
Abstract
If we were to keep macrolide consumption below a certain threshold, would this reduce the probability of macrolide resistance emerging? No study that we are aware of has addressed this question. We, therefore, assessed at a country level if there was a macrolide consumption threshold for the selection of a prevalence of macrolide resistance of over 5% in Streptococcus pneumoniae, Treponema pallidum, and Mycoplasma genitalium. In this ecological-level analysis, we found evidence for a macrolide consumption threshold of 1.3 defined daily doses per 1,000 inhabitants per day (DID) for M. genitalium, 1.8 DID for T. pallidum, and 2.3 DID for S. pneumoniae. Our results provide further motivation for macrolide stewardship campaigns that strive to reduce macrolide consumption to levels below at least 2 DID.
Background
A wide range of in vitro, clinical and epidemiological studies have established that antimicrobial consumption plays a crucial role in the emergence and spread of antimicrobial resistance (AMR) (Fig. 1).1–4 While there is broad consensus on this point, there is far less consensus as to whether or not the association between antimicrobial consumption and AMR is linear. 5 Certain authors have claimed that there is a “use it and lose it” relationship whereby AMR is viewed as the inevitable outcome of using antimicrobials.5,6 In contrast, Levy hypothesized that there were thresholds of antimicrobial consumption, below which AMR was unlikely to emerge and spread. 7 A recent longitudinal study has provided epidemiological evidence to back up the existence of such thresholds for a range of antimicrobials in different bacterial species. In this study, minimum antimicrobial consumption thresholds were identified for carbapenem resistance in Acinetobacter baumannii, cephalosporin resistance in Escherichia coli, gentamicin resistance in Pseudomonas aeruginosa, and methicillin resistance in Staphylococcus aureus. 5 This study was, however, limited to isolates from inpatients in five European countries. It would be useful to know if there were also thresholds of antimicrobial consumption in the general population. If so, these could be used as targets in antimicrobial stewardship campaigns. 8

Two mechanisms whereby antibiotic (AB) therapy can lead to the spread of antimicrobial resistance (red bacteria) in a population.
Ecological studies are justified and important in this field as the pathway between consumption and AMR operates at both individual and population levels. Lipsitch and Samore outlined four mechanisms by which antibiotic treatment could select for resistance at a population level. 3 As an example, treatment with macrolides is likely to eradicate susceptible streptococci from an individual leading to the individual both being less likely to transmit susceptible streptococci to others and being at a higher risk of colonization by resistant streptococci.3,9 Both these effects may be easier to detect at a population than an individual level (Fig. 1).3,9
The relative importance of bystander selection to the emergence of AMR varies by bacterial species according to factors such as the proportion of the time that the bacteria circulate in a population without causing symptoms. 4 All three organisms chosen for the current analysis are asymptomatic for the majority of the time they circulate in a population.4,10–12 In addition, an ecological association has been found between population-level consumption of macrolides and macrolide resistance for each of these organisms. For streptococci, for example, previous articles have found strong associations between macrolide consumption and AMR in Streptococcus pneumoniae13–15 and group A Streptococcus. 14 This association has been found to apply at national14,16 and subnational levels.13,17 Similar results have been found for Treponema pallidum and Mycoplasma genitalium.10,18 These analyses all used linear regression to assess the association between consumption and resistance and did not assess for the existence of a threshold effect. We were unable to find a study that evaluated if there was evidence of antimicrobial consumption thresholds in any of these species. In this article, we assess if the ecological evidence supports the existence of a macrolide consumption threshold for the induction of macrolide resistance in S. pneumoniae, T. pallidum, and M. genitalium.
Methods
Data
S. pneumoniae
AMR data
The S. pneumoniae susceptibility data from 2005 to 2018 were taken from the European Center for Disease Prevention and Control (ECDC) Surveillance Atlas, which reports resistance prevalence estimates from the European Antimicrobial Resistance Surveillance Network (EARS-Net)—the EU's main surveillance system for AMR in bacteria that cause serious infections. All 28 EU Member States and 2 EEA countries (Iceland and Norway) participate in EARS-Net, but one country (Greece) does not report data on S. pneumoniae. Only data from invasive (blood and cerebrospinal fluid) isolates are included in EARS-Net. This is done to limit biases that may emerge if isolates from all anatomical sites were included. Further details can be found in the EARS-Net reporting protocol. 19 The system depends on national network representatives in each participating country, reporting their locally tested susceptibility data to The European Surveillance System on an annual basis. The data for macrolide resistance report the prevalence of resistance (as a percent) to erythromycin, clarithromycin, or azithromycin. The details of the survey methodology and susceptibility testing are available at https://www.ecdc.europa.eu/en/surveillance-atlas-infectious-diseases. For each country, we calculated the median prevalence of macrolide resistance in the years 2005–2018.
Antimicrobial consumption data
Data from the European Surveillance of Antimicrobial Consumption (ESAC) were used as a measure of national general population-level antimicrobial drug consumption.20,21 ESAC provides open access to the data collected on antimicrobial use in ambulatory care and hospital care in 30 European countries.20,21 ESAC reports antimicrobial consumption as the number of defined daily doses (DDD) per 1,000 inhabitants per day (DID) following the World Health Organization guidelines.21,22 One DDD is defined as the average maintenance dose per day for a drug used in its main indication for adults.21,22 As an example, the DDD for azithromycin is 0.3 g. 22 We used ATC group J01F (macrolides, lincosamides, and streptogramins), which is how ESAC reports macrolide consumption. Data were available from 1998 to 2018.
T. pallidum
The data for the prevalence of genotypic macrolide resistance in T. pallidum were extracted from a global country-level study that used linear regression to assess the association between macrolide consumption and resistance in T. pallidum. 10 The national prevalence of genotypic macrolide resistance was based on a literature review that included all studies that reported the prevalence of genotypic macrolide resistance (A2058G or A2059G, E. coli numbering) published between 1980 and 2018. 10 Where more than one prevalence estimate was available per country, the peak prevalence of resistance was used. The macrolide consumption data, expressed in DID, (for the year before that which provided the resistance prevalence) was taken from MIDAS Quantum database of the marketing research company IQVIA (Danbury, CT). IQVIA classifies the following antimicrobials as macrolides: Erythromycin, Azithromycin, Clarithromycin, Dirithromycin, Telithromycin, Clindamycin, Fidaxomicin, Lincomycin, Troleandomycin and Dalfopristin/quinupristin. IQVIA uses national sample surveys that are performed by pharmaceutical sales distribution channels to estimate antimicrobial consumption from the volume of antibiotics sold in retail and hospital pharmacies.
M. genitalium
The data for both AMR and macrolide consumption were taken from a global study that compared macrolide consumption and resistance in M. genitalium. 18 The prevalence of genotypic resistance to macrolides (mutations at positions 2058 or 2059 in 23S ribosomal RNA [rRNA]) used in this study was the country prevalence of macrolide resistance estimated by a systematic review of the prevalence of macrolide and fluoroquinolone resistance in M. genitalium. 11 This systematic review included all studies that reported the prevalence of genotypic resistance to macrolides or fluoroquinolones published up to January 7, 2019. The macrolide consumption data used in this analysis were taken from the year before the resistance prevalence estimate. 18 The macrolide consumption data, in DID, were obtained from the same IQVIA source described above.
Timing of emergence of macrolide resistance in relation to total macrolide and azithromycin consumption
A number of studies have suggested that the widespread use of the long-acting macrolide, azithromycin has played an important role in the genesis of macrolide resistance in S. pneumoniae and T. pallidum.12,23,24 To illustrate the putative association between total macrolide/azithromycin consumption and macrolide resistance we plotted the emergence of AMR by year in T. pallidum,25,26 M. genitalium, 11 and S. pneumoniae 12 in the United States in relation to the increase in sales of azithromycin in this population (sales were used as a proxy for consumption levels) 12 and total macrolide consumption. The data for azithromycin sales were taken from an article that obtained annual sales from the manufacturer's (Pfizer) annual financial reports. 12 Sales data were available until 2005 when the azithromycin patent expired in the United States. Total macrolide consumption in DID was obtained from the IQVIA database described above. Data were available for the years 2000–2015. The resistance prevalence estimates for T. pallidum were taken from two sexually transmitted infection clinics (San Francisco and Seattle),24,25 for M. genitalium from the systematic review described above 11 and for S. pneumoniae from an article that compiled resistance prevalence estimates from a literature review of the topic. 12
Analyses
We used an unvalidated but novel and simple method to define a putative macrolide consumption threshold for AMR. The U.S. Centers for Disease Control and Prevention, the World Health Organization and others have recommended changing treatment protocols for Neisseria gonorrhoeae once the prevalence of AMR exceeds 5%.27,28 Although somewhat arbitrary, we used >5% as our threshold of high prevalence of resistance. For each bacterial species, we then defined the macrolide-5% threshold as the highest median level of macrolide consumption of countries with a median resistance prevalence ≤5% for S. pneumoniae and M. genitalium and the peak resistance prevalence ≤5% for T. pallidum.
We compared differences in macrolide consumption between groups of countries using the Wilcoxon rank sum test. The statistical analyses were performed in Stata 16.0. A p-value of <0.05 was regarded as significant.
Ethics approval
This analysis involved ecological analyses of public access data, and thus, no ethics approval was necessary.
Results
In the countries with available macrolide resistance estimates, the consumption of macrolides varied considerably. In the ESAC dataset, macrolide consumption was relatively stable between 1998 and 2018—with the notable exceptions of Bulgaria, Ireland, France, and Poland (Fig. 2). The median country macrolide consumptions varied between 0.8 DID in Sweden, and 4.9 DID in Italy (median 2.9 DID, interquartile range [IQR] 2.2–3.4). Likewise, in the global IQVIA dataset, macrolide consumption varied considerably (Fig. 3).
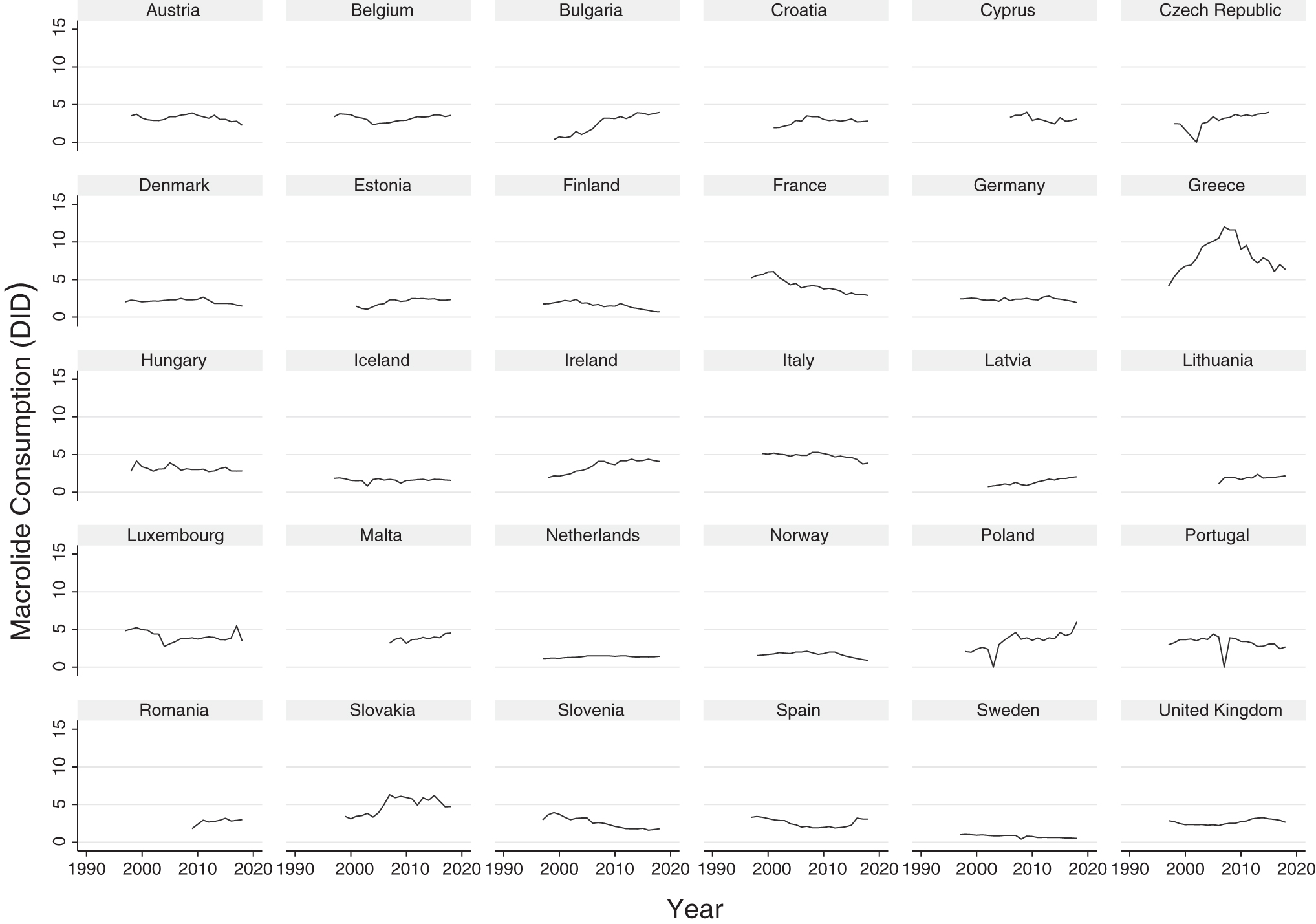
Macrolide consumption in 30 European countries, 1997–2018, according to European Surveillance of Antimicrobial Consumption. Data are in DID. DID, defined daily doses per 1,000 inhabitants per day.
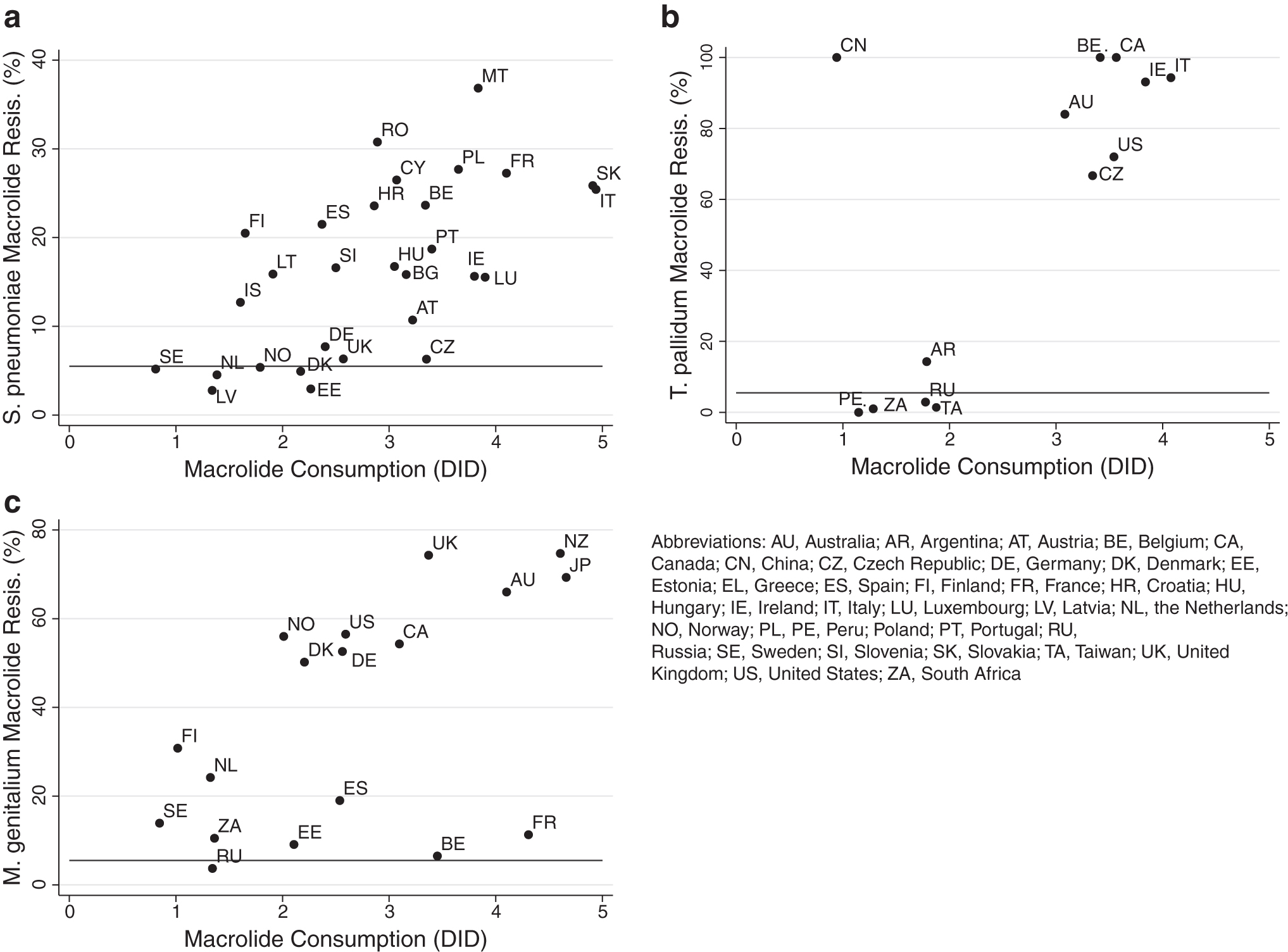
Country-level associations between macrolide consumption (in median number of DID) and antimicrobial resistance in Streptococcus pneumoniae
Large variations were also evident in the prevalence of macrolide resistance to M. genitalium, T. pallidum, and S. pneumoniae (Fig. 3).
Macrolide-5% threshold in S. pneumoniae
The prevalence of macrolide resistance was ≤5% in six countries—Sweden, the Netherlands, Latvia, Norway, Denmark, and Estonia (Fig. 3). The highest macrolide consumption in these countries was 2.3 DID in Estonia (median 1.6, IQR 1.3–2.2). Nine countries consumed 2.3 DID or less (Sweden, Latvia, the Netherlands, Iceland, Finland, Norway, Lithuania, Denmark, and Estonia). The prevalence of macrolide resistance was lower in countries that consumed less versus more macrolides than this threshold—median 5.2% (IQR 4.5–12.7%) and median 20.1% (IQR 15.6–26.2%), respectively; p < 0.001.
Macrolide-5% threshold in T. pallidum
The prevalence of macrolide resistance in T. pallidum was ≤5% in five countries (Peru, Madagascar, South Africa, Taiwan, and Russia). Of these countries, macrolide consumption was highest in Taiwan (1.8 DID). Macrolide consumption was <1.8 DID in five countries (Argentina, China, Peru, Russia, and South Africa). The prevalence of macrolide resistance was considerably lower in countries that consumed less versus those that consumed more macrolides than this threshold—median 1.2%, (IQR 0–14.3%) and median 84%, (IQR 66.7–100%), respectively; p = 0.011.
Macrolide-5% threshold in M. genitalium
Macrolide resistance was ≤5% in two countries (Kenya and Russia). Macrolide consumption data were not available for Kenya and were 1.3 DID in Russia. Macrolide consumption was lower than or equal to 1.3 DID in Finland, the Netherlands, Sweden, and Russia. The prevalence of macrolide resistance was higher in countries above this threshold (median 41%, IQR 12.6–61.3%) than Russia (3.7%), but this difference was not statistically significant (p = 0.137).
Timing of emergence of macrolide resistance in relation to azithromycin consumption
Azithromycin sales in the United States increased rapidly from close to zero dollars in 1991 to over $2 billion in 2005 (Fig. 4). This increase was followed ∼3 years later by an increase in macrolide resistance in S. pneumoniae from close to zero to above 30%. The rapid increases in macrolide resistance in T. pallidum and M. genitalium, however, followed ∼10 and 20 years after the increase in azithromycin consumption. Total macrolide consumption was high in 2000 (4.4 DID) and, while it decreased over time (2.6 DID in 2015), it remained high compared with consumption in countries such as Sweden (0.6 DID in 2015).

Temporal relationship between macrolide consumption and resistance in the United States. The emergence of macrolide resistance in Streptococcus pneumoniae in the United States followed a few years after the steep increase in azithromycin sales (U.S. $ × 108). The emergence and spread of macrolide resistance in Treponema pallidum (S, Seattle; SF, San Francisco) and Mycoplasma genitalium in the United States followed one to two decades later. Total macrolide consumption (in DID) declined slightly after 2000 but remained high compared with other countries.
Discussion
The application of our macrolide-5% methodology produced evidence of a macrolide consumption threshold of 1.3 DID for M. genitalium, 1.8 DID for T. pallidum, and 2.3 DID for S. pneumoniae.
There are a number of caveats to this conclusion, not the least of which is that we have only investigated the impact of a single variable on the genesis of AMR. The emergence and spread of AMR is dependent on multiple factors acting at different levels.5,6,29,30 These factors include homologous and heterologous class antimicrobial consumption (individual and population level), vaccination, travel, and sanitation.5,6,10,29–31 Not controlling for differences in vaccination coverage against S. pneumoniae is a particularly important omission, since this has been shown to have a significant impact on not only the incidence of invasive pneumococcal infections but also the prevalence of AMR. 31 The relative contributions of specific risk factors (such as population-level macrolide consumption) is also likely to vary between bacterial species according to factors such as the mechanisms whereby they acquire macrolide resistance as well as their susceptibility to bystander selection.4,31,32 This is evident if we consider the differences in the timing of the emergence of macrolide resistance in the three organisms in the United States. If the effect of population-level macrolide consumption on AMR was uniform, then we would expect macrolide resistance to emerge concurrently. A number of factors may play a role in explaining differences in the timing of resistance emerging. The prevalence of S. pneumoniae is typically higher compared with T. pallidum and M. genitalium, which may have placed it under a greater selection pressure from population-level consumption of macrolides. 4 The incidence of T. pallidum in the United States was low in the 1980s and early 1990s and only began to increase in the late 1990s, which may have meant that T. pallidum would only have been placed under a selection pressure from macrolides consumed for other purposes in the late 1990s. 33 The data from the Seattle cohort support this conclusion. Macrolides were not used to treat syphilis in this center, but a high proportion of clients (27%) had received macrolides for other indications in the 12 months before their syphilis diagnosis and self-reported macrolide use was associated with macrolide resistance in T. pallidum. 24 The delayed increase in macrolide resistance in M. genitalium may be explained by changes in treatment guidelines for STIs such as the use of azithromycin in combination with ceftriaxone as first-line treatment for N. gonorrhoeae in 2010. 28 A complementary explanation is that increases in screening and treatment of STIs that can be treated with azithromycin such as chlamydia and M. genitalium played a role.34,35
A number of other factors may explain the differences in the association between macrolide consumption and resistance in the three species. Differences in the fitness costs of resistance-associated mutations may be important. Variations in the biological pathways to macrolide resistance between the three species also likely play an important role. S. pneumoniae can take up resistance-conferring sections of DNA (such as erm-type methylases and mef-type efflux pumps) through transformation and conjugation.31,36 This process has been shown to have played an important role in its acquisition of resistance to macrolides. 36 M. genitalium and T. pallidum do not have this ability and the acquisition of resistance typically results from chromosomal mutations in the gene coding for the 23s RNA.10,11,24
There are also a number of countries with low reported consumption of macrolides but a high prevalence of macrolide resistance. The high prevalence of macrolide resistance in T. pallidum in China is an example (Fig. 3). These examples could be explained by high macrolide consumption in local populations with high prevalence of circulating T. pallidum (such as core groups) or the acquisition of resistant strains through travel from high-consumption countries. 10 The very high prevalence of macrolide resistance in other bacterial species, as well as T. pallidum in China could also be explained by a false low estimate of macrolide consumption in this population.10,32 It is possible that countries with ≤5% macrolide resistance in these bacterial species will still cross this resistance threshold. Evidence along these lines is available for the two countries (France and Belgium) with low macrolide resistance in M. genitalium (6.5% and 11.3%, respectively) but high macrolide consumption (Fig. 3). The resistance prevalence estimates from both countries were derived from relatively old studies used in the systematic review. 11 More recent studies have found a much higher prevalence of macrolide resistance in both countries (74% and 58%, respectively).37,38 These limitations mean that the results should be viewed with caution and require further validation. The way that travel can disseminate AMR may also mean that for certain bacterial species, a threshold may only be effective if globally applied. 39 We also used antimicrobial consumption data from two main sources—ESAC (total ambulatory and hospital consumption) when the AMR prevalence data were limited to European countries, and IQVIA (total hospital and retail consumption) when the AMR data were global. Other studies have, however, found that the IQVIA and ESAC antimicrobial consumption estimates correlate very closely with one another.30,40 For the longitudinal study in the United States, we also used both total macrolide consumption in retail and hospital pharmacies (from IQVIA) and sales of azithromycin (from manufacturer sales reports). These datasets use somewhat different methodologies to assess antimicrobial consumption, which means it would be problematic to make comparisons across datasets. We have, therefore, refrained from doing this in our analyses.
Our illustration of the association in the timing of the increase in azithromycin consumption and macrolide resistance in the United States is too crude for us to be able to make confident claims that any association is causal. More detailed analyses correlating local antimicrobial consumption data with changes in AMR would be required to assess causality. Other studies that have conducted such analyses have typically found positive associations.1,2,41
Despite these limitations, the study may provide guidance to health planners. For example, there is considerable debate in the literature as to the net benefits and risks of screening men who have sex with men in preexposure prophylaxis (PrEP) cohorts for gonorrhoea and chlamydia,34,35,42,43 PrEP guidelines recommend up to three-monthly screening, 42 but this has been shown to result in the consumption of ∼12.1 DID of macrolides. 35 In the absence of a rough consumption resistance threshold, it is difficult for planners to know how to interpret this 12.1 DID figure. If we use the macrolide-5% thresholds outlined in this study, then a consumption of 12.1 DID macrolides could be seen as being between 5- and 9-fold higher than the resistance thresholds for S. pneumoniae, M. genitalium, and T. pallidum that were found in this study. In the absence of any evidence from randomized controlled trials showing any benefit from screening, 42 planners may use this information to reevaluate the need/frequency of chlamydia/gonorrhoea screening in this population. They could also use this information to justify cutting back screening to the PrEP clients. One option would be to visualize the macrolide consumption as a “macrolide consumption footprint,” which could be compared with the threshold footprint. 8
While our analysis has not evaluated the extent to which macrolide resistance is reversible, longitudinal studies in Finland have found that a decline in macrolide consumption was followed by a significant decline in the frequency of erythromycin resistance in group A streptococcal isolates (17 to 9%). 2 Likewise, studies in Scotland have found that reductions in macrolide consumption were temporally associated with declines in the incidence of Clostridium difficile 44 and methicillin-resistant S. aureus infections. 45 Taken in conjunction with this evidence, our study provides further motivation for macrolide/antimicrobial stewardship campaigns that strive to reduce macrolide consumption to levels at least below 2 DID, but if the burden of infection allows, preferably to under 1 DID as achieved in countries such as Sweden.
Data Availability
The data we used are publicly available from the articles we refer to and the ECDC data are available from: https://atlas.ecdc.europa.eu
Footnotes
Author Contributions
C.K. conceptualized the study. C.K. was responsible for the acquisition, analysis, and interpretation of data. C.K., S.S.M.-B., and C.V.D. contributed to the first draft and read and approved the final draft.
Acknowledgment
The authors would like to thank the ECDC for the data provided on their Surveillance Atlas of Infectious Diseases.
Disclosure Statement
No competing financial interests exist.
Funding Information
No specific funding was received for this work.