades, an increasing number of human infections caused by this pathogen was reported; only two pediatric cases were due to methicillin-susceptible isolates. We describe the first case of methicillin-resistant S. pseudintermedius diagnosed in a 12-year-old immunocompromised girl with refractory anaplastic ependymoma, presented with life-threatening pneumonia and bacteremia. The girl had close contact with her two pet dogs. This case emphasizes that immunocompromised children should be advised on proper handling of household pets to minimize the risk of infection, which could be life threatening.
Introduction
Staphylococcus pseudintermedius is a coagulase-positive Staphylococcus species, which was first identified in animals in 1999 as Staphylococcus intermedius, to be reclassified later in 2005 as S. pseudintermedius. 1 It belongs to a group of three closely related Staphylococcal species (S. pseudintermedius, S. intermedius, and S. delphini) known as the S. intermedius group. S. pseudintermedius is commensal in dogs and mainly associated with skin and ear infections. After its identification, studies have shown that ∼90% of healthy dogs are colonized with this bacterium, mainly in the pharynx and rectum. 2
S. pseudintermedius shares several important virulence factors with S. aureus such as coagulase, protease, DNase, β-hemolysin, and exfoliative toxin.
2
Numerous antimicrobial resistance genes were identified in S. pseudintermedius, including ermB for macrolides and lincosamide resistance, S-L gyrA 251 and S-I grlA 239 for fluoroquinolone resistance, aac(6)-aph(2) and aph(3′)-III for aminoglycoside resistance, tet(M) and tet(K) for tetracycline resistance, and rpoB for rifampicin resistance.
3
In the past, S. pseudintermedius isolates were generally susceptible to penicillinase-stable beta-lactam antibiotics,
2
but, since 2006, methicillin-resistant S. pseudintermedius (MRSP) has been increasingly emerging,
4
mainly due to mecA-containing S. pseudintermedius clonal spread. Five successful MRSP clonal complexes (CC) with specific resistance traits and geographical distribution have spread globally, with CC71 and CC258 being predominant in Europe.
5
Recent studies show high prevalence of MRSP and multidrug resistance in clinical samples from pets.
6
Only a few cases of MRSP human infections were reported in the adult population (Table 1
Summary of Reports on Human Infections Due to S. pseudintermedius
F, female; M, male; MALDI-TOF, matrix-assisted laser desorption ionization time-of-flight; MRSP, methicillin-resistant S. pseudintermedius; MSSP, methicillin-susceptible S. pseudintermedius.
S. pseudintermedius is not part of the normal human flora, thus human infections are limited to individuals who have frequent contact with animals, especially dogs. Dog ownership and direct contact with contaminated lesions in dogs were found as predictors for human colonization and infection.7,8 S. pseudintermedius colonization in pet owners is higher than in the general population, and pet owners usually carry strains that are identical to their dogs isolates, suggesting zoonotic transmission.6,7 MRSP but not methicillin-susceptible S. pseudintermedius (MSSP) were isolated from nasal swabs of veterinarians suggesting that MRSP may have a particular predisposition to human colonization compared with MSSP. 9 Despite that, the origin of the organism remains unknown in most cases.
The first case of S. pseudintermedius human infection was described in 2006 by Van Hoovels et al., reporting the development of endocarditis after a cardiac device implantation in an adult patient.
10
In the past two decades, about 82 cases of S. pseudintermedius human infection were reported, but only two of them were diagnosed in children (Table 1
Case Report
A 12-year-old girl was admitted to the Department of Pediatric Hemato-Oncology at Soroka University Medical Center, Beer-Sheva, Israel, after 2 days of vomiting, cough, dyspnea, orthopnea, and somnolence (Fig. 1). Her medical background included refractory anaplastic ependymoma diagnosed at the age of 3 months, s/p ventriculoperitoneal shunt insertion, seizures, right hemiparesis, right vocal cord paresis, hypothyroidism, mild-to-moderate left ventricular failure, hyper-reactive airways disease, and recurrent eczematous rash. Her past treatment included three craniotomies, radiotherapy, radiosurgery, and chemotherapy. She suffered few recurrences and was treated with several chemotherapeutic regimens. The last relapse was diagnosed at the age of 10 years, for which treatment with vincristine, bevacizumab, temozolomide, and etoposide was initiated. Two days before admission, she completed her last chemotherapy course.
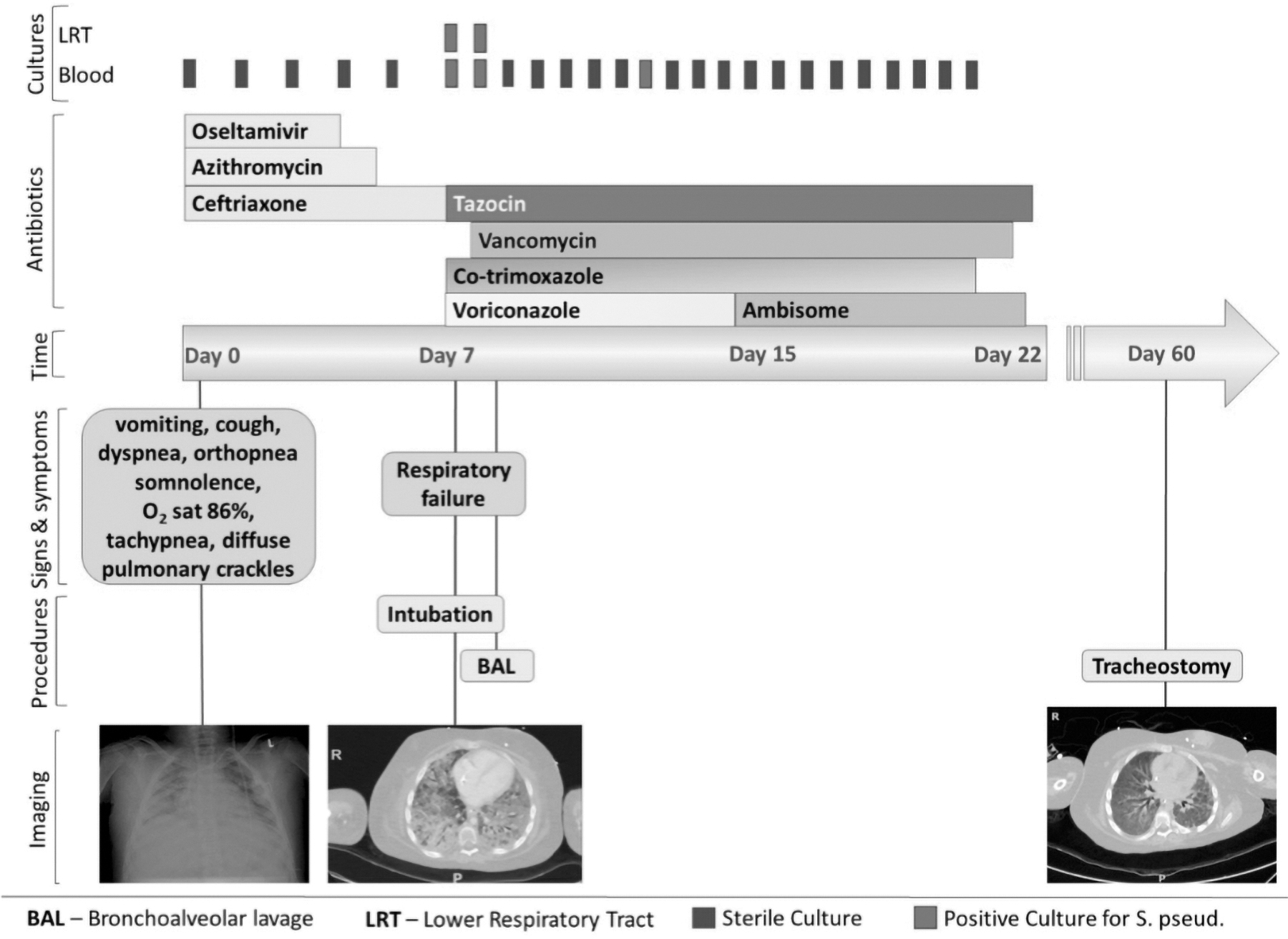
Timeline of the case report.
On admission, she was hemodynamically stable and afebrile (body temperature of 36.7°C). She had tachypnea, dyspnea, hypertension, peripheral edema, and bilateral diffuse crackles on lung auscultation. Laboratory tests revealed anemia of 8.8 g/dL, mild leukocytosis of 16.2 × 103/μL, thrombocytopenia of 91 × 103/μL, increased C-reactive protein (16.7 mg/dL, reference range <0.5), hyponatremia of 127 mEq/L, and hypochloremia of 90 mEq/L. Chest X-ray showed bilateral pulmonary infiltrates (Fig. 2). Echocardiography showed decreased but stable cardiac function with left ventricular ejection fraction of 50%. Blood cultures were drawn and treatment with ceftriaxone, azithromycin, oseltamivir, furosemide, and enalapril was initiated.

Chest X-ray on admission showing diffuse bilateral pulmonary infiltrates.
Six days later, her respiratory status deteriorated and she required noninvasive ventilation. Laboratory tests showed marked elevation of CRP (30 mg/dL) and antimicrobial treatment was changed to piperacillin/tazobactam and voriconazole. A day later, due to further respiratory deterioration, she was transferred to the Pediatric Intensive Care Unit (PICU) and invasive mechanical ventilation was initiated. Upon arrival, she had severe oxygenation problem (oxygenation index as high as 35 with PO2/FiO2 of 30) and required significantly high ventilatory pressures and oxygen, recruitment maneuvers, and inhaled nitric oxide therapy. She was supported with inotropic agents for 14 days. Treatment with trimethoprim/sulfamethoxazole was added to cover possible Pneumocystis jirovecii infection. An echocardiographic examination showed pulmonary hypertension with worsening cardiac function.
Computerized tomography scan demonstrated diffuse bilateral pulmonary infiltrates with ground-glass appearance and air bronchogram (Fig. 3). Flexible bronchoscopy showed patent airways, but the distal airways were filled with purulent sputum. Lower respiratory secretions were positive for Gram-positive cocci, identified by MALDI-TOF as S. pseudintermedius (VITEK®MS, bioMérieux, Marcy l'Etoile, France, established protocols, using VITEK GP ID Card—Reference number 21342). Blood cultures obtained on the same day were also positive for S. pseudintermedius. The antimicrobial susceptibility profiles, Vitek2 system, were confirmed by E-test strips (bioMérieux, Marcy l'Etoile, France)—Table 2.

CT scan on admission to PICU showing diffuse bilateral pulmonary infiltrates with ground glass appearance. CT, computerized tomography; PICU, Pediatric Intensive Care Unit.
Minimum Inhibitory Concentration Values for S. pseudintermedius Isolates from the Patient and the Dogs
Breakpoints based on CLSI M100 Ed30:2020. CLSI, Clinical & Laboratory Standards Institute.
Characterization of MRSP strains was later performed at the National Reference Center, Central Laboratories, Israel Ministry of Health, Jerusalem, Israel. Lysis of bacterial cells was performed by suspending 1–2 colonies, grown on nutrient agar (PD040 HyLabs), in 100 μL of lysis buffer (lysozyme 50.8 units; lysostaphin 2.7 units; trisaminomethane 0.1 M pH = 8; ethylenediaminetetraacetic acid [EDTA] 0.01 M; distilled dionized water to a final volume of 100 μL), incubation in 37°C for 30 min and then boiling for 10 min. The lysate was centrifuged 14,000 rpm × 30 sec and diluted 1:10, 1.5 μL of the diluted lysate was used as a template for real-time PCR reaction. Real-time PCR primers and TaqMan probe for mecA were obtained from the Centers for Disease Control and Prevention (CDC). Both human isolates were positive for mecA. spa type was determined by sequencing the polymorphic X region of the staphylococcal protein A gene (spa) as described previously (PMID: 15635028). The spa gene was not amplified; thus the strain was not typeable. For whole-genome sequencing (WGS), automated extraction of DNA was performed using the QIAsymphony® instrument. Fresh bacterial growth was collected from nutrient agar and lysate was prepared “off-board” according to the manufacturer's recommendations. The resulting clear supernatant was used for the DNA extraction on the QIAsymphony instrument. Nextera Flex DNA Libraries (Illumina, San Diego, CA) were sequenced on NextSeq (Illumina), with read length of 150 bp paired-end at >100 × coverage. Reads were analyzed by the BioNumerics 7.6.3 (Applied Maths, Belgium). De-novo assemblies were generated by SPAdes 3.7.1 and whole-genome multilocus sequence typing (MLST) (wgMLST) analysis was performed on the BioNumerics 8.0 (Applied Maths) using default settings. Whole genome analysis of strain SA17047 revealed 100%, 99.08%, and 99.64% identity to lukS-I gene of S. pseudintermedius (accession No. AM850056), lukS-I and lukF-I genes of S. intermedius (accession No. X79188), and mecA gene of S. aureus NCTC8325 (accession No. NG_047936), respectively. In silico spa PCR, using the BioNumerics S. aureus functional genotyping tool, was negative. The MLST profile of the bacterial isolate SA17047 was ST71 and was deposited in the pubMLST database (id 2442). To further investigate the global context of the Israeli strain, the pubMLST S. pseudintermedius database was screened for MRSP isolates. MLST profiles of 974 MRSP isolates were downloaded from pubMLST and imported to the BioNumerics software and used for phylogeny analysis. Phylogeny was deduced by calculating a minimal spanning tree based on MLST allelic profiles (Fig. 4). A notable diversity was observed among the global S. pseudintermedius population, with ST71 the predominant clone. Broth microdilution method was used to determine the antimicrobial susceptibility profile of the isolates and was performed by using Sensititre susceptibility plates (Gram-positive GPALL1F AST Plate) according to the manufacturer's instructions. Minimum inhibitory concentrations (MICs) were determined according to Clinical & Laboratory Standards Institute (CLSI) guidelines (M100 2020). The isolates were resistant to penicillin, oxacillin, ciprofloxacin, levofloxacin, moxifloxacin, clindamycin, gentamicin, and trimethoprim/sulfamethoxazole. Intermediate resistance was observed for erythromycin and chloramphenicol. Susceptibility was observed for tetracycline, vancomycin, daptomycin, linezolid, rifampin, and nitrofurantoin.

Phylogenetic minimum spanning tree based on MLST allelic profile of the bacterial isolate SA17047 (ST-71). MLST, multilocus sequence typing.
The girl had two dogs at home that used to sleep in her bed; both dogs were apparently healthy with no known skin lesions and were up to date with their vaccines. Two days after the girl was diagnosed with S. pseudintermedius infection, swabs were obtained from the ears of her dogs grew S. pseudintermedius identified by MALDI-TOF, and a zoonotic transmission of infection was suspected (Table 2). The patient's port-a-cath was removed and treatment with vancomycin was initiated. Bacterial, fungal, and mycobacterial cultures; P. jirovecii stains and PCR; universal fungal and bacterial PCRs, galactomannan, and viral multiplex PCRs were all negative. After 3 days of vancomycin treatment she had a mild clinical and radiological improvement.
One week later, both lower respiratory secretions and blood cultures were sterile (Fig. 1). Several therapeutic approaches aiming to wean her off the mechanical ventilation, including intermittent pressure support ventilation, pulse therapy of corticosteroids, nutritional support, and use of immunomodulation agents (azithromycin) had failed. This was attributed to muscle weakness and a very low pulmonary compliance. Hence, she underwent a tracheostomy followed by gradual improvement. Overall, she was hospitalized for 60 days in the PICU. The girl was transferred to an ambulatory rehabilitation ward after 3 months of hospitalization, still requiring ventilator support.
Discussion
S. pseudintermedius has been isolated with increasing frequency from human infections, whether due to a true increase in prevalence or improvement in diagnostic technologies. Human cases were reported mainly with community skin and soft tissue infections, 8 followed by bacteremia, ear and sinus infections, pneumonia, and peritonitis (Table 1). Diabetes mellitus, peripheral vascular disease, and cardiovascular diseases are the most common comorbidities. 8 Immunodeficiency was found in 17% (14/83) of reported cases.
Two cases of S. pseudintermedius infections have been reported in children, both MSSP. A 4-month-old infant with neuroblastoma who did not receive any chemotherapy was hospitalized and treated for S. pseudintermedius bacteremia, with favorable outcome. The isolate from the infant was identical (by pulse-field gel electrophoresis) to the isolate cultured from the oral mucosa of his colonized bulldog pet. 11 The second case was a 6-year-old boy with hemophilia B and dog exposure, admitted due to catheter-related bacteremia with S. pseudintermedius with favorable outcome after catheter removal. 12
We present, in this study, the first case of MRSP severe pneumonia and bacteremia in an oncology pediatric patient, caused by the globally reported ST71 lineage. In most reported cases, although dog exposure was documented as risk factor, S. pseudintermedius was not isolated from the suspected animal. In the present study, S. pseudintermedius was isolated from the ears of two pet dogs, living in close proximity with the described patient. However, our study is limited since the relatedness of canine and human isolates was not assessed by MLST or WGS. Moreover, the isolates' resistance profiles were not identical (Table 2) and the time point of the dogs' colonization and infection could not be assigned.
We assumed that the dogs were colonized with several S. pseudintermedius clones and that the close proximity between the girl and her pets prompt a transmission of bacterial strains with different drug susceptibility. Laarhoven et al. found different clonal lineages of S. pseudintermedius in members of the same household. 13 In his longitudinal study of MRSP colonization in dogs and the transmission of MRSP to humans, contact animals, and the environment, he found intermittent MRSP-positive colonization in dogs and different genotypes within one household in different time points. In addition, positive environmental samples were found while no animals or humans were MRSP positive, indicating survival of MRSP in the environment for prolonged periods of time. 13
The immunosuppressive status of the girl and many antimicrobial therapies administered probably predisposed antibiotic-resistant organism transmission and the development of invasive opportunistic lung infection, in contrast to the superficial infections usually related to this pathogen.
Pneumonia is a rare presentation of S. pseudintermedius; the first case was reported in a 73-year-old man with type II diabetes mellitus who underwent bypass surgery in 1999, 9 before the final classification of the pathogen three subgroups. No animal contact was identified. 14 The second case was a 65-year-old male with disseminated metastatic small cell bronchial carcinoma who received chemotherapy and brain radiation and died few hours after admission. The identification of S. pseudintermedius from bronchial aspiration was done by amplification and sequencing of the tuf gene; his bronchial aspiration grew also Pasteurella dagmatis, another rare zoonotic infectious pathogen. 15
In summary, S. pseudintermedius is an emerging zoonotic opportunistic pathogen in immunocompromised patients, including children. The emergence of multidrug-resistant strains emphasizes the need for timely susceptibility tests to minimize the potential use of broad-spectrum antibiotics. All immunocompromised patients should receive environmental risk assessment and prevention education regarding safe pet ownership to avoid MRSP transmission from animal patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.