
Abstract
We modified rapid polymyxin Nordmann–Poirel (RPNP) test, called rapid colistin disk elution (RCDE) test, for detecting colistin resistance in Gram-negative bacilli and evaluated its performance compared with colistin broth disk elution (CBDE) test recommended by Clinical and Laboratory Standards Institute (CLSI). The RCDE test was performed by using a 10-μg colistin disk in 2.7 mL volume (final colistin concentration of 3.7 μg/mL) of either cation-adjusted Mueller–Hinton broth or phenol red broth base media with bacterial inoculum of 1-μL loop, and 1–4 and 16–20 hr incubation for Enterobacteriaceae and Acinetobacter baumannii isolates, respectively. Both tests were evaluated in 236 Enterobacteriaceae and 49 A. baumannii isolates using broth microdilution as reference method. Among the Enterobacteriaceae isolates, categorical agreement and very major error (VME or false intermediate susceptibility) rate were 98.3% and 5.4%, respectively, for the RCDE test, compared with 97.9% and 7.1%, respectively, for the CBDE test. Both tests had major error (ME or false resistance) rate of 0.6%. For the A. baumannii isolates, the RCDE and CBDE tests gave high VME rates of 8.3% and 16.7%, respectively. The RCDE test showed good performance comparable with the CBDE test but is cheaper and more rapid (3 hr) and convenient, thus suggesting as an alternative for detecting colistin resistance among Enterobacteriaceae in low-income countries.
Introduction
Colistin or polymyxin E has bactericidal activity by the interaction between its cationic polypeptide and anionic lipid A of lipopolysaccharide (LPS) in outer membrane of Gram-negative bacteria. 1 This agent was introduced and not widely used because of its neurotoxicity and nephrotoxicity. However, it has been reused as one of the last resorts for the treatment of infections with carbapenem-resistant Gram-negative bacteria, particularly Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacteriaceae, which are presented as a growing concern worldwide. 2 After increased clinical use, acquired colistin resistance in these bacteria has been reported in many countries. The most common mechanisms of colistin resistance are the LPS modifications by mutations of two-component regulatory systems such as PhoP/PhoQ and PmrA/PmrB, 1 resulting in the addition of positively charged molecules to the LPS. These lead to the decrease in the binding between colistin and lipid A. In 2015, the first plasmid-mediated colistin resistance, named mobilized colistin resistance-1 (mcr-1) gene, was found in Escherichia coli. 3 Currently, mcr-1 to mcr-10 genes have been identified mostly in Enterobacteriaceae. 4 Worryingly, the occurrence of colistin resistance genes on plasmids could result in their rapid and global dissemination among Gram-negative bacilli particularly those with carbapenem resistance, leading to limited therapeutic options. Therefore, rapid detection of colistin resistance among these bacteria is urgently needed.
The standard method for colistin susceptibility testing is the determination of minimum inhibitory concentration (MIC) by broth microdilution (BMD) method.5,6 However, it is time consuming (16–20 hr) and impractical for low-resource laboratories. Other methods such as disk diffusion and gradient diffusion methods commonly used in routine testing are not recommended because of poor diffusion of large colistin molecule in agar medium.7,8 Nordmann et al. 9 developed the rapid polymyxin Nordmann–Poirel (RPNP) test for detecting colistin resistance in Enterobacteriaceae. It is based on the detection of acid metabolites of glucose from bacterial growth in the presence of colistin by observing the color change of phenol red from red to yellow. This test gave low sensitivity to detect colistin resistance in Enterobacter spp., 10 whereas the performance of the commercial rapid polymyxin Acinetobacter test (Elitech Microbiology) was controversial, 100% sensitivity and specificity studied by Lescat et al. 11 in contrast to 41.2% sensitivity and 86.1% specificity reported by Kon et al. 12 Recently, Simner et al. 13 have developed the colistin broth disk elution (CBDE) test based on colistin disk elution in cation-adjusted Mueller–Hinton broth (CA-MHB). This test is now recommended by the Clinical and Laboratory Standards Institute (CLSI) for detecting colistin resistance in Enterobacteriaceae and P. aeruginosa. 5 Although the CBDE test can assume MIC values of colistin, it requires seven disks of 10 μg colistin for each test isolate, and large amount of media and glassware as well as long incubation period (16–20 hr). Therefore, a rapid and simple screening test for colistin resistance in Gram-negative bacteria is still needed for routine laboratory.
The original RPNP test 9 requires special agent such as colistin sulfate powder, which may not be available in routine or low-resource laboratories. In contrast, the CBDE test needs large amount of materials, making it laborious and more expensive. We, therefore, modified the RPNP test, named rapid colistin disk elution (RCDE) test, by the use of a 10-μg colistin disk instead of colistin solution or seven colistin disks with either Mueller–Hinton broth (MHB) or phenol red broth (PRB) media. The performance of the RCDE test was then evaluated and compared with the CBDE test, recommended by CLSI, 5 using the BMD method as gold standard.
Materials and Methods
Bacterial isolates
A total of 285 nonduplicate clinical isolates of Enterobacteriaceae (n = 236) and A. baumannii (n = 49) obtained from patients in Srinagarind Hospital, Khon Kaen University, Thailand, between 2010 and 2020 were used. The Enterobacteriaceae isolates included 138 Klebsiella pneumoniae, 49 E. coli, 42 Enterobacter cloacae, 2 Pantoea (Enterobacter) agglomerans, 3 Citrobacter freundii, 1 Klebsiella aerogenes, and 1 Klebsiella oxytoca. All test isolates were identified by conventional biochemical tests 14 followed by VITEK®2 automated system (bioMérieux, Marcy-l'Étoile, France) for species unidentified isolates. They were of different strains based on their biotypes, antibiograms, enterobacterial repetitive intergenic consensus polymerase chain reaction (ERIC-PCR) or pulsed-field gel electrophoresis profiles.5,14–16 All colistin-resistant (CL-R) isolates were screened for the presence of the most prevalent mcr-1 by PCR method, 17 of which three E. coli isolates carried mcr-1. E. coli ATCC 25922 with colistin MICs of 0.25–2 μg/mL was used as a colistin-intermediate (CL-I) control strain, whereas an mcr-1-harboring K. pneumoniae clinical isolate with colistin MIC of 4 μg/mL from a hospital in northern Thailand was used as a CL-R control strain.
This study was approved (October 22, 2019) by the Ethics Committee of Khon Kaen University (project No. HE581434).
Colistin MIC determination
The BMD method was performed using colistin sulfate (Sigma-Aldrich, St. Louis, MO) concentrations ranging from 0.25 to 32 μg/mL according to the CLSI guidelines 18 and interpreted using the CLSI breakpoint. 5 Isolates are categorized as CL-I and CL-R when colistin MICs are ≤2 and ≥4 μg/mL, respectively.
RCDE test
The RPNP test was modified by using a 10-μg colistin disk (Oxoid, Basingstoke, Hampshire, United Kingdom) with either MHB (Oxoid) or PRB (Himedia, Mumbai, India). The conditions for the RCDE test were optimized, including (1) incubation times at 15, 30, and 60 min for allowing colistin to elute from the disk into 2.7 mL of the medium (final colistin concentration of 3.7 μg/mL); (2) inoculum sizes of 1-μL loop, 5 μL (half of 10-μL loop) and 10-μL loop of test isolates (inoculum sizes of ∼108, 109, and 109 CFU/mL, respectively); (3) incubation times at 35°C for 1, 2, 3, 4, 6, and 16–20 hr; and (4) result interpretation by observation of color change of the medium from orange to yellow. Eleven CL-R (3 K. pneumoniae, 3 E. coli, 2 E. cloacae, and 3 A. baumannii) and 20 CL-I isolates (7 K. pneumoniae, 5 E. coli, 2 E. cloacae, 2 C. freundii, and 4 A. baumannii) were used for optimization experiments. Further experiments were blind testing under optimal conditions obtained as described hereunder.
The RPNP solution was prepared as described by Nordmann et al. 9 If a commercial CA-MHB medium is unavailable, the MHB medium was manually cation-adjusted as follows. In brief, the solution consisted of 2.5 g of MHB (containing 4.305 μg/mL calcium ion [Ca2+] and 4.704 μg/mL magnesium ion [Mg2+]), and 0.005 g of phenol red (Sigma-Aldrich) in 90 mL of distilled water. The pH was adjusted to 6.7 by adding drops of 1 M HCl, followed by autoclaved at 121°C for 15 min. After cooled down at room temperature, the medium was added with 10 mL of 10% anhydrous D(+)-glucose (Carlo Erba Reagents, Milan, Italy), 149 μL of 10 mg/mL of Ca2+ and 44 μL of 10 mg/mL of Mg2+ (final concentrations of 20 and 10 μg/mL, respectively) sterilized by filtration. 18 For the PRB medium, it contained 1.6 g of PR broth base (0.002% phenol red) and 1 g of anhydrous D (+)-glucose in 100 mL of distilled water. The pH was adjusted to 7.0 by adding drops of 1 M HCl and the medium was autoclaved at 118°C for 15 min. After cooled at room temperature, the medium was added with 200 μL of 10 mg/mL of Ca2+ and 100 μL of 10 mg/mL of Mg2+ (final concentrations of 20 and 10 μg/mL, respectively).
Each isolate was performed in two test tubes of size 13 × 100 mm, tubes A (growth control) and B (test), each containing 2.7 mL of the medium. Tube B was then added with a 10-μg colistin disk, left at room temperature for 30 min and finally mixed by vortex for 15 sec. A 1-μL loop of bacterial colonies was inoculated into each tube. Both tubes were incubated at 35°C and interpreted by observation of yellow color after incubation at every 1 hr for 4 hr for the Enterobacteriaceae isolates and 16–20 hr for the A. baumannii isolates. The color change of the phenol red from orange to yellow in both tubes were interpreted as CL-R, whereas those observed in tube A only were considered CL-I.
CBDE test
The CBDE test was carried out by the method of Simner et al. 13 For each isolate, four tubes each containing 10 mL CA-MHB were added with 0, 1, 2, and 4 colistin disks (Oxoid) and incubated at room temperature for 30 min to generate final colistin concentrations of 0 (growth control), 1, 2, and 4 μg/mL, respectively. A 50 μL volume of bacterial suspension adjusted its turbidity to 0.5 McFarland standard (final inoculum of 7.5 × 105 CFU/mL) was added into each tube (tubes 1–4) and mixed gently by vortex. Colistin MICs were visually inspected after 16–20 hr incubation at 35°C.
Reproducibility testing
Three CL-R (two K. pneumoniae and one A. baumannii with colistin MICs of 4, 32, and 4 μg/mL, respectively), two CL-I K. pneumoniae and A. baumannii (2 μg/mL), and E. coli ATCC 25922 (0.5 μg/mL) isolates were subjected to the RCDE, CBDE, and BMD methods on 3 separate days. All isolates were performed in duplicate for the three tests.
Statistical analysis
Owing to the lack of a susceptible category for colistin, intermediate result was considered susceptible for evaluating the performance of each test. The sensitivity and specificity of each method were calculated using the BMD method as gold standard. Categorical agreement (CA), very major errors (VMEs), and major errors (MEs) were calculated in accordance with the CLSI guidelines. 19 The CA is the total number of isolates tested by any screening test that gives either CL-I or CL-R results in the same categorical interpretation as the reference method. The VMEs and MEs correspond to false intermediate susceptibility and false resistance, respectively. Acceptable rates of the CA are ≥90%, whereas those of the VMEs and MEs are <3%. 19 All tests were repeated if an isolate showed categorical disagreement between the BMD method and any test. If the repeat result confirmed the first result, a categorical error was confirmed; if the repeat result was changed, the third testing was performed as the final result.
Results
The optimal conditions for the RCDE test were as follows: (1) 30-min incubation time for colistin elution from the disk, which was consistent with that of the CBDE test 13 ; (2) 1-μL loop of each test isolate for inoculum size because the use of either half or full 10-μL loop gave false resistance for both Enterobacteriaceae and A. baumannii isolates; (3) 3 and 16–20 hr incubation time for the Enterobacteriaceae and A. baumannii isolates, respectively; and (4) using the same criteria as those of the RPNP test for interpretation. For the 236 Enterobacteriaceae isolates, the results were observed at every 1 hr for 4 hr and the same results were obtained at 3 and 4 hr. Therefore, the optimal incubation time was 3 hr for the Enterobacteriaceae isolates.
Regarding the reproducibility testing, all CL-R and CL-I isolates were correctly classified by all three tests. Using the BMD method, 56 Enterobacteriaceae isolates, including 40 K. pneumoniae, 9 E. coli, 6 E. cloacae and 1 E. agglomerans, were CL-R with MICs ranging from 4 to >32 μg/mL (Table 1) and 32.1% of them (n = 18) exhibited MIC of 4 μg/mL. Of the 180 CL-I isolates, 94 isolates (52.2%) showed MICs of 1–2 μg/mL. Among the 49 A. baumannii isolates, 11 of the 12 (91.7%) CL-R isolates gave MICs of 4 μg/mL, whereas 34 of the 37 (91.9%) CL-I isolates had MICs of 1–2 μg/mL (Table 2).
Evaluation of the Rapid Colistin Disk Elution and Colistin Broth Disk Elution Tests for Colistin Resistance Screening in the 236 Enterobacteriaceae Isolates Compared with the Broth Microdilution Method
MICs determined by BMD method.
BMD, broth microdilution; CBDE, colistin broth disk elution; MIC, minimum inhibitory concentration; RCDE, rapid colistin disk elution test.
Evaluation of the Rapid Colistin Disk Elution and Colistin Broth Disk Elution Tests for Colistin Resistance Screening in the 49 Acinetobacter baumannii Isolates Compared with the Broth Microdilution Method
MICs determined by BMD method.
The RCDE test using either MHB or PRB medium gave the same results and could detect colistin resistance within 2–3 hr (Fig. 1). It correctly identified 53 of 56 CL-R Enterobacteriaceae isolates within 2 hr (n = 41) or 3 hr (n = 12) (Table 1). False negatives (false intermediate susceptibility) were observed in two isolates of K. pneumoniae and one isolate of E. cloacae with MIC of 4 μg/mL. This test could detect 179 of 180 CL-I Enterobacteriaceae isolates with 1 false positive (false resistance) in a K. pneumoniae isolate with MIC of 2 μg/mL. Eleven of the 12 CL-R A. baumannii isolates gave positive results with the RCDE test, whereas false resistance was found in 4 CL-I isolates with MICs of 2 μg/mL (n = 3) and 1 μg/mL (n = 1) (Table 2). Therefore, the RCDE test provided sensitivity, specificity, CA, VME, and ME rates of 94.6%, 99.4%, 98.3%, 5.4%, and 0.6%, respectively, for the Enterobacteriaceae isolates and 91.7%, 89.2%, 89.8%, 8.3%, and 10.8%, respectively, for the A. baumannii isolates (Table 3).
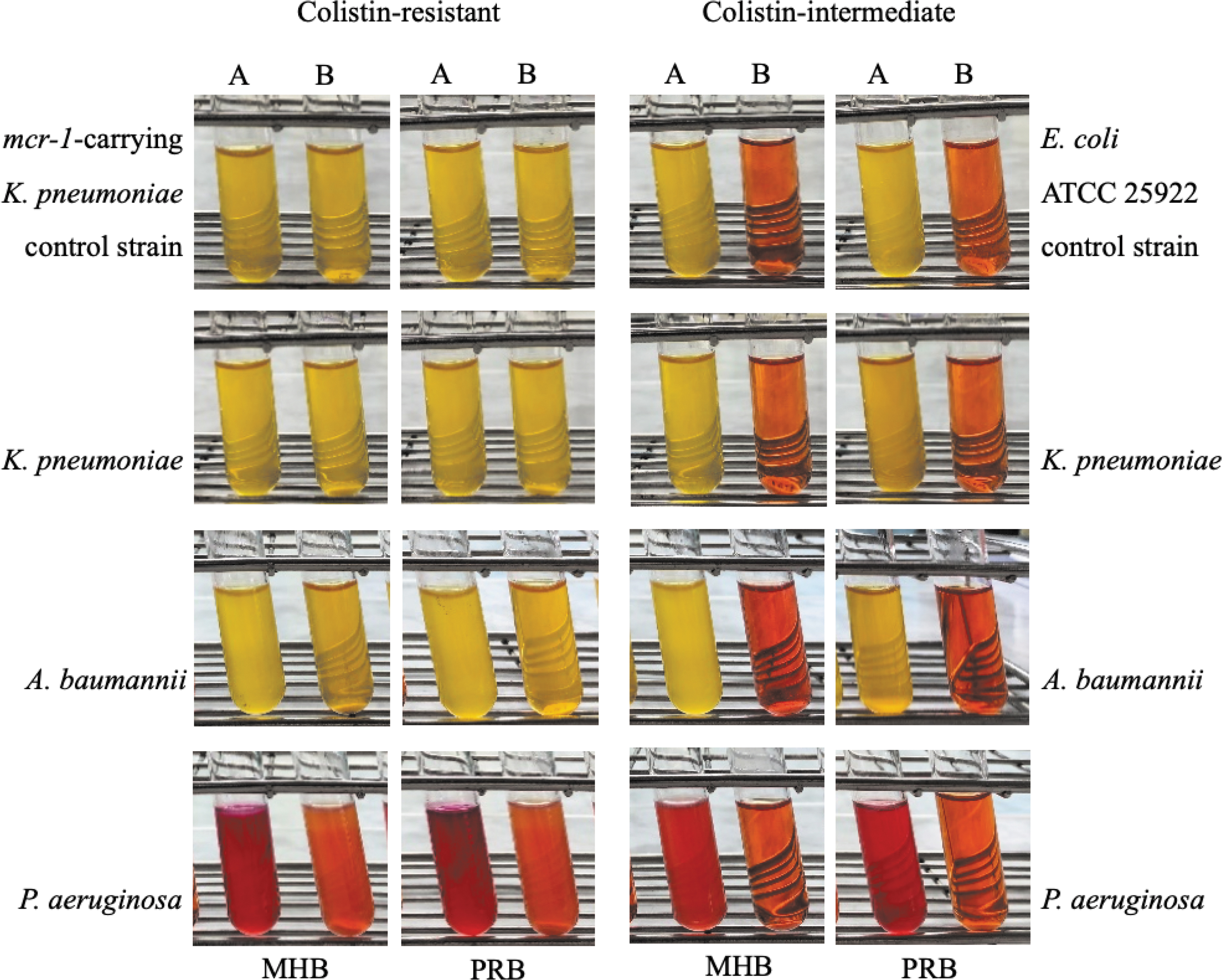
Detection of colistin resistance by the RCDE test in Enterobacteriaceae isolates within 3 hr, and Acinetobacter baumannii and Pseudomonas aeruginosa isolates within 16–20 hr. A: colistin-free MHB or PRB medium; and B: 10-μg colistin disk-containing MHB or PRB medium. MHB, Mueller–Hinton broth; PRB, phenol red broth; RCDE, rapid colistin disk elution.
The Performance of the Rapid Colistin Disk Elution and Colistin Broth Disk Elution Tests for Detecting Colistin Resistance in the Enterobacteriaceae and Acinetobacter baumannii Isolates
CA, categorical agreement; ME, major error; VME, very major error.
The CBDE test could detect colistin resistance in the Enterobacteriaceae isolates within 16–20 hr. This test incorrectly classified four CL-R Enterobacteriaceae isolates with MICs of 4 μg/mL (each of K. pneumoniae, E. coli, and E. cloacae) and 8 μg/mL (E. coli) (Table 1). In contrast, an E. cloacae isolate with the MIC of 2 μg/mL gave false resistance. The CBDE test correctly identified 10 of 12 CL-R A. baumannii isolates (Table 2). Two isolates with false intermediate susceptibility exhibited MIC of 4 μg/mL. No false resistance was observed in any CL-I A. baumannii isolate. Therefore, the CBDE test gave sensitivity, specificity, CA, VME, and ME rates of 92.9%, 99.4%, 97.9%, 7.1%, and 0.6%, respectively, for the Enterobacteriaceae isolates and 83.3%, 100%, 95.9%, 16.7%, and 0%, respectively, for the A. baumannii isolates (Table 3).
Discussion
In this study, the RCDE test was performed using a 10-μg colistin disk with either MHB or PRB medium. The PRB medium available in most laboratories was used to eliminate the phenol red preparation. If available, a commercial CA-MHB medium can be used, making the RCDE test more convenient. Although the colistin disk elution step takes 30 min longer than the RPNP test, the use of colistin disk is more convenient than preparing colistin solution. Moreover, using 1-μL calibrated loop for bacterial inoculation is easy to perform. Therefore, the RCDE test is simple, convenient, and cost-effective for identifying colistin resistance.
Among the Enterobacteriaceae isolates, the RCDE test provided the CA (98.3%) within the acceptable rate similar to that (97.9%) of the CBDE test in this study (Table 3) and to those reported previously (97.4–98.8% and 97.4–98.6% for the RPNP and CBDE tests, respectively).9,13,20–25 However, the VME rates of both tests were not in the acceptable rates (<3%) with the lower rate by the RCDE test (5.4% vs. 7.1% by the CBDE test), compared with those of previous reports (0–2% and 2.5–10.4% for the RPNP and CBDE tests, respectively).9,13,20–25 The high VME rates in our study may be due to the large number of the test isolates with MIC of 4 μg/mL (n = 18) (Table 1). The RCDE test failed to correctly characterize 3 out of the 18 CL-R isolates. In addition, only 56 CL-R isolates were included in this study. This was because of low prevalence of colistin resistance in our hospital. Further evaluation of the RCDE test in large number of CL-R isolates is needed. In contrast, both tests gave the ME rates (0.6%) within the acceptable rates, even though 17 CL-I isolates with MIC of 2 μg/mL close to the breakpoint were included in this study. Similarly, previous reports showed the ME rates of 1.8–5.1% and 0% by the RPNP and CBDE tests, respectively.9,13,20–25 The RCDE and CBDE tests showed the sensitivities of 94.6% and 92.9%, respectively, slightly higher than that (89.7%) of the CBDE test reported by Simner et al., 13 whereas the specificity (99.4%) of our study was comparable with that (100%) of the previous study. Recently, colistin susceptibility test tube has been developed using 5-mL CA-MHB with a 10-μg colistin disk (final concentration of 2 μg/mL). It provided 91.2% CA and 7.0% VME and 12% ME rates. 26 Therefore, the RCDE test showed good performance comparable with the CBDE test but is more rapid, practical, and cost-effective for colistin resistance screening in Enterobacteriaceae isolates. Combination of the RCDE test with mcr detection may be useful for prevention and control of the dissemination of these resistance determinants.
For the A. baumannii isolates, the RCDE test provided higher sensitivity (91.7%) but lower specificity (89.2%) than those (83.3% and 100%, respectively) of the CBDE tests. For the two isolates with false intermediate susceptibility by the CBDE test, one isolate was the same as that observed by the RCDE test. The remaining isolate showed skipped wells during the MIC determination by the BMD method, suggesting that the CBDE test may not be able to detect colistin heteroresistance. Similarly, four isolates with false resistance by the RCDE test may be due to the colistin heteroresistance commonly found in this organism. 27 Further confirmation by the modified population analysis profile assay revealed that these four isolates were colistin heteroresistant. 28 This may be because of the inoculum size for the RCDE test (108 CFU/mL) larger than that for the CBDE test (105 CFU/mL), thus having more chance to select CL-R subpopulation under the presence of colistin. However, the RCDE test is not suitable for applying in A. baumannii isolates, and neither is the CBDE test. 5
The CBDE test is recommended by CLSI for detecting colistin resistance in Enterobacteriaceae and P. aeruginosa isolates. 5 We also evaluated the performance of the RCDE test in 10 P. aeruginosa isolates, including 1 CL-R isolate with MIC of 4 μg/mL and 9 CL-I isolates with MICs range with 1–2 μg/mL, compared with the CBDE test. The interpretation for the P. aeruginosa isolates is different from those for Enterobacteriaceae and A. baumannii isolates by inspection of red/orange color with turbidity in both tubes within 16–20 hr incubation, indicating colistin resistance (Fig. 1). This is due to the difference in glucose metabolic pathway of P. aeruginosa from those of the Enterobacteriaceae and A. baumannii isolates. 29 It was found that both RCDE and CBDE tests showed 100% CA. However, we tested a limited number of bacterial isolates due to our low prevalence of colistin resistance in this bacterium. Therefore, further evaluation of the RCDE test in larger sample size of P. aeruginosa is necessary.
Unlike the CBDE test, the RCDE test cannot provide the colistin MICs of test isolates. This study also has some limitations that should be noted. First, the test isolates were from one hospital only. However, they were of different strains. Evaluation of the RCDE test in different regions should be further investigated. Second, apart from mcr-1 detection, chromosomally mediated mechanisms of colistin resistance were not investigated. Third, the sample size of CL-R isolates in this study was small. Further evaluation in larger samples is needed. Finally, the colistin disk tested was from one supplier only. However, the CBDE test used colistin disks from other companies such as Becton Dickinson (BD, Sparks, MD),13,21 thus implying that this commercial disk can be applied for our RCDE test as well.
Conclusion
The advantages of the RCDE test include (1) cost-effectiveness due to the use of only one colistin disk as well as of less medium and glassware; (2) convenience due to no step of adjusting turbidity of bacterial suspension to McFarland standard and of preparing colistin solution; and (3) rapidness to interpreting results within 3 hr. Therefore, the RCDE test is suggested for alternative routine testing of colistin resistance among Enterobacteriaceae isolates in low-resource laboratories. This would be useful for infection control purpose to prevent the spread of CL-R strains particularly those with plasmid-mediated mcr genes.
Footnotes
Acknowledgments
We are grateful to Ms Ampai Supajeen, Clinical Microbiology Laboratory, Nan Hospital, Nan province, for kindly providing the mcr-1-harboring K. pneumoniae isolate used as the CL-R control; and staff of Clinical Microbiology Laboratory, Srinagarind Hospital, Khon Kaen, Thailand, for collecting the clinical isolates.
Authors' Contributions
Individual contributions of each author were as follows: conceptualization and supervision by A.C.; methodology and writing—original draft preparation by A.N., A.C., and K.L.; resources (samples collection) by A.N. and C.S.; investigation by A.N.; data processing and writing—review and editing by A.N., A.C., K.L., A.L., N.C., P.T., and C.S. All authors reviewed and approved the article, and also have read and agreed to the published version of the article.
Disclosure Statement
We declare no competing interests.
Funding Information
This study was supported by KKU Research Fund (Project Nos. 600011 and 6100017). We thank the Graduate School, Khon Kaen University, for providing scholarship for A.N. (Student Grant No. 611H11).