
Abstract
Bacteria that cause life-threatening illnesses in humans are also capable of contaminating hospital surfaces, thus pose as a potential source of infection. This study aimed to investigate the prevalence, genetic diversity, virulence, and antibiotic resistance profile of Klebsiella pneumoniae in South Africa. In a nonoutbreak setting involving four public hospitals, 777 samples were collected in three different wards from 11 different sites. Phenotypic and genotypic methods were used for isolation and identification. The Kirby-Bauer disk-diffusion method was used to examine antibiotic resistance followed by the combination disk method to characterize extended-spectrum β-lactamases (ESBLs). Antibiotic resistance and virulence genes were screened using PCR and clonality was investigated using enterobacterial repetitive intergenic consensus (ERIC)-PCR. Seventy-five (10%) K. pneumoniae isolates were recovered. These isolates were obtained from all four hospitals and all three wards involved. However, only six frequently touched surfaces were contaminated. Thirty (40%) isolates were characterized as ESBLs showing high resistance to antibiotics and mostly harboring the blaCTX-M group one gene. Virulence genes were highly prevalent among all the isolates. ERIC-PCR showed that the isolates recovered from different sites within the same hospital were genetically similar. The study highlighted that K. pneumoniae can contaminate various surfaces and this persistence allows for the dissemination of bacteria within the hospital environment. The information from this study can assist hospitals to evaluate and improve current infection prevention and control interventions in place.
Introduction
Hospital-acquired infections (HAIs) are infections that occur in a patient while receiving medical care at a health care facility. However, HAIs are not initially present when the patient is first admitted; thus, symptoms only appear 48 hr or more after admission, or within 30 days of being discharged.1,2 HAIs are of global concern, hence, in the United States of America and Europe, prevalence rates are at 4.5% and 7.1%, respectively. 3 Due to limited resources, the true burden is unestablished in South Africa; however, there are anecdotal reports suggesting that HAIs are more prevalent in public health care facilities in comparison to private health care facilities. 4 Nonetheless, HAIs are associated with increased morbidity and mortality. 5 Furthermore, due to the prolonged hospital stay and need for additional treatment and diagnostic tests, HAIs increase health care costs. 6 A large proportion of HAIs are caused by bacteria. 2 Notably, Klebsiella pneumoniae is one of the six bacterial species that commonly cause HAIs. 7
Many factors influence a patient's risk of acquiring an infection. 6 Patients who suffer from other underlying conditions such as diabetes and those who have recently undergone medical procedures such as surgery are more vulnerable to infections. 6 Studies have also indicated that a contaminated hospital environment can play a role in transmitting bacteria since medical equipment such as blood pressure (BP) cuffs and housekeeping surfaces such as bedrails can harbor bacteria. 8 Research has demonstrated that the survival period of Klebsiella species on dry surfaces is usually between 2 hr and more than 30 months. This persistence is influenced by humidity, temperature, inoculum size, surface, and strain type. 8
Once the hands of hospital care workers encounter contaminated surfaces, they can transmit bacteria to patients during patient care if hand hygiene protocols are not strictly adhered to. Thus, contaminated hands either from the environment or from direct contact with infected or colonized patients cause 30–40% of the HAIs that occur.8,9 Infection prevention and control (IPC) measures implemented in health care facilities aim to reduce the chances of developing a HAI. 10 Practicing good hand hygiene and effectively cleaning surfaces are critical measures that can decrease the bacterial load, thus reducing any chances of bacterial transmission.8,9,11
The Klebsiella genus consists of gram-negative species that fall under the Enterobacteriaceae family. 12 K. pneumoniae can cause various infections such as pneumonia, urinary tract infections, and bloodstream infections. 13 These infections are more challenging to treat when antibiotic-resistant bacteria are involved. 14 K. pneumoniae can acquire antibiotic resistance genes encoding extended-spectrum β-lactamases (ESBLs), which confer resistance to important β-lactam antibiotics such as third-generation cephalosporins and monobactams.14,15 The three main β-lactamase enzyme families are CTX-M, SHV, and TEM, encoded by the blaCTX-M, blaSHV, and blaTEM genes, respectively. 16 K. pneumoniae also has four well-established virulence factors. These include the capsule, lipopolysaccharide, siderophores, and pili. 13
In South Africa, less than 20% of individuals rely on the well-resourced private sector to provide health care; thus, a vast majority relies on the underresourced public sectors. 17 The public health care system consists of four different levels that cater to various services. District hospitals are level one, and they provide general services to patients. When necessary, a patient can be referred to a regional (level two), tertiary (level three), or central (level four) hospital for specialist and subspecialist services. 18 In South Africa, there is a paucity of data that investigate the bacterial contamination of surfaces and equipment within the hospital environment. Given this information, the aims of this study were twofold. First, to examine the prevalence of K. pneumoniae on inanimate surfaces in South African public hospitals, and second, to determine the genetic diversity, antibiotic resistance, and virulence profiles of the collected isolates.
Materials and Methods
Ethical considerations
Ethical clearance to execute this study was granted by the Biomedical Research Ethics Committee at the University of KwaZulu-Natal (Ref. No.: BE 606/16). The study was registered on the Health Research and Knowledge Management (Ref. No.: KZ2017RP24 630) database as required by the Department of Health, South Africa. Gatekeepers approval was granted by both district and hospital management.
Sample sites
Four public hospitals situated in KwaZulu-Natal, South Africa, participated in this study. For confidentiality purposes, the different hospitals are denoted as A, B, C, and D. Furthermore, the information pertaining to each hospital detailed below was obtained from two National Health Act documents, which outlines the regulation of hospital categories 19 and the National Health insurance policy. 20 Hospital A and hospital B are large, with bed sizes ranging between 800–850 and 900–950, respectively. Hospital A is classified as a central hospital containing highly complex equipment. As a result, it can provide subspecialist and superspecialist services such as advanced trauma care and organ transplants. Hospital B is a tertiary hospital offering sophisticated diagnostic and treatment services. Hospital C and hospital D are smaller, with bed sizes ranging between 500–550 and 550–600, respectively. Hospital C is a regional hospital and it provides services that can be offered by general specialists in psychiatry, internal medicine, obstetrics and gynecology, orthopedic, general surgery, radiology, and pathology. Hospital D is a district hospital providing general services such as surgical interventions and emergency services.
Sample collection
In a nonoutbreak setting, a total of 777 samples were collected over a period of 3 months (September to November 2017). Each hospital was sampled before noon once a month on one specific day of the week. Three wards per hospital were selected for sampling, namely the intensive care unit (ICU), general, and pediatrics. A total of 11 predetermined frequently touched sampling sites were included in the study, namely the patient file, sink, mop, occupied bed (the medical history of the patient occupying the bed was unknown), unoccupied bed (no patient had been assigned to that bed before sampling therefore it was vacant), BP monitor, nurses' table, drip stand, telephone, ventilator, and the linen room door handle. Amies Agar gel transport swabs (ThermoFisher Scientific, Waltham, USA) were used to sample ∼10 cm of the area of interest. The swabs were placed back into the transport media and transported in cooler containers filled with icepacks to the laboratory and processed within 4 hr after collection. The swabs collected were immersed in 15 mL of tryptic soy broth (Oxoid, Basingstoke, United Kingdom) and incubated overnight. All incubations described in this study occurred at 35 ± 2°C for 24 hr.
Isolation and preliminary identification
Subsequent to incubation, 30 μL of the sample was spread plated onto HiCrome Klebsiella selective agar base supplemented with Klebsiella selective supplement (both from HiMedia Laboratories, Mumbai, India). After overnight incubation, the presumptive purple mucoid colonies formed from each plate were subcultured onto MacConkey Agar (Oxoid). Following incubation, the pink mucoid lactose fermenting presumptive colonies formed were subcultured onto nutrient agar (Oxoid) and incubated further. The preliminary bacterial screening was performed using several biochemical tests, namely catalase (Catalase reagent; Clinical Sciences Diagnostic, Johannesburg, South Africa), oxidase (Oxidase strips; Oxoid), motility (Edwards and Ewing Motility Medium, HiMedia Laboratories), and triple sugar iron agar (Oxoid) test. Further bacterial identification was conducted using Analytical Profile Index (API) 20E (bioMérieux, Marcy-l'Étoile, France). The presumptive K. pneumoniae isolates were subsequently stored at −80°C in tryptic soy broth (Oxoid) containing 10% glycerol. K. pneumoniae ATCC BAA-1705 was used for quality control purposes.
DNA extraction and molecular confirmation
The genomic DNA was extracted using the conventional boiling method as previously described. 21 The DNA concentration and purity were assessed using the Nanodrop ND-1000 Spectrophotometer (ThermoFisher Scientific) and subsequently stored at −20° C for further downstream applications. Using the extracted genomic DNA, the isolates were subjected to conventional PCR for the amplification of the khe gene (encoding hemolysin) used to detect K. pneumoniae.22,23 The PCR was carried out using a T100™ Thermal Cycler (Bio-Rad, Hercules, USA) with the conditions specified in ***Table 1. The total reaction volume was 25 μL and it consisted of 12.5 μL DreamTaq PCR master mix (2 × ) (ThermoFisher Scientific), 5.5 μL nuclease-free water, 5 μL template DNA, and 1 μL of each primer (forward and reverse). All primers used in this study were purchased from Inqaba Biotechnical Industries (Pty) Ltd., Pretoria, South Africa. All stock primers (100 μM) were diluted to a 10 μM working stock. The resulting PCR products were loaded into 1.5% (w/v) agarose gel stained with ethidium bromide and subjected to gel electrophoresis at 60 V for 90 min using 0.5 × tris-borate-EDTA buffer (ThermoFisher Scientific). A 100 bp DNA ladder (New England Biolabs, Ipswich, USA) was used as a molecular weight marker. The results were visualized using the ChemiDoc imaging system (Bio-Rad). K. pneumoniae ATCC BAA-1705 served as a positive control. All the PCRs conducted in this study included a negative control using nuclease-free water instead of template DNA.
The Expected Amplification Size, Primer Sequences, and PCR Conditions for the Identification, Virulence, and Antibiotic Resistance Genes
Y = T or C; R = A or G; M = A or C; H = A or C or T.
Antibiotic susceptibility testing
The PCR confirmed that K. pneumoniae isolates were subjected to antibiotic susceptibility testing using Kirby-Bauer disk diffusion on Mueller Hinton Agar (Oxoid) according to the Clinical Laboratory Standards Institute guidelines. 24 A total of 12 antibiotics belonging to seven different classes were screened. These include antibiotics from the β-lactam class: ampicillin (AMP, 10 μg), cefazolin (KZ, 30 μg), cefoxitin (FOX, 30 μg), ceftriaxone (CRO, 30 μg), meropenem (MEM, 10 μg), and amoxicillin-clavulanate (AMC, 20/10 μg); the aminoglycosides class: gentamicin (CN, 10 μg); the fluoroquinolone class: ciprofloxacin (CIP, 5 μg); the tetracycline class: tetracycline (TE, 30 μg); the folate pathway inhibitors class: trimethoprim-sulfamethoxazole (SXT, 1.25/23.75 μg); the phenicols class: chloramphenicol (C, 30 μg); and finally, the nitrofurans class: nitrofurantoin (F, 300 μg) (Oxoid). Escherichia coli ATCC 25922 was used for quality control purposes. The results were interpreted as per Clinical Laboratory Standards Institute (CLSI) guidelines. 24 Isolates were considered multidrug-resistant (MDR) when they showed resistance to at least one antibiotic in three or more different antibiotic classes. 25
Phenotypic detection of ESBL producers
The isolates resistant to ceftriaxone 24 were subjected to the ESBL test as per CLSI guidelines. 24 The combination disc method was performed on Mueller-Hinton Agar (Oxoid) using discs (D67C MAST Discs, Mast Group, Bootle, United Kingdom) of ceftazidime (CAZ, 30 μg) and cefotaxime (CTX, 30 μg) alone and in combination with clavulanate (10 μg). Results were interpreted according to the CLSI guidelines. 24 K. pneumoniae ATCC 700603 and E. coli ATCC 25922 were used as a positive and negative control, respectively.
Identification of virulence and antibiotic resistance genes
PCR was used to detect β-lactamase (blaTEM, blaSHV, blaCTX-M group 1), aminoglycoside [aac(3′)-II, aac(6′)-Ib], and fluoroquinolone (qnrB)-associated resistance genes. Virulence genes encoding type 3 pili (mrkD), siderophore (entB), and lipopolysaccharide (wabG) were also screened using PCR. All the PCR conditions used are outlined in Table 1. Singleplex (entB, blaTEM, blaSHV) reactions were conducted in the volumes previously described above. All the multiplex reactions were made to a total volume of 25 μL that comprised 12.5 μL DreamTaq PCR Master Mix (2 × ) (ThermoFisher Scientific) and 5 μL of DNA. The primer volumes differed in each reaction and they were the following, respectively: mrkD and wabG, 0.5 and 1 μL; blaCTX-M group 1 and aac(3′)-II, 1.5 and 1 μL; and qnrB and aac(6′)-Ib, 1.5 and 0.5 μL. Nuclease-free water was added in different volumes to the different reactions to make up the total volume. For quality control purposes the following positive controls were used: K. pneumoniae ATCC BAA-1705 for the virulence genes, K. pneumoniae strain 3_S2 (accession number: LJDW00000000) for qnrB and aac(6′)-Ib, and K. pneumoniae strain 15_S8 (accession number: LJEC00000000) was used for all the remaining antibiotic resistance genes. The resulting PCR products were analyzed using the conditions specified previously.
Investigating genetic diversity using enterobacterial repetitive intergenic consensus-PCR
Representative isolates were subjected to enterobacterial repetitive intergenic consensus (ERIC)-PCR to assess clonality. Using an overnight pure culture, 48 isolates were subjected to genomic DNA extraction using the Quick DNA Fungal/Bacterial Miniprep kit (Zymo Research, Irvine, USA) according to the manufacturer's instructions. The extracted genomic DNA was quantified and assessed for purity using the Nanodrop ND-1000 Spectrophotometer (ThermoFisher Scientific). The extracted DNA was utilized to conduct ERIC-PCR using a T100 Thermal Cycler (Bio-Rad). The following PCR conditions were applied: 2 min of initial denaturation at 95°C, 34 cycles of 30 sec of denaturation at 90°C, 1 min of annealing at 52°C, 8 min of extension at 65°C, and a final elongation of 16 min at 65°C. The total volume was 25 μL and it consisted of 12.5 μL of DreamTaq PCR Master Mix (2 × ) (ThermoFisher Scientific), 7.5 μL of nuclease-free water, 3 μL of genomic DNA, and 1 μL of each ERIC 1 and ERIC 2 primer. 30 Only, 7 μL of the PCR products were loaded into a 1% (w/v) agarose gel and subjected to gel electrophoresis at 75 V for 180 min using 1 × tris-acetate-EDTA buffer (ThermoFisher Scientific). A 1kb DNA ladder (New England Biolabs) was used as a molecular weight marker. Thereafter, the gel was stained in ethidium bromide for 30 min and visualized using the ChemiDoc™ imaging system (Bio-Rad). K. pneumoniae ATCC BAA-1705 was used for quality control purposes. The resulting banding patterns were analyzed using BioNumerics version 6.6.11 (Applied Maths NV, Sint-Martens-Latem, Belgium). The similarity of the banding patterns was assessed using the Dice coefficient, and the dendrogram was generated using the unweighted pair group method with arithmetic averages, using 1% tolerance and 0.5% optimization. The isolates were grouped into clusters based on a similarity of ≥60%.
Statistical analysis
The data generated were analyzed using the IBM Statistical Package for Social Sciences (SPSS) version 25 (IBM Corporation, New York, USA). A chi-square test of homogeneity was used to investigate whether the prevalence differed (non-ESBL and ESBL) between the different hospitals and between the various wards. Significant differences were further examined by conducting multiple pairwise comparisons via the implementation of a post hoc analysis using the Z-test of two proportions with a Bonferroni correction. Chi-square test for association and Fischer's exact test investigated the association between the different antibiotic resistance genes and virulence genes. All results were considered significant when p < 0.05.
Results
Prevalence of K. pneumoniae
From the 777 samples collected, a total of 75 (10%) K. pneumoniae isolates were obtained over a period of 3 months. The total number of K. pneumoniae isolates recovered was equally high in tertiary hospital B and district hospital D. The total occurrence of K. pneumoniae was lowest in central hospital A (Fig. 1A). The total sum of K. pneumoniae isolates detected was highest in the pediatric ward (Fig. 1B). From the 11 sites included in this study, K. pneumoniae was only recovered from six sites and the highest total contamination was observed from the occupied bed followed by the sink, mop, unoccupied bed, patient file, and BP monitor (Fig. 1C). Zero (0%) K. pneumoniae isolates were recovered from the nurse's table, door handle, drip stand, telephone, and ventilator.
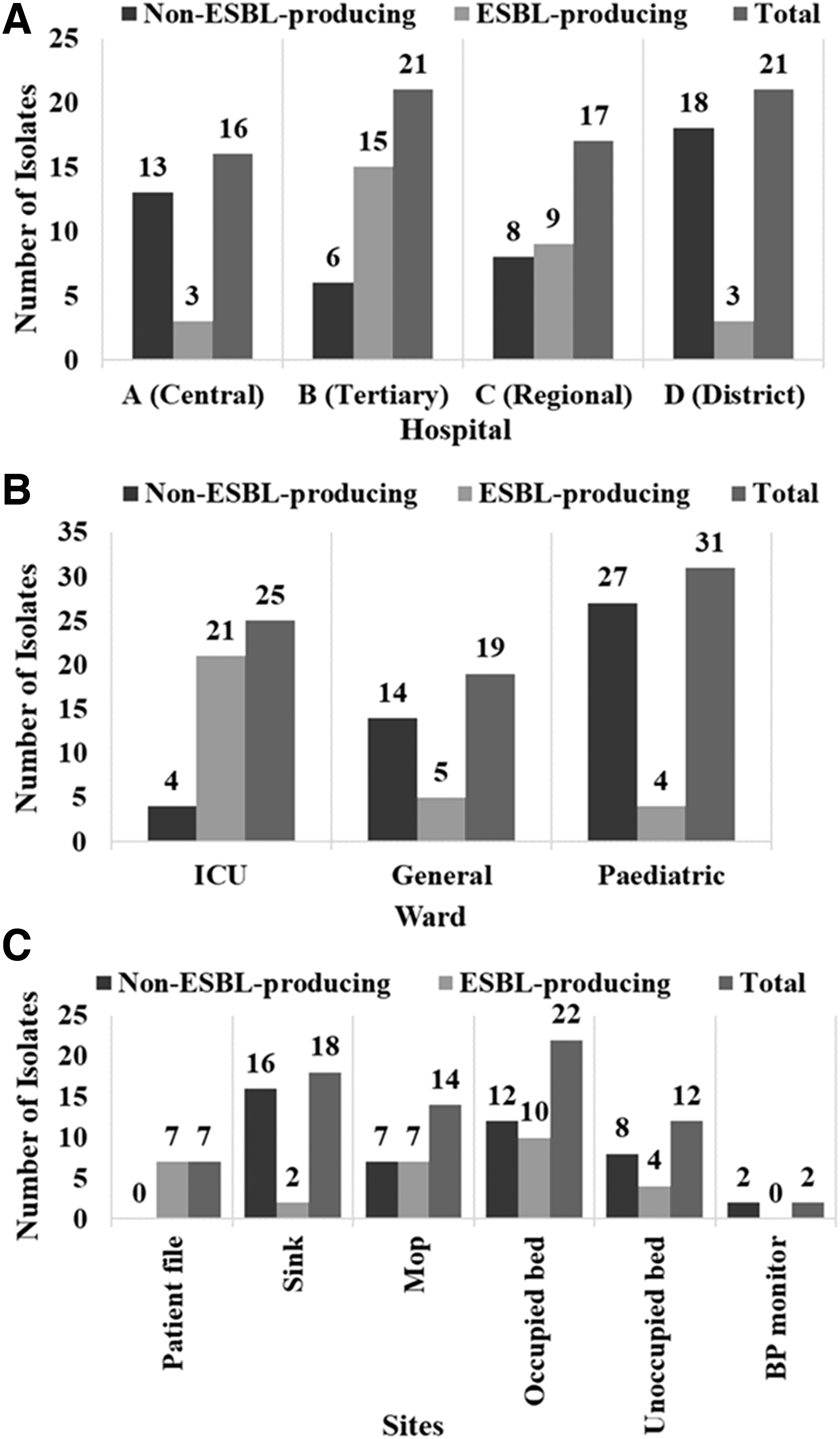
The overall proportion of non-ESBL and ESBL-producing Klebsiella pneumoniae isolates recovered across the different
Only 30 (40%) of the 75 K. pneumoniae were phenotypically identified as ESBL producers. The proportion of ESBLs recovered from tertiary hospital B was significantly (p < 0.05) higher compared to central hospital A and district hospital D. Although more ESBL isolates were detected in tertiary hospital B compared to regional hospital C, this difference was not significant (p ≥ 0.05) (Fig. 1A). The number of ESBL isolates obtained from the ICU was significantly (p < 0.05) higher compared to the general and pediatric ward (Fig. 1B).
Antibiotic susceptibility testing
The ESBLs showed higher resistance to the antibiotics screened compared to the non-ESBLs (Table 2). A total of 29 ESBL isolates were classified as MDR.
The Prevalence of Antibiotic Resistance for All the Klebsiella pneumoniae Isolates Collected
Detection of antibiotic resistance and virulence genes
The various resistance genes were detected at different prevalences (Table 3). The blaSHV gene was the most prominent among isolates (Table 3); however, it showed no significant (p ≥ 0.05) association with the other screened resistance genes. A significant association (p < 0.05) was only observed between the following resistance genes: blaTEM and blaCTX-M group 1; blaTEM and aac(3′)-II; blaTEM and aac(6′)-Ib; blaTEM and qnrB; blaCTX-M group 1 and aac(3′)-II; blaCTX-M group 1 and aac(6′)-Ib; blaCTX-M group 1 and qnrB; aac(3′)-II and aac(6′)-Ib; aac(3′)-II and qnrB; and aac(6′)-Ib and qnrB. All the virulence genes screened were significantly (p < 0.05) associated with one another and were highly abundant among isolates (Table 3).
The Prevalence of the Resistance and Virulence Genes in All the Klebsiella pneumoniae Isolates Collected Within the Hospital Environment
Investigating clonality using ERIC-PCR
The genetic diversity among 48K. pneumoniae isolates was investigated using ERIC-PCR. At each hospital, ward and site, these selected isolates had a unique antibiogram and resistome. The isolates revealed 20 different ERIC-types (A to T) based on a similarity of ≥60%. At cutoff ≥80%, a total of 27 ERIC-types were displayed containing 13 major clusters (major cluster assigned when n ≥ 2, n = number of isolates) (Fig. 2). In contrast to all the other ERIC-types, which were hospital-specific, ERIC-type T consisted of isolates from tertiary hospital B and regional hospital C (Fig. 2). Within the major ERIC-types, none of the ESBL and non-ESBL isolates clustered together. Major ERIC-type K consisted of isolates regarded as 100% identical and recovered from the sheets of an occupied and an unoccupied bed in the ICU of tertiary hospital B (Fig. 2). Major ERIC-type M consisted of isolates from the sink and sheet of an occupied bed in the ICU of tertiary hospital B. These isolates shared a similarity of ≥80% (Fig. 2). Within their respective clusters, isolates from ERIC-type F and ERIC-type H, shared a similarity of ≥60%. ERIC-type F consisted of genetically similar isolates obtained from the sink and occupied bed in the general ward of district hospital D. ERIC-type H consisted of genetically similar isolates from the sheet of occupied and unoccupied beds in the general ward of central hospital A (Fig. 2).
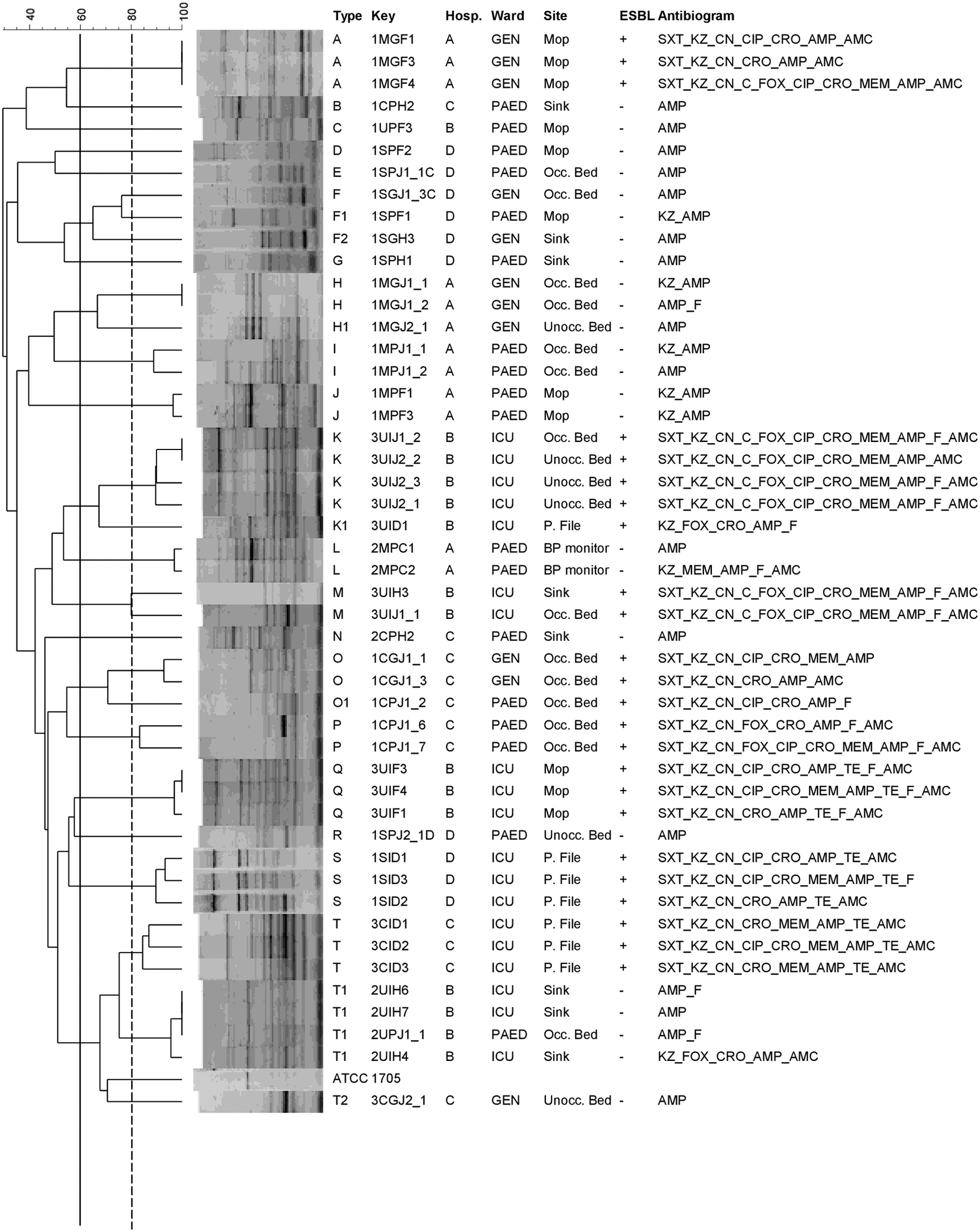
Dendrogram depicting the ERIC-PCR profiles from 48 Klebsiella pneumoniae isolates. K. pneumoniae ATCC BAA 1705 was used for quality control purposes. The red solid line at 60% specifies the ERIC-type cutoff, whereas the dashed line at 80% specifies the major ERIC-type cutoff. Hosp., Hospital; A, Central Hospital; B, Tertiary Hospital; C, Regional Hospital; D, District Hospital; PAED, pediatric; GEN, general; Occ. Bed, occupied bed; Unocc. Bed, unoccupied bed; P. File, Patient File; + indicates an ESBL-producing isolate and − indicates a non-ESBL-producing isolate; AMP, Ampicillin; KZ, Cefazolin; FOX, Cefoxitin; CRO, Ceftriaxone; MEM, Meropenem; CIP, Ciprofloxacin; CN, Gentamicin; AMC, Amoxicillin-clavulanate; F, Nitrofurantoin; SXT, Trimethoprim-sulfamethoxazole; TE, Tetracycline; C, Chloramphenicol. ERIC, enterobacterial repetitive intergenic consensus.
Discussion
A study involving public hospitals situated in KwaZulu-Natal, South Africa, was conducted to determine the prevalence, clonality, virulence, and antibiotic resistance profile of K. pneumoniae recovered on frequently encountered surfaces in the hospital environment. The overall prevalence was 10%, and this low prevalence is relatively similar to the 11.5% reported in Uganda 31 and the 11.6% reported in Ethiopia, 32 involving the recovery of Klebsiella from the hospital environment.
Tertiary hospital B had an overall higher prevalence of K. pneumoniae compared to central hospital A (Fig. 1A). Although both these hospitals can receive referral patients from other provinces, the former hospital contains more beds, thus it can accommodate more patients. The higher influx of patients may influence environmental contamination leading to a higher prevalence. Similarly, this can possibly explain the higher prevalence of K. pneumoniae in district hospital D compared to regional hospital C (Fig. 1A), as the former hospital contains more beds. In addition, district hospitals support primary health care facilities as they provide services to patients referred from community health care centers or clinics. Furthermore, they also serve as a gateway for patients to access specialized care. 18 This dual function may also contribute to a higher inflow of patients. The number of people present in the hospital environment is one of the factors that can influence the quantity and types of microorganisms detected. 8
Health care textiles such as bedsheets and staff uniforms may play a role in the dissemination of bacteria. 33 In this study, K. pneumoniae was recovered from the bedsheets of occupied and unoccupied beds (Fig. 1C). The high prevalence on occupied beds is expected as bedsheets used by patients can be contaminated with bodily substances (blood, skin, urine, and stool) containing a high number of microorganisms. 33 Carbapenem-resistant K. pneumoniae has also been detected in hospital bed linen surrounding the pillow in a study conducted in China. 34 Hospital care workers can touch these surfaces during patient care, and in the absence of hand hygiene, be disseminated throughout the hospital. The identification of K. pneumoniae on the linen of unoccupied beds is worrisome because a patient who is admitted and assigned to that unoccupied bed is at risk of developing a HAI caused by K. pneumoniae. Currently, the information that exists regarding the survival of microorganisms on hospital textiles after laundering differs among researchers due to the different temperatures investigated. 33 Furthermore, even if laundry processes are efficient at removing microorganisms, recontamination can occur if there is negligence at various posthandling processes such as sorting, ironing, folding, and packing. 35
Hand washing sinks were the second most abundant site where K. pneumoniae was recovered (Fig. 1C). Moist environments such as sinks favor the survival of gram-negative bacteria. 36 Sinks also accommodate the formation of bacterial biofilms and are an ideal environment where bacteria can exchange resistance genes through horizontal gene transfer.37,38 It has been suggested that when hand washing occurs in a pathogen contaminated sink or sink drain, the hands of hospital care workers can be colonized with bacteria due to backsplash. Contaminated hands can come into contact with patients during routine care activities, thus demonstrating a possible route of transmission. 39 A K. pneumoniae outbreak linked to a contaminated handwashing sink has been reported in Sweden. 40 This suggests that the effective and efficient cleaning of sinks in hospitals should be emphasized.
Patient files are constantly handled by hospital care workers to write daily notes after attending to a patient during routine checks and after performing medical procedures. 41 In this study, K. pneumoniae was also detected on patient files (Fig. 1C). Patient files are vulnerable to contamination because they are often placed on multiple surfaces such as nursing stations and patient beds. Ineffective hand hygiene between handling these contaminated files and touching patients increases the probability of transmission.41,42 Previous studies conducted in Saudi Arabia 41 and Taiwan 42 have also reported the recovery of K. pneumoniae from patient files.
Only 30 of the 75 (40%) K. pneumoniae isolates recovered were characterized as ESBLs, thus correlating with the resistance to ceftriaxone detected (Table 2). The ESBL percentage reported in this study is lower compared to previous studies conducted in Egypt 43 and Ethiopia, 44 where K. pneumoniae accounted for 56.25% and 42.10% of the ESBL isolates recovered from hospital surfaces and equipment, respectively. These differences among the various countries may be due to several factors. First, the higher or lower usage of ESBL selecting β-lactam antibiotics and second, the implementation of IPC measures may vary from optimal to suboptimal. Antibiotic-resistant bacteria emerge due to selection pressure; however, these microorganisms are maintained within the hospital environment due to inadequate IPC measures. 45
A high quantity of ESBLs was detected in tertiary hospital B (Fig. 1A). The referral system suggests that medical conditions presented at health care facilities become increasingly complex and severe as the hospital classification levels progress, leading to the higher usage of antibiotics, especially broad spectrum antibiotics. 46 When third-generation cephalosporins are used, the outcome is the emergence of ESBLs. 47 These results are consistent with a study conducted on clinical isolates obtained from 16 different public hospitals situated in KwaZulu-Natal, which found that the number of ESBL-producing bacteria was highest in tertiary hospitals followed by regional and then district hospitals. 46 Central hospital A also deals with complex medical cases, but it had a lower prevalence of ESBLs (Fig. 1A). Compared to other hospitals included in this study, central hospital A has more financial and medical resources that can be directed at improving IPC measures. Several factors influence the implementation of IPC measures. These factors include limited financial resources, inadequate infrastructure and poorly implemented systems. The latter consists of the unsatisfactory purchase and distribution of supplies such as hand disinfectant.48,49
A significant (p < 0.05) proportion of the ESBLs recovered was from ICU (Fig. 1B). This finding is possibly attributable to the high intake of antibiotics in this ward as it is specifically designed for critically ill patients.36,50 Frequently administered antibiotics are often broad-spectrum and constant exposure can facilitate the emergence of MDR bacteria. 51
Majority of the ESBLs were MDR, and they exhibited higher levels of resistance compared to non-ESBLs (Table 2). A similar finding was also reported in a previous study conducted in Egypt, 43 involving isolates recovered from hospital surfaces. The resistance to gentamicin, ciprofloxacin, and all the β-lactams screened in this study (Table 2) is of great concern as antibiotics from the aminoglycoside, fluoroquinolone, and β-lactam class are often used to treat infections caused by bacteria within the Enterobacteriaceae family such as K. pneumoniae. 52
Most isolates showing phenotypic resistance to gentamicin (Table 2) harbored the aac(3′)-II gene (Table 3). This gene was detected simultaneously with aac(6′)-Ib in some isolates but at a lower prevalence (Table 3). Not all the isolates exhibiting phenotypic resistance to ciprofloxacin (Table 2) tested positive for qnrB (Table 3). This suggests that other mechanisms were involved in this resistance. The high prevalence of the blaSHV gene (Table 3) is possibly due to the presence of the blaSHV-1 gene on the chromosome, resulting in the intrinsic resistance to ampicillin. 53
A great number of the ESBLs harbored the blaCTX-M resistance gene. Only variants belonging to group one were screened and detected. The group one primer set collectively targeted group one variants such as CTX-M-1, CTX-M-3, and CTX-M-15. 27 The latter is most commonly detected in Africa. 15 This study found that the blaCTX-M gene was significantly (p < 0.05) associated with the aminoglycoside and fluoroquinolone encoding genes screened and detected in most ESBL isolates. Coresistance phenotypes to aminoglycosides and fluoroquinolones have been linked to the CTX-M type ESBL. 15 These results coincide with a study conducted in Algeria reporting the detection of group one variants (CTX-M-15 and CTX-M-3) in ESBL-producing K. pneumoniae isolates recovered from hospital surfaces. Furthermore, in most isolates, the study also showed the association of the blaCTX-M gene with qnrB and aac(6′)-Ib; however, most of the isolates carried the aac(6′)-Ib-cr variant. 54
Type 3 pili play a significant role in biofilm formation on abiotic surfaces, whereas enterobactin is a common siderophore secreted by K. pneumoniae to acquire bound and unbound iron in the host environment. Iron is an important element needed by the bacterium to thrive during an infection.13,14,55 These virulence factors are encoded by the mrkD and entB genes, respectively. In this study, the overall prevalence of the mrkD gene was 95% (Table 3). This high prevalence is relatively similar to the 92% reported in Algeria 55 and the 96% reported in Brazil, 56 involving the recovery of K. pneumoniae from medical devices and clinical isolates. However, the frequency of the entB gene observed in this study (92%) (Table 3) is slightly lower than the 100% reported in Brazil. 56
Genetically related isolates within major ERIC-type M were isolated from the sheet of an occupied bed and sink in the ICU of tertiary hospital B. Similarly, related clones of ERIC-type F were noted from different sites (the occupied bed and sink) in the general ward of district hospital D (Fig. 2). By inserting a fluorescent marker into a sink drain cover, Hota et al. 57 showed that during a 15-sec handwash, fluorescent residues were transmitted and detected in the immediate vicinity as well as 1 m from the sink. Researchers further suggested the probability of undetected microparticles traveling further than 1 m. 57 Kotay et al. 37 demonstrated that when a sink strainer or sink bowl was colonized with green fluorescent protein-expressing E. coli, dispersion of the microorganism to surrounding surfaces occurred when the faucet was turned on. 37 Furthermore, when water tap handles are contaminated with bacteria, there is a chance of hand recontamination occurring upon contact, which can nullify any handwashing that has happened. 58 The recontamination of hands can result in the dissemination of bacteria if contact is made with other sites.
Major ERIC-type K consisted of genetically similar isolates originating from the sheet of an occupied and unoccupied ICU bed in tertiary hospital B. Genetically related isolates within ERIC-type H were derived from a sheet of an occupied and unoccupied bed in the general ward of hospital A (Fig. 2). The failure to adhere to IPC measures is a likely cause. However, due to the detection of K. pneumoniae on the sheets of unoccupied beds, hospital textiles, including laundry and linen services, should not be excluded when investigating possible routes of transmission. There is a clustering of genetically similar isolates (ERIC-type T) between tertiary hospital B and regional hospital C (Fig. 2). This is most likely possible because patients in hospital C can get referred to hospital B when they require services that are not offered by regional hospitals, but present in tertiary hospitals.
The study was, however, limited by the lack of sequence analyses that precluded the determination of ESBLs variants and carbapenemase-associated resistance in the hospital environments, warranting further studies that ascertain these resistance determinants.
Conclusion
This study is one of the very few hospital environment-based studies conducted in South Africa. It highlighted the prevalence of K. pneumoniae on various frequently touched hospital surfaces and equipment, which can be further disseminated to other sites if IPC measures are suboptimal. This was further supported by the recovery of genetically similar isolates from different surfaces within the same hospital. Some of the isolates recovered were characterized as ESBLs and showed high resistance to clinically significant antibiotics. Overall, the study emphasized the importance of regular monitoring of the hospital environment. The findings of this study can assist IPC staff to identify the possible sources of transmission and to assess as well as improve current IPC interventions in place.
Footnotes
Acknowledgments
The authors express gratitude to the participating hospitals, along with the IPC staff. They also thank Prof Olaniran Ademola for allowing them to use the BioNumerics software to construct the dendrograms. Finally, they thank Dr Akebe Luther King Abia for his technical assistance.
Authors' Contributions
Coconceptualized the study: N.Z.Z.M., C.O.S., D.G.A., O.T.Z., and L.A.B. Performed the laboratory work: N.Z.Z.M. Analyzed the data: N.Z.Z.M., C.M., D.G.A., and L.A.B. Wrote the article: N.Z.Z.M. Undertook critical revision of the article: all.
Data Availability
The generated data used to support the findings of this study are included within the article.
Disclaimer
Any views, findings, conclusions, or recommendations conveyed in this study are those of the author (s), thus they do not represent the organizations that supported the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors acknowledge the funding received from the UKZN College of Heath Sciences Young Research Grant (L.A.B.).