
Abstract
Antibiotic-resistant bacteria can leave hospitals and therefore contaminate the environment and, most likely, humans and animals, through different routes, among which wastewater discharge is of great importance. This study aims to assess the possible role of hospital sewage as reservoir and dissemination pathway of carbapenem-resistant Gram-negative bacilli (GNB). Carbapenem-resistant GNB were selectively isolated from wastewater collected from a public hospital in Batna, Algeria. Species identification was carried out using matrix-assisted laser desorption and ionization time-of-flight mass spectrometry, and antibiotic susceptibility was evaluated by the disc diffusion method. β-Lactamase production was investigated phenotypically using the double-disk synergy assay and the modified CarbaNP test, then the molecular mechanisms of β-lactam-resistance were studied by PCR and sequencing. Ten Enterobacteriaceae and 14 glucose-nonfermenting GNB isolates were obtained. All Enterobacteriaceae isolates were positive for OXA-48 and TEM-1D β-lactamases, where seven of them coproduced an extended-spectrum β-lactamase. VIM-2 carbapenemase was detected in six glucose-nonfermenting GNB isolates. However, three Pseudomonas aeruginosa, one Comamonas jiangduensis and one Acinetobacter baumannii isolates were positive for VIM-4 variant. In addition, NDM-1 enzyme was detected in four A. baumannii isolates. Our findings highlight the potential impact of hospital wastewater in the spread of drug resistance mechanisms outside of hospitals.
Introduction
The introduction of antibiotics into the therapeutic arsenal has significantly reduced mortality rates due to bacterial infectious diseases. Consequently, these drugs have remarkably increased longevity by up to 20 years. 1 However, rapidly after their therapeutic use, these miraculous drugs have been threatened by the emergence and spread of antimicrobial resistance. 2 This phenomenon is now a major public health concern worldwide, for which an estimated 700,000 deaths are attributed each year. 3 In late 2017, the World Health Organization published a priority list of drug-resistant pathogens requiring the development of new effective drugs, with carbapenem-resistant Gram-negative bacilli (GNB) (Pseudomonas aeruginosa, Acinetobacter baumannii, and enterobacteria) at the top of the list as of critical priority. 4
Carbapenems are the most powerful β-lactams and are often used as a treatment of last resort for infections caused by multidrug-resistant GNB. 5 Resistance to carbapenems in GNB arises from membrane permeability alteration (efflux pumps expression and porins dysfunction) and/or from enzymatic hydrolysis of the carbapenem compound through carbapenemase production. This latter is the most powerful and clinically relevant mechanism. 6 Carbapenemases constitute a diverse group of enzymes, which are assigned to three Ambler classes A, B, and D and may confer resistance to almost all β-lactam compounds. 3
Antibiotic-resistant pathogens, including carbapenemase producers, have been widely associated with clinical settings due to the selective pressure exerted by the intensive use of antibiotics. 7 Consequently, hospitals are recognized as ecological niches for antibiotic-resistant pathogens and are considered hotspots for their emergence and spread. 8 One possible route by which antibiotic-resistant bacteria can leave hospitals, and therefore contaminate the environment, and most likely humans and animals, is through their wastewater discharge. 9 Indeed, hospital effluent is generated by all hospital activities and has a wide variety of characteristics depending on many factors such as the size of the hospital, the type of wards, and the number of patients admitted. 10 As a result, hospital effluent may contain significant amounts of antibiotic-resistant bacteria as well as antibiotic residues and other contaminants. 7
Several previous studies have documented the detection of bacteria resistant up to last-resort antibiotics in hospital wastewater 11 and in environments impacted by such effluents, 12 thus highlighting its role in the spread of drug resistance mechanisms. In the same context, and in light of the lack of data from Algeria, we investigated the wastewater of an Algerian hospital for the presence and diversity of carbapenem-resistant GNB as well as the molecular mechanisms involved to assess the possible role of the hospital wastewater as a reservoir and dissemination pathway of such resistance mechanisms.
Materials and Methods
Sampling, strains recovery, and identification
In November 2018, 3 sewage samples were collected from distinct wastewater outlets of a public hospital with 120 beds in Batna, Algeria. The hospital is located in the city center and involves two main wards, infectious diseases ward and pulmonology ward. In addition, it receives a wide variety of patients being a regional center for the treatment of brucellosis and tuberculosis. From this hospital, wastewater is discharged directly without any pretreatment. Wastewater had to be discharged to a wastewater treatment plant (WWTP) before its discharge into the environment. However, the WWTP is not operational since several years. So, unfortunately hospital wastewater is directly discharged into the environment through a surface water body called Wadi El Gourzi.
Samples were collected in sterile 1-L glass bottles and stored at 4°C until treatment within 2 hours. Two hundred milliliters of each sample were concentrated by centrifugation at 7,000 rpm for 15 minutes at 4°C. Subsequently, pellets were used for selective isolation of carbapenem-resistant GNB. One inoculation loop of each pellet was streaked on MacConkey agar plates supplemented with 64 μg/mL of vancomycin and 2 μg/mL of ertapenem or 4 μg/mL of imipenem. In addition, 2 mL from each pellet were enriched for 24 hours in brain heart infusion broth supplemented by the abovementioned antibiotic combinations, and 2 mL of sterile paraffin oil were added to ertapenem-containing tubes. Subsequently, one inoculation loop of each positive tube was cultured on MacConkey agar with the same antibiotic combination.
Antibiotic concentrations were chosen according to the antibiotic committee of the French society for microbiology_2018 breakpoints. We used 2 μg/mL of ertapenem to select for ertapenem-resistant enterobacteria, and we used 4 μg/mL of imipenem to select for imipenem-resistant and intermediate GNB. Cultures were incubated for 24 hours at 37°C. Representative colonies were purified and identified using the matrix-assisted laser desorption and ionization time-of-flight mass spectrometry. 13
Antibiotic susceptibility testing and phenotypic detection of β-lactamase production
The obtained strains were examined for their sensitivity to different antibiotic groups using the disc diffusion method and inhibition zone diameters were interpreted according to the antibiotic committee of the French society for microbiology breakpoints. The following antibiotics were tested: ticarcillin (75 μg), piperacillin (75 μg), ticarcillin/clavulanate (75/10 μg), amoxicillin/clavulanate (20/10 μg), piperacillin/tazobactam (75/10 μg), cefoxitin (30 μg), cefotaxime (30 μg), ceftazidime (30 μg), cefepime (30 μg), aztreonam (30 μg), ertapenem (10 μg), imipenem (10 μg), tobramycin (10 μg), gentamicin (15 μg), amikacin (30 μg), ciprofloxacin (5 μg), and cotrimoxazole (1.25/23.75 μg).
The eventual production of carbapenemases and extended-spectrum β-lactamases (ESBLs) was searched for using the modified CarbaNP-test (MCNP-test) and the double-disc synergy test, respectively.14,15
Molecular characterization of β-lactam resistance mechanisms
β-Lactam resistance encoding genes of blaKPC, blaNDM, blaVIM, blaOXA-48, blaOXA-23, blaOXA-24, blaOXA-58, blaCTX-M, blaTEM, and blaSHV were searched for by real-time PCR. Then, positive strains were confirmed by standard PCR. Amplified products were sequenced based on the Sanger's sequencing method using Big Dye terminator chemistry on an ABI 3130XL automated sequencer (Applied Biosystems, Foster City, CA). Sequence analysis was carried out using the CodonCode Aligner Software and sequences were blasted against the ARG-ANNOT (Antibiotic Resistance Gene-ANNOTation) database. 16 In addition, P. aeruginosa isolates were subjected to the amplification of the oprD gene using previously described primers. The resulting sequences were compared with the reference sequence of the P. aeruginosa PAO1 strain (GenBank Accession No. NC_002516.2). Sequences of primers used in this study are presented in Supplementary Table S1.
Multilocus sequence typing
Multilocus sequence typing (MLST) of the A. baumannii isolates was performed by PCR amplification and sequencing of the seven housekeeping genes cpn60, fusA, gltA, pyrG, recA, rplB, and rpoB and sequence types were determined according to the MLST database.
Results
Identification and antibiotic susceptibility testing
Altogether, 24 GNB isolates were recovered from the 3 sewage samples. Strains were identified as Citrobacter braakii (n = 5), Citrobacter freundii (n = 4), Raoultella ornithinolytica (n = 1), P. aeruginosa (n = 3), Pseudomonas putida (n = 3), Pseudomonas oleovorans (n = 1), Pseudomonas mendocina (n = 1), A. baumannii (n = 4), and Comamonas jiangduensis (n = 2). Strains' origin and isolation medium are presented in Fig. 1.
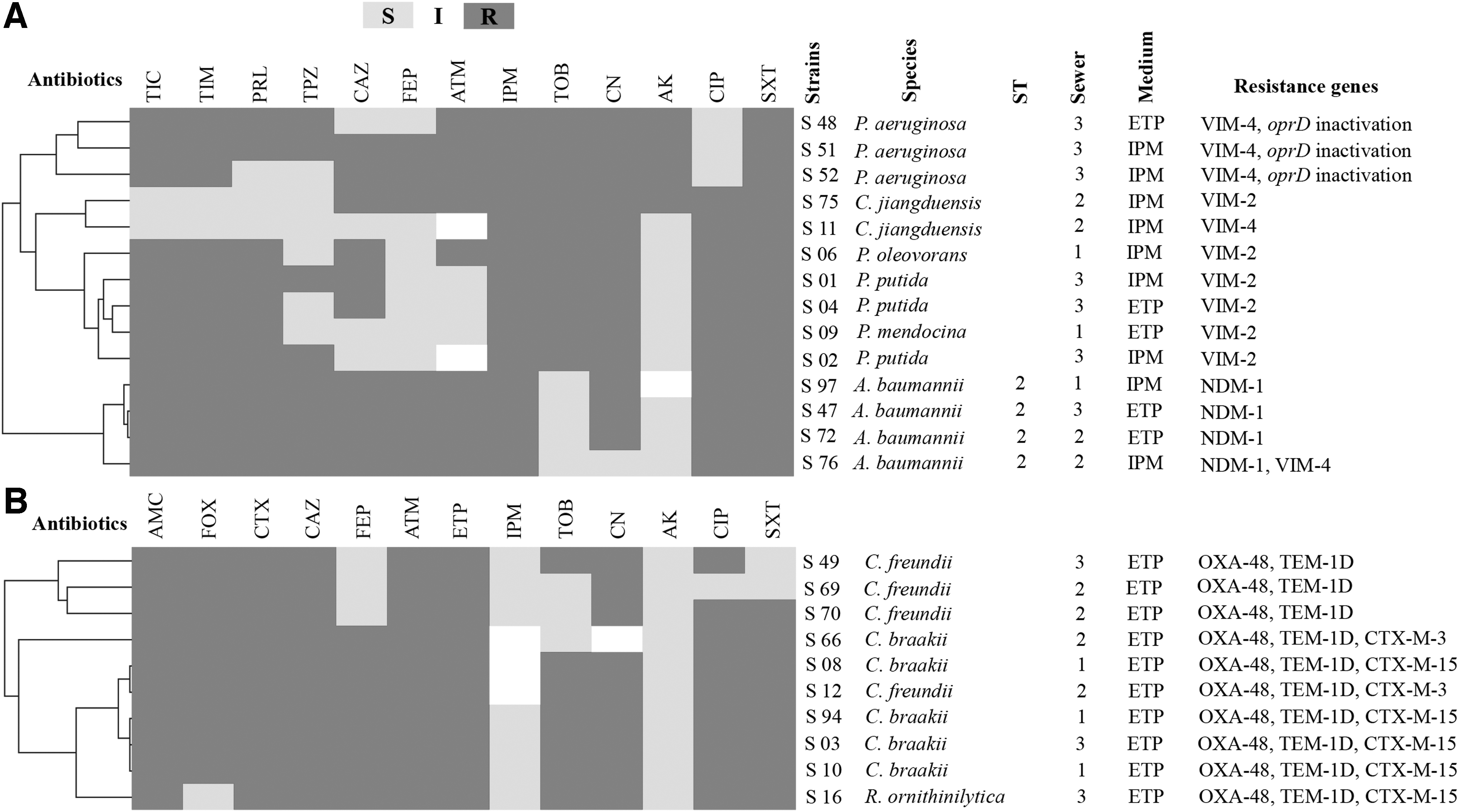
Antibiogram results, β-lactam resistance mechanisms and origins of our isolates clustered using the MEV software version 4_6_2.
Antibiotic sensitivity testing performed using the disc diffusion method showed that our isolates exhibited extensive drug resistance phenotype (three A. baumannii, four C. braakii, and one C. freundii) and multidrug resistance phenotype for the other isolates, as shown in Fig. 1. In addition, all of our isolates were positive for the MCNP-test indicating carbapenemase production.
Molecular characterization of β-lactam resistance mechanisms
All obtained isolates were subjected to molecular investigation to detect mechanisms underlining β-lactam resistance. PCR and sequencing results showed that all our isolates were positive to at least one β-lactamase encoding gene.
Regarding Enterobacteriaceae isolates, OXA-48 carabapenemase and TEM-1D β-lactamase were detected in all strains. In addition, seven of them coproduced an ESBL. CTX-M-3 ESBL was detected in one C. braakii and one C. freundii isolates. Furthermore, four C. braakii strains and the R. ornithinolytica isolate coproduced the CTX-M-15 ESBL.
In this study, we report the first detection of metallo-beta-lactamases (MBLs) in hospital wastewater in Algeria. VIM-2 enzyme was detected in P. putida, P. oleovorans, and P. mendocina isolates as well as in one C. jiangduensis strain. On the contrary, the second C. jiangduensis isolate was positive for VIM-4 MBL. In addition, three out of the four A. baumannii isolates were NDM-1 producers. Interestingly, VIM-4 and NDM-1 coproduction was detected in the remaining A. baumannii strain. Finally, our P. aeruginosa isolates associated two mechanisms of carbapenem resistance, namely the production of VIM-4 MBL and the inactivation of the oprD gene. The alignment of the fully amplified and sequenced oprD gene of the three P. aeruginosa isolates with the sequence type of PAO1 strain, allowed the detection of frameshift mutations leading to premature stop codons. The first, which was detected in two isolates, is a 4-bp insertion at position nt200. The second, detected in one isolate, was a 1-bp deletion of nt602.
Multilocus sequence typing
MLST analysis showed that all A. baumannii isolates identified in this study (n = 4) belonged to a single sequence type ST2.
Discussion
As one of our latest lines of therapy for multidrug-resistant GNB infections, 5 maintaining carbapenems' effectiveness appears to be a priority. However, in recent years, we have witnessed a wide spread of carbapenem-resistant GNB, not only in clinical settings but also in the community 17 and in the environment. 18 Besides, the strong selective pressure exerted by the dramatic use of antibiotics in health care facilities makes them important ecological niches for antibiotic-resistant pathogens. 8 These latter may leave hospitals through wastewater systems as a potential pathway for their wide spread in the environment, which is a serious public health concern, especially since it is estimated that more than 80% of wastewater (including hospital wastewater) worldwide is released into the environment untreated. 19
In the present study, we investigated one possible route of the dissemination of such drug-resistant organisms outside hospitals through the examination of hospital wastewater for the occurrence of carbapenem-resistant GNB. Our results confirmed the potential contribution of hospital sewage discharge in the spread of carbapenem-resistance mechanisms through the detection of highly drug-resistant carbapenemase-producing GNB.
In terms of detected species, carbapenemase-producing C. braakii, C. freundii, P. aeruginosa, and A. baumannii have previously been isolated from hospital sewage.20,21 However, to the best of our knowledge, we report, in this study, the first detection of carbapenemase-producing R. ornithinolytica, P. oleovorans, P. mendocina, P. putida, and C. jiangduensis in hospital wastewater.
The Ambler class “D” OXA-48 enzyme was the dominant carbapenemase detected in this study, it was detected in all of our Enterobacteriaceae isolates. This enzyme was first detected in a Klebsiella pneumoniae isolated from urinary tract infection in the Istanbul faculty hospital in September 2001. 5 It confers resistance to penicillin, but hydrolyses poorly carbapenems and it is inactive on oxyimino cephalosporins. Interestingly, our isolates coproduced either the TEM-1D β-lactamase, or the TEM-1D with CTX-M-3 or CTX-M-15 ESBLs, which may explain their high level of β-lactam resistance. The association of OXA-48 and ESBLs has been already reported in several previous studies. 22
In Algeria, OXA-48 was first described in 2014 in an Escherichia coli ST131 clinical isolate. Since then, several reports have described the isolation of OXA-48 producers in numerous Algerian cities from different sources, including clinical specimens, hospital environment, human and animal stools, and environmental samples, 5 indicating its widespread dissemination, as shown in Fig. 2.5,17,23–25 It is noteworthy that most OXA-48 producers are detected in North-Eastern Algeria, which could be attributed to the lack of studies from other regions since it has been suggested that this enzyme is endemic in that country. 26

Distribution of OXA-48 producers detected in Algeria, including those of the present study (mentioned in bold).
On the same note, five previous studies have reported the detection of OXA-48 producers in Batna from clinical samples,17,27 hospital environment 22 wild animals, 28 and recently from currency coins. 25 Despite the multiplicity of studies describing the detection of OXA-48 producers in Algeria, this is the first description of OXA-48-producing C. braakii, C. freundii, and R. ornithinolytica from hospital sewage in Algeria. Several previous studies have reported the detection of OXA-48-producing Enterobacteriaceae from hospital sewage in different countries.21,29–31
In Algeria, no studies have reported the detection of the OXA-48 variant in hospital sewage, but other variants have been described. In 2018, Yousfi et al. reported the detection of OXA-48-like carbapenemase in Klebsiella oxytoca and the OXA-416 variant in Shewanella xiamenensis isolated from hospital effluents. 32 Apart from hospital sewage, OXA-48 producers have been recovered from different aquatic environments in Algeria. OXA-48-producing E. coli, K. pneumoniae, R. ornithinolytica, C. braakii, and C. freundii have been isolated from river water in Bejaia city. 33 In addition, Mairi and coauthors have reported the isolation of OXA-48-producing Enterobacteriaceae from wastewater, river water, fountain water, and water dam in different Algerian cities. 34
Moreover, MBLs-producing glucose-nonfermenting GNB were also described in the present study. MBLs, first described in 1991, are powerful β-lactamases that hydrolyze all β-lactams, except monobactams. Members of the subclass B1, including IMP, VIM, and NDM enzymes are the most clinically relevant MBLs. 35 We report in the present study the first environmental MBL-producing GNB in Algeria and the first detection of VIM-4 MBL in aquatic habitat. VIM enzymes were first described in 1999. 35 Nowadays, several studies exist reporting the isolation of VIM producers from hospital sewage worldwide.20,29
Furthermore, in this study, four A. baumannii isolates were positive for NDM-1 enzyme. This latter was the latest MBL to be described in 2009. 35 NDM-1 has previously been detected in A. baumannii isolates recovered from hospital sewage in China in 201336 and in Bangladesh in 2017. 37 Most worrying in this study is the coexistence of NDM-1 and VIM-4 MBLs in an A. baumannii. Yet, this is not the only carbapenem-resistance mechanism association detected in the present study. Our three P. aeruginosa isolates associated MBL production and oprD gene inactivation, indicating the importance of hospital sewage as reservoir of drug resistance determinants. VIM and NDM producers were never been detected in aquatic environments in Algeria, however, several studies have reported their isolation from other sources.24,38–41
MLST results revealed that our A. baumannii isolates belonged to the widespread international clone ST2. This sequence type has been reported in Algeria from different sources with Ambler class D carbapenemase production, including OXA-23 from clinical isolates, hospital environment, and fish,41–44 and OXA-24 from clinical samples.42,44 With regard to the strains isolated from fish, it has been suggested that the contamination originates from wastewater discharge near the study site. However, MBL-producing A. baumannii ST2 have never been reported in Algeria. Regarding aquatic environments, several studies have reported the detection of MBL-producing A. baumannii in water. 45 Nevertheless, only one study reported the occurrence of carbapenemase-producing A. baumannii ST2 in aquatic habitat. This latter described the isolation of OXA-23-producing A. baumannii ST2 from WWTP in Croatia. 46 Interestingly, the authors suggested a hospital origin for these strains.
Hospitals are favorable environments for bacterial proliferation and interaction 47 and their wastewater has been largely recognized as a reservoir for carbapenem-resistant GNB. Several studies have shed the light on the role of hospital sewage in the dissemination of resistant bacteria into the environment. In a study conducted in Italy, authors reported a genetic relationship by pulsed-field gel electrophoresis between environmental carbapenemase-producing strains obtained from untreated and treated hospital sewage and clinical ones isolated in the same period. 48 In addition, a Swedish study has detected a similarity between clinical VIM-1-producing K. oxytoca isolates and those isolated from surface water receiving treated hospital effluents. 49 Furthermore, Zhang et al. suggested that the discharge of treated wastewater is a major source of the spread of high-risk resistance determinants to receiving water bodies and thus to the environment. 50
Indeed, an important part of the diffusion and the evolution of antibiotic resistance depends on aquatic environments. 51 These latter are not only reservoirs of resistant organisms, but constitute an ideal environment for horizontal gene transfer, which is of great interest as most resistance genes, including those encoding for carbapenemases, are carried by mobile genetic elements. This phenomenon may explain the carriage of MBLs by nonconventional bacterial species, such as C. jiangduensis detected in the present study, which in turn play the role of reservoirs of resistance genes facilitating their dissemination.
In the present study, we report the first detection of OXA-48 and MBL producers in hospital sewage in Algeria, highlighting its potential role in the dissemination of antibiotic-resistant GNB outside hospitals. Our findings could have serious public health implications. Therefore, further studies are required for investigating the contribution of wastewater discharge in the dissemination of resistant organisms and resistance determinants into environmental water bodies, as well as the links between human, animal, and environmental isolates. Moreover, efficient wastewater treatment processes must be followed to reduce the impact of hospital wastewater discharge into the environment.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the French Government under the “Investments for the Future” program managed by the National Agency for Research (ANR) (Méditerranée-Infection 10-IAHU-03) and the DGRSDT of the Algerian Ministry of Higher Education and Scientific Research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.