
Abstract
Infections due to extended-spectrum β-lactamase (ESBL)–producing Enterobacterales are an increasingly common problem. For many of these infections, no oral treatment options are available. The activity of amoxicillin–clavulanate combined with ceftibuten or cefpodoxime was evaluated against a group of Escherichia coli and Klebsiella pneumoniae clinical isolates possessing a variety of CTX-M- and SHV-type ESBLs; some possessed blaTEM1 as well. In time-kill studies, the combination of subinhibitory concentrations of amoxicillin–clavulanate with ceftibuten was bactericidal and synergistic for all strains with an amoxicillin–clavulanate MIC ≤32 μg/mL, regardless of the type of ESBL and the cephalosporin minimal inhibitory concentration (MIC). The combination with cefpodoxime was also bactericidal and synergistic against all but one of these strains. These combinations were further tested against two strains of K. pneumoniae and one E. coli in a sepsis model using Galleria mellonella larvae. The combination of amoxicillin–clavulanate with ceftibuten demonstrated a synergistic survival benefit against all three strains. The combination with cefpodoxime also improved survival against the two K. pneumoniae strains, but not the E. coli strain. These findings support combining amoxicillin–clavulanate with ceftibuten, and possibly cefpodoxime, for the treatment of infections due to ESBL producers and suggest that having an amoxicillin–clavulanate MIC of 32 μg/mL or less may predict activity at clinically achievable concentrations. Clinical studies are warranted to further evaluate this therapeutic approach.
Introduction
Extended-spectrum β-lactamase (ESBL)–producing Enterobacterales are an important cause of urinary tract infection (UTI) and other infections worldwide. Because of frequent resistance to oral antibiotic agents, infections caused by ESBL–producing Escherichia coli and Klebsiella pneumoniae can be difficult to treat. In 2017, the CDC estimated nearly 200,000 ESBL infections in the United States with an attributable cost of $1.2 billion. 1 A significant portion of these costs relate to increased length of hospital stay, increased drug costs, and increased administration costs all associated with the need for parenteral antibiotics such as carbapenems. Aside from resistance to oral β-lactam agents, the majority of ESBL producers have coresistance to fluoroquinolones and trimethoprim–sulfamethoxazole.2,3
Many ESBL–producing E. coli isolates are susceptible to nitrofurantoin. However, nitrofurantoin resistance rates in ESBL–producing E. coli isolates from Latin America, some European countries, and the United States have ranged from 13% to 29% in some studies.4,5 In addition, ESBL–producing K. pneumoniae are frequently resistant to nitrofurantoin. 5 Moreover, nitrofurantoin is ineffective for upper UTI and cannot be used in patients with significant renal dysfunction. Fosfomycin tromethamine has demonstrated in vitro activity against ESBL-producing Enterobacterales in the United States, particularly E. coli. 6 The use of oral fosfomycin has traditionally been limited to treatment of lower UTI due to poor systemic absorption. Several small studies of oral fosfomycin for lower UTI due to ESBL–producing E. coli have demonstrated fairly high clinical cure rates.7,8 Intermittent repeated doses of oral fosfomycin have also been used to treat pyelonephritis and other complicated UTI. 9 Most studies have been retrospective, reported low microbiologic cure rates, and higher clinical failure rates with K. pneumoniae and other species other than E. coli.8,9 In addition, fosfomycin resistance was noted to emerge in clinical studies 9 and in an in vitro pharmacodynamic bladder infection model. 10
Clavulanic acid is an older β-lactamase inhibitor, which interacts with many class A enzymes at the active site and may have activity against some ESBLs. 11 Ceftibuten and other oral “third generation” cephalosporins have been reported to have somewhat lower minimal inhibitory concentrations (MICs) for ESBL producers than earlier generation cephalosporins. 12 The addition of clavulanate to these agents significantly lowers the MICs often below the susceptibility breakpoints. 12
Two small studies reported successful treatment of outpatients with UTI due to ESBL producing bacteria with the combination of amoxicillin–clavulanate plus either ceftibuten or cefixime.13,14 Nearly all of these infections were due to E. coli. Very little clinical information was provided in these reports. In the first report, the ceftibuten MICs were unusually low (0.5–4 μg/mL), which may not be typical of most ESBL strains. 13 In the second report, no MIC information was provided, and the types of ESBLs involved were unknown. 14 The combination of amoxicillin–clavulanate with cefixime was used in two children with upper UTI. 15 However, the patients received gentamicin intravenously for 3 days with clinical response before the initiation of the β-lactam combination.
More information about the activity of this combination against a variety of strains with varied ESBL types and β-lactam MICs would clarify the general applicability of this treatment strategy. In this report, the in vitro activity of amoxicillin–clavulanate combined with ceftibuten or cefpodoxime is evaluated against ESBL–producing E. coli and K. pneumoniae, and the in vivo activity of these combinations is assessed in a Galleria mellonella sepsis model.
Materials and Methods
Bacterial isolates
Study isolates were selected from clinical isolates of E. coli and K. pneumoniae collected over a 3-month period in 2017 at seven hospitals in Brooklyn, New York. 16 Isolates were presumed to possess an ESBL if the ceftazidime and/or ceftriaxone MIC was ≥2 μg/mL, and blaKPC and other carbapenemases were absent. A subset of the presumptive ESBL isolates was chosen to include samples with three MIC patterns: ceftazidime MIC ≥ fourfold higher than ceftriaxone MIC, ceftazidime MIC ≥ fourfold lower than ceftriaxone MIC, and ceftazidime MIC within twofold of the ceftriaxone MIC. One Klebsiella pneumoniae carbapenemase (KPC)-producing isolate of E. coli was also included.
In vitro studies
MICs of amoxicillin–clavulanate, ceftibuten, and cefpodoxime were done by the CLSI broth microdilution method. 17 Genetic fingerprinting of the isolates was performed by the rep-PCR method as previously described. 18 Isolates differing by 0–1 bands were considered to be related. PCR testing for CTX-M, SHV, and TEM ESBLs was performed as previously described.16,19 Whole genome sequencing was performed on one isolate to characterize β-lactam resistance.
Time-kill studies were performed as previously described. 20 The following antibiotic concentrations, chosen to reflect clinically relevant levels, were used: Amoxicillin–clavulanate 8/4 μg/mL, ceftibuten 8 μg/mL, and cefpodoxime 2 μg/mL. In addition, each antibiotic was tested at 0.25 × MIC up to the concentrations above. Each antibiotic was tested alone, and amoxicillin–clavulanate was also tested combined with ceftibuten and with cefpodoxime. Bactericidal activity was defined as a 1,000-fold decrease in the log10 cfu/mL at 24 h. Synergy was defined as a 100-fold decrease in the log10 cfu/ml at 24 h in a combination compared to each single agent. Antagonism was defined as a 100-fold reduced killing in a combination compared to either single agent.
G. mellonella sepsis model
G. mellonella caterpillars (Grubco, Inc., Fairfield, OH) were used in a sepsis model as previously described. 20 Two strains of K. pneumoniae and one strain of E. coli for which in vitro synergy was demonstrated were selected for the in vivo study. Caterpillars weighing 180–260 mg were used. The volume of each injection of bacterial inoculum, PBS, and antibiotic solution was 10 μL. Preliminary studies of varying inocula were tested for each strain to identify an inoculum that resulted in a majority surviving 24 h but not surviving 72 h. The resulting inocula ranged from 1 × 105 to 1 × 107 cfu.
Groups of 20 caterpillars were given an injection of inoculum followed 30 min later by an injection of PBS, amoxicillin–clavulanate, ceftibuten, cefpodoxime, amoxicillin–clavulanate plus ceftibuten, or amoxicillin–clavulanate plus cefpodoxime. The antibiotic concentrations used were estimated to produce levels ∼8 μg/mL for amoxicillin–clavulanate and ceftibuten and 2 μg/mL for cefpodoxime. Amoxicillin–clavulanate was also dosed four- to eightfold lower alone and in combination with the other agents; ceftibuten was also dosed fourfold lower for one of the strains. The caterpillars were kept in Petri dishes at room temperature and monitored for 6 days. Survival rates between the groups were compared on days 3 and 6 using Fisher's exact test. This study was approved by the IRB Committee at SUNY Downstate Medical Center.
Results
In vitro studies
A total of 15 isolates of ESBL–producing E. coli and 15 K. pneumoniae were included, along with 1 isolate of KPC–producing E. coli (Tables 1 and 2). Amoxicillin–clavulanate MICs ranged from 4- > 64 μg/mL and ceftibuten MICs from 0.125- > 64 μg/mL. Cefpodoxime MICs for most isolates were >64 μg/mL. Fingerprinting by the rep-PCR method revealed eight unique strains of E. coli and nine unique strains of K. pneumoniae. The predominant ESBLs identified were CTX-M types for E. coli and SHV types for K. pneumoniae. A blaEC family class C β-lactamase was identified in one E. coli isolate (KC111). The non-ESBL TEM1 was also present in most isolates. An ESBL could not be identified in one K. pneumoniae isolate (ME31). Additional studies are underway to characterize this strain.
In Vitro Studies for Extended-Spectrum B-Lactamase–Producing Escherichia coli Isolates
Interaction between subinhibitory concentrations of amoxicillin–clavulanate and ceftibuten in time-kill studies.
Interaction between subinhibitory concentrations of amoxicillin–clavulanate and cefpodoxime in time-kill studies.
AMC, amoxicillin-clavulanate; CRO, ceftriaxone; CAZ, ceftazidime; CTB, ceftibuten; CPD, cefpodoxime.
In Vitro Studies for Extended-Spectrum B-Lactamase–Producing Klebsiella pneumoniae Isolates
Interaction between subinhibitory concentrations of amoxicillin–clavulanate and ceftibuten in time-kill studies.
Interaction between subinhibitory concentrations of amoxicillin–clavulanate and cefpodoxime in time-kill studies.
Six K. pneumoniae isolates had both CTX-M and SHV type ESBLs. In time-kill studies, amoxicillin–clavulanate alone and ceftibuten alone were bactericidal at 8 μg/mL for the isolates with MICs ≤8 μg/mL. Synergistic bactericidal activity was seen between amoxicillin–clavulanate and ceftibuten for all isolates, and with cefpodoxime for all but one isolate, with amoxicillin–clavulanate MICs ≤32 μg/mL regardless of ESBL type (Tables 1 and 2). For those isolates, synergy was seen using amoxicillin–clavulanate concentrations ranging from 1 to 8 μg/mL and ceftibuten concentrations ranging from 0.03 to 8 μg/mL.
G. mellonella sepsis model
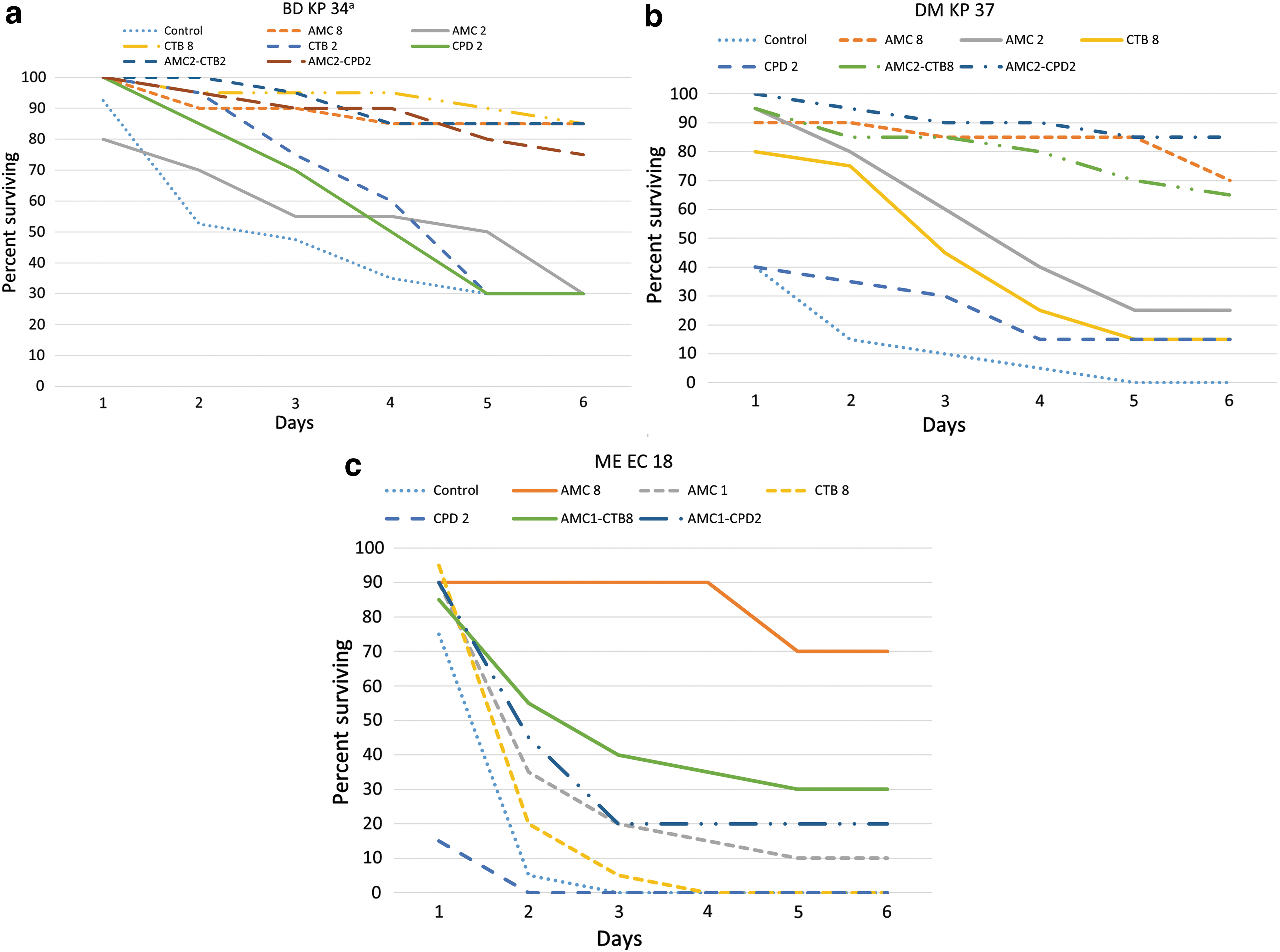
Two strains of K. pneumoniae (BD34 and DM37) and one strain of E. coli (ME18) were selected for the in vivo sepsis model (Fig. 1a–c). For all three strains, amoxicillin–clavulanate alone improved day 3 and 6 survival at a dose estimated to produce a concentration of 8 μg/mL (p < 0.002). Ceftibuten alone at a dose estimated to produce a concentration of 8 μg/mL also improved day 3 survival for K. pneumoniae strains BD34 (p = 0.0013) and DM37 (p = 0.03) but had no effect at day 6. Cefpodoxime alone at a dose estimated to produce a concentration of 2 μg/mL was ineffective. The combination of amoxicillin–clavulanate at the lower concentrations of 1–2 μg/mL with subinhibitory concentrations of ceftibuten improved day 3 and 6 survival for all three strains (p ≤ 0.02 for all comparisons). This combination was also superior to lower dose amoxicillin–clavulanate alone at day 6 for both K. pneumoniae strains (p ≤ 0.025) but not for E. coli ME18. The combination of the lower concentrations of amoxicillin–clavulanate with cefpodoxime also improved day 3 and 6 survival for both K. pneumoniae strains (p ≤ 0.002) and was superior to lower dose amoxicillin–clavulanate alone at day 6 (p ≤ 0.01). However, this combination was ineffective against E. coli ME18.
Discussion
ESBL-producing Enterobacterales are a common cause of infections in many parts of the world. Due to the co-occurrence of resistance to other classes of antibiotics such as fluoroquinolones and trimethoprim–sulfamethoxazole, oral options for treating these infections are often unavailable. Oral therapy is generally simpler for the patients, safer to administer, and less costly to use. Oral therapy is also appropriate for most infections of the urinary tract, which is the source of many ESBL–producing bacterial infections. Oral fosfomycin has been suggested as an option for treating UTIs due to ESBL-producing bacteria. However, the effectiveness and optimal dosing for managing upper UTI are unclear. Oral fosfomycin is also much less effective against K. pneumoniae than E. coli, and resistance to both species can emerge during treatment.8–10
The dearth of oral treatment options has sparked interest in combining clavulanate with oral third generation cephalosporins. Reduced MICs and other measures of in vitro synergy have been reported with the combination of amoxicillin–clavulanate with cefixime, ceftibuten, cefpodoxime, and cefdinir.12,21,22 Two small studies reported on the use of amoxicillin–clavulanate combined with either ceftibuten or cefixime for UTI.13,14 The first study involved isolates that all possessed CTX-M type ESBLs and had unusually low ceftibuten MICs that may not be generalizable to other cases. 13 The second study provided no ESBL typing or MIC data. 14 The clinical information provided in both studies was very limited.
In this report, we examined a group of contemporary clinical isolates of ESBL–producing E. coli and K. pneumoniae, including several strains with a variety of CTX-M and SHV type ESBLs and a range of β-lactam MICs. In this investigation, the in vitro studies demonstrated that both amoxicillin–clavulanate and ceftibuten have bactericidal activity at or above the MICs in the strains with relatively lower MICs. Cefpodoxime MICs were substantially higher than the clinically relevant concentrations tested in the time-kill studies. Bactericidal synergy with ceftibuten could be reliably predicted for both species regardless of ESBL type if the amoxicillin–clavulanate MIC was ≤32 μg/mL. Synergy was seen in these isolates despite ceftibuten MICs up to 64 μg/mL. The reason in vitro synergy with cefpodoxime was not seen with one K. pneumoniae strain (DM69) having a lower amoxicillin–clavulanate MIC is not clear. Bactericidal synergy was not observed in any isolate with an amoxicillin–clavulanate MIC ≥64 μg/mL at the concentrations tested.
The in vivo G. mellonella sepsis model confirmed the findings of the time-kill studies. Amoxicillin–clavulanate alone at a dose estimated to produce a level of 8 μg/mL improved survival for the three strains despite all having MICs of 16–32 μg/mL. Ceftibuten at the same dose produced similar results to a lesser extent. The most likely explanation for this finding is that the actual levels in the caterpillars, estimated based on weight and an assumption of even distribution of the antibiotics, may have been two- to fourfold higher than predicted. More significant is the finding of improved survival seen when doses expected to produce subinhibitory concentrations of the antibiotics were combined. Improved survival was seen at days 3 and 6 for all three strains by the combination using ceftibuten. The combination with cefpodoxime was effective for only two of the three strains despite having in vitro synergy for all three strains. The reason for this is unclear and may also be related to drug distribution and the antibiotic levels achieved in the caterpillars.
The findings of this study support the concept of combining amoxicillin–clavulanate with oral third-generation cephalosporins to treat appropriate ESBL infections. The MIC of amoxicillin–clavulanate, a readily available test that can be performed in any clinical microbiology laboratory, appears to be an accurate measure of the likelihood of achieving synergy with ceftibuten at clinically relevant levels. Higher concentrations of amoxicillin–clavulanate may have demonstrated greater activity when used alone, even against strains with higher MICs. However, higher concentrations are not likely to be achieved clinically using current dosing strategies. The maximum targeted level of amoxicillin–clavulanate (8/4 μg/mL) used in this study can be achieved only for a portion of the time with standard dosing. This highlights the potential benefit of combining amoxicillin–clavulanate with a cephalosporin. The combination provided activity using much lower amoxicillin–clavulanate levels that are routinely achieved in clinical practice. More clinical studies are needed to confirm the efficacy of these combinations.
Footnotes
Acknowledgment
The authors thank Ahuva Landman for her technical assistance.
Ethical Statement
This research was approved by the IRB at SUNY Downstate Medical Center.
Authors' Contributions
All authors contributed to the laboratory procedures and production of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.