
Abstract
In this study, we compared the microbiological, genotypic, and antibiotic resistance characteristics of uropathogenic Escherichia coli (UPEC) strains in patients with pyelonephritis in Korea according to sex based on data corresponding to the February 2015 to June 2018 period. Based on Escherichia coli phylogenetic group analysis, gene virulence detection, and subgroup analyses by sex, we observed that the antibiotic resistance percentages and proportions corresponding to extended-spectrum beta-lactamase producing UPEC were higher in males than in females. In addition, phylogenetic group B2 showed predominance in both the male and female groups, which further showed similar adhesion molecule distributions. Toxin-associated factors, hlyA and cnf1, were more common in males. In clinical presentations, urinary predisposing factors, complicated urinary tract infections (UTIs), concomitant bacteremia, and persistent fever were also more common with males. Although females and males showed UPEC genotypic differences, there were no differences between them with respect to poor outcomes. Persistent fever was associated with community-acquired infection and bacteremic UTI and relapsed UTI within 3 months was associated with urinary tract stone. In future, it will be necessary to conduct multicenter studies, involving more cases on UPEC to validate our results.
Introduction
Urinary tract infection (UTI) is one of the most common bacterial infections worldwide.1,2 In Korea, Escherichia coli was found to be among the causative agents of community-acquired UTI in 62.2% of male patients and 90.2% of female patients, with males showing higher antibiotic resistance percentages. 3 Multiple studies involving the exploration of the clinical characteristics of UTIs in adults in Korea have been conducted,1,3–8 and in a genotypic study of uropathogenic Escherichia coli (UPEC) conducted in other countries, analysis according to sex was primarily focused on community-onset infection.9–11
Although UTIs are more common in women, it has been reported that cases in males tend to be more severe. Several hypotheses, such as genitourinary anatomy and sex hormones, have been put forward regarding these differences in UTI prevalence and severity according to sex.8,12,13 Until now, several studies, in which UPEC strains were compared according to sex, have been reported; however, these studies tended to include only community-acquired infections.3,9,10,14,15
Thus, in this study, our objective was to explore the microbiological and genotypic characteristics of UPEC according to sex, including community-acquired infection, health care-associated infection, and nosocomial infection.
Methods
Study subjects
This study was conducted at Keimyung University Dongsan Hospital, a tertiary hospital in Korea, and involved the patients who were diagnosed with UTI caused by E. coli and admitted between February 2015 and June 2018. All the patient data were categorized under two groups, male and female, and the inclusion criteria were as follows: (1) quantitative culture isolated from midstream urine or a catheter showing E. coli at >105 colony forming unit/mL and (2) the presence of urinary symptoms, such as urgency, frequency, residual urine sense, and dysuria. This information was collected from the medical records of the patients. The exclusion criteria were as follows: patients aged below 18 years, presence of polymicrobial infections, and patients who were transferred to other hospitals during treatment. In addition, the infections were categorized as follows: community-acquired, health care-associated, and nosocomial infections.
Community-acquired infections were defined as those with symptoms that occurred within 48 hours after hospital visit, while health care-associated infections were defined as those in which patients had any health care-associated risk factors and showed symptoms before hospital admission or within 48 hours after visiting the hospital. The health care-associated risk factors included hospitalization within 90 days, hemodialysis, intravenous medication in outpatient clinics, or residency in long-term care facilities. Nosocomial infections were defined as those in which symptoms occurred at least 48 hours after hospital admission. Considering the difference in the proportions of community-acquired UTI and health care-associated/nosocomial UTI in male and female patients, subgroup analyses were conducted to determine whether these differences were associated with sex or the category of infection.
This study was approved by the Ethics Committee and Institutional Review Board of Keimyung University Dongsan Medical Center, Daegu, Korea (IRB No. 2019-05-075), and the requirement for written informed consent was waived by the committee because of the retrospective nature of the study and use of previously collected specimens.
Study design
Data collection
Medical records, including information on underlying diseases, previous antibiotics use, antibiotic resistant percentages, clinical features, antibiotics treatment, and treatment outcomes, were retrospectively analyzed. Only the medical records in our hospital system were used. Obstructive UTI was defined as UTI characterized by urinary retention due to urinary tract obstruction caused by one of the following factors without a urinary catheter: benign prostate hyperplasia, uterine prolapse, or malignancy. Urinary tract stone was not considered as obstructive UTI, but was classified as a predisposing factor. Severe UTI was defined as UTI combined with multiorgan failure or hypotension, and complicated UTI was defined as UTI with predisposing factors for persisting and relapsing infections, such as urinary tract stones, foreign bodies (e.g., indwelling urinary catheters or other drainage devices), or obstructions.
Early treatment outcomes were determined after 72 hours of empirical antibiotic use, based on persistent fever and acute kidney injury, with persistent fever defined as fever persisting over 72 hours. Late treatment outcomes were determined based on infection-related 30-day mortality (death due to UPEC within 30 days) and relapsed UTI within 3 months.
Antibiotic resistance and extended-spectrum beta-lactamase production
Clinical specimens, including blood, urine, and pus, were collected for microbe identification. In particular, E. coli strains were isolated using a Vitek system (BioMérieux, Marcy-lÉtoile, France). Antimicrobial susceptibility profiles and extended-spectrum beta-lactamase (ESBL) production were determined using Phoenix GN Combo Panels 448541 (BD Diagnostic Systems, Sparks, MD) by interpreting the breakpoints recommended by the Clinical and Laboratory Standards Institute.16,17
Phylogenetic groups
The phylogenetic groups of E. coli isolates were determined using the PCR-based method developed by Doumith et al. 18 Notably, the E. coli strains were categorized into one of the four main phylogenetic groups, A, B1, B2, and D, using four phylogenetic group markers, gadA, chuA, yjaA, and TSPE4.C2, respectively, and the groups were determined based on the different combinations of the four amplicons. Crude DNA was prepared by lysing the cell colonies at 100℃ for 15 minutes in 500 μL of sterile distilled water, followed by centrifugation. The lysis supernatant was then used for PCR under the following conditions: initial activation at 94℃ for 4 minutes, followed by 30 cycles at 94℃ for 30 seconds, 65℃ for 30 seconds, 72℃ for 30 seconds, and a final extension step of 5 minutes at 72℃. The primers used in this study are listed in Supplementary Table S1. 18
Virulence genes
Virulence genes were detected via multiplex PCR assay as previously described by Johnson and Stell. 19 The reaction was conducted with initial activation at 95℃ for 12 minutes, followed by 25 cycles of denaturation (94℃, 30 seconds), annealing (63℃, 30 seconds), and extension (68℃, 3 minutes), and a final extension (72℃, 10 minutes). The amplicons were then electrophoresed in 2% agarose gels, stained with ethidium bromide, and destained with distilled water. The primers used in this study are listed in Supplementary Table S2. 19
Statistical analysis
Statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC). The different categories were compared by performing chi-squared test or Fisher's exact test, and for p-value correction based on the multiple test theory, we used the Benjamini–Hochberg method. To test the partial effect of sex and category of infection on each factor, we used the generalized linear model, including the interaction term, and if the interaction term was not significant, it was pooled as a predominant effect. Then, the partial effect was tested. Further, to compare the nominal variables without a normal distribution, a Wilcoxon signed-rank test was performed. The Mann–Whitney U test and independent t test were also performed for variables that followed non-normal and normal distribution, respectively. Statistical significance was defined as p < 0.05.
The risk factors for poor treatment outcomes, that is, persistent fever as an early treatment outcome and relapsed UTI within 3 months as a late treatment outcome, were analyzed using logistic regression analysis in the overall cohort. An independent variable with a p < 0.05 from the univariable analysis or important clinical variables were included in the multivariable analysis and a variable with a final p < 0.05 or p < 0.1 was considered as a significant risk factor.
Results
Epidemiology
In total, 372 E. coli UTI cases were identified, 15 cases were excluded due to polymicrobial infection or transferred to other hospitals. Thus, overall, 357 patients (female, 293; male, 64) were enrolled in this study. Among them, 257 patients (72.0%) were categorized as having community-acquired UTI, while the remaining 100 patients (28.0%) were categorized as health care-associated or nosocomial infections (Fig. 1). In the female group, the distributions of community-acquired, health care-associated, and nosocomial UTI were 75.4%, 21.5%, and 3.1%, respectively, and in the male group, they were 56.2%, 32.8%, and 10.9%, respectively.
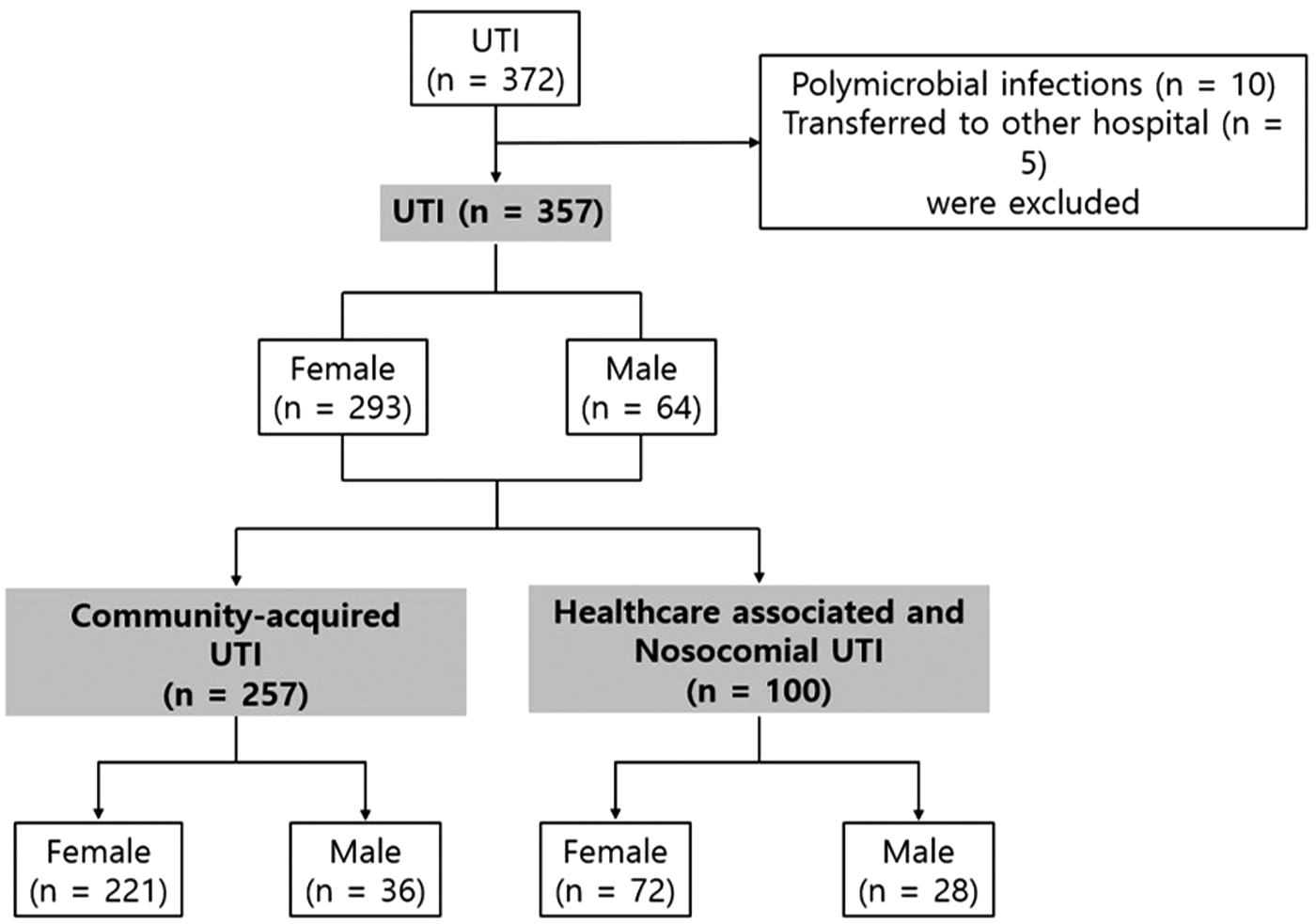
Flowchart corresponding to the patients enrolled in this study.
Basic characteristics of the study group
The median ages of the female and male patients were 73.0 and 74.0 years, respectively. Diabetes mellitus was more strongly associated with UTI in the female than in the male (43.0% in females vs. 26.6% in males), and this association was also particularly evident in the subgroup analysis involving health care-associated or nosocomial UTI cases (44.4% vs. 17.9%). Obstructive uropathy at the time of admission (1.0% vs. 42.2%) and an indwelling urinary catheter at the time of admission (5.8% vs. 18.8%) were more associated with the male than the female.
Further, neurogenic bladder features were more predominant in males with health care-associated or nosocomial UTI than in their female counterparts (13.9% vs. 32.1%). Our results also indicated that antibiotic usage within 3 months (19.1% vs. 37.5%) and intermittent urinary catheterization (0.0% vs. 4.7%) were more common in males than in females (Table 1), and regarding the previous antibiotics used within 3 months, fluoroquinolone (44.4% vs. 50.0%) showed predominance, followed by third-generation cephalosporin (42.6% vs. 50.0%) and carbapenem (14.8% vs. 16.7%).
Comparison of Clinical Characteristics According to Sex
The p-value was calculated using Fisher's exact test.
UTI, urinary tract infection.
Clinical syndromes of study group
Acute pyelonephritis was identified as the most prevalent clinical syndrome, with 99.0% and 92.2% prevalence in females and males, respectively (p = 0.006). Further, renal abscesses were accompanied by acute pyelonephritis in 8.5% of females and 4.7% of males, and in the male group, acute prostatitis and prostatic abscesses were observed in 10 cases (15.6%) and 4 cases (6.2%), respectively. Furthermore, complicated UTI was more prevalent in the male than in the female (7.5% vs. 65.6%). Moreover, in the female, health care-associated or nosocomial UTI (23.6%) showed a higher proportion of complicated UTI than community-acquired UTI (2.3%). Our analysis also indicated that bacteremic UTI was more prevalent in the male (60.1% vs. 75.0%) (Table 1). Similarly, the percentage of severe UTIs was slightly higher in the male than in the female (34.8% vs. 36.0%, p = 0.089); however, the difference was not significant.
Comparison of antibiotic resistance and ESBL production
Males showed higher antibiotic resistance percentages than females with respect to aztreonam (34.8% vs. 65.1%), cefazolin (39.9% vs. 65.1%), cefotaxime (36.5% vs. 65.1%), ceftazidime (34.8% vs. 65.1%), cefepime (34.8% vs. 65.1%), and ciprofloxacin (39.3% vs. 71.4%). When a generalized linear model was used to investigate the partial effects of sex and category of infection, it was observed that both sex and category of infection had effects on antimicrobial resistance, but no interactions were observed (Supplementary Table S3). In addition, the proportions of ESBL-producing E. coli identified using the Phoenix GN Combo Panels 448541 in females and males were 34.9% and 65.6%, respectively.
Further, all the specimens were sensitive to carbapenems, and in community-acquired UTI, the resistance percentages to ciprofloxacin in females and males were 29.1% and 50.0%, respectively, (p = 0.012). Furthermore, the proportions of ESBL-producing E. coli were 24.5% and 50.0%, respectively (p = 0.002). Regarding health care-associated or nosocomial UTI, the resistance rates to cefepime in females and males were 65.3% and 85.7%, respectively (p = 0.043), while the proportions of ESBL-producing E. coli were 50.0% and 85.7%, respectively (p = 0.057).
Comparison of phylogenetic groups and virulence factors
Phylogenetic group B2 showed predominance in both groups, followed by phylogenetic group D. Particularly, phylogenetic group B2 showed a higher proportion in the male (75.3% vs. 88.9%), whereas group D showed a higher proportion in the female (19.7% vs. 6.4%). Notably, the male and female also showed some differences with respect to the virulence factors. However, we did not observe any significant increase with respect to the occurrence of adhesion molecules in clinical isolates from male patients. A statistically significant difference was observed in community-acquired UTI, and papC was more frequently observed in the male. In addition, subgroup analysis of both community-acquired UTI and health care-associated or nosocomial UTI showed that toxin-associated virulence factors, including hlyA and cnf1, tended to be detected more frequently in the male.
Comparison of antibiotics and treatment outcomes
Regarding the analysis of empirical antibiotics, third-generation cephalosporin was most commonly used antibiotic in both groups, followed by meropenem. Specifically, for community-acquired UTI, 89.1% of females and 91.7% of males were prescribed third-generation cephalosporins, and for health care-associated or nosocomial UTI, 59.7% of females and 71.4% of males were prescribed third or fourth-generation cephalosporin, while 30.6% of females and 21.4% of males were administered carbapenems. The concordance of the initial therapy was higher in the female than in the male (73.7% vs. 45.3%, p = 0.001). During hospital stay, antibiotic treatments were modified for 281 patients (95.9%) in the female and 59 patients (93.7%) in the male.
The reason for modification was to adjust the concordant antibiotic treatment after antibiotic susceptibility testing (61 cases [22.4%] vs. 26 cases [48.1%]), the aggravation of symptoms or persistent fever (72 cases [26.5%] vs. 15 cases [27.8%]), and a switch to oral antibiotics (66 cases [24.3%] vs. 4 cases [7.3%]). The median time to modification was 3 days in the female and 2 days in the male (p = 0.001). Meropenem was the most commonly replaced antibiotic. In 38 female patients and 9 male patients, carbapenems were prescribed as initial antibiotics, and among them, 28 female (73.7%) and 5 male (55.6%) were subjected to antibiotic de-escalation. In particular, third-generation cephalosporin was the most frequently de-escalated antibiotic (9 cases [32.1%] vs. 1 case [20.0%]), followed by fluoroquinolone (6 cases [21.4%] vs. 1 case [20.0%]).
The median durations of antibiotic treatment corresponding to the female and male were 19 and 22 days, respectively, and the mean times to defervescence were 2.15 and 2.80 days for the female and male, respectively (p < 0.001). We also observed that in the female and male, persistent fever was observed in 18.4% and 40.6% cases, respectively, and the median durations of hospital stay were 10 and 16 days, respectively. However, both groups showed no significant difference with respect to 30-day mortality (1.7% vs. 1.6%) and infection-related 30-day mortality (0.7% vs. 0.0%). Even though a greater number of male patients experienced relapsed UTI within 3 months, this difference was not significant (Table 2).
Comparison of Treatment Outcomes
Significance was also observed based on the Benjamini–Hochberg method.
Risk factors for persistent fever and relapsed UTI within 3 months
Due to the low 30-day mortality rate corresponding to the cases recruited in this study, persistent fever and relapsed UTI within 3 months were considered as clinical outcomes to identify associated variables via logistic regression analysis. In this regard, univariate analysis showed that male sex, obstructive uropathy at the time of admission, community-acquired infection, bacteremic UTI, and papA, papC, papG allele II, and papG were significantly associated with persistent fever. In addition, community-acquired infections (odds ratio [OR] 2.31; 95% confidence interval [95% CI]: 1.269–4.206; p = 0.006) and bacteremic UTI (OR 2.84; 95% CI: 1.663–4.849; p < 0.001) were significantly associated with persistent fever (Table 3).
Variables Associated with Persistent Fever
Significance was also observed based on the Benjamini–Hochberg method.
CI, confidence intervals; ESBL, extended-spectrum beta-lactamase; OR, odds ratio.
Univariate analysis also showed that health care-associated infection, complicated UTI, ESBL-producing E. coli, and urinary tract stones were significantly associated with relapsed UTI within 3 months, and based on multivariate analysis, only urinary tract stone (OR 2.652; 95% CI: 1.053–6.681; p = 0.039) was significantly associated with relapsed UTI within 3 months (Table 4). Sex did not show any significant association in both outcomes. There were also no associations between the phylogenetic groups or virulence factors and both outcomes.
Variables Associated With Relapsed Urinary Tract Infection Within 3 Months
Discussion
This study revealed several differences between males and females with respect to genotypic characteristics, antibiotic resistance rates, and the clinical presentations of UPEC—induced UTI. Predisposing factors for UTI, bacteremic UTI, and persistent fever were more common in the male, which also showed higher antibiotic resistance percentages than the female. Further, hlyA and cnf1 were more frequently detected in the male, while KpsMTII was more frequently detected in the female.
E. coli strains can be classified under three main groups (commensal, intestinal pathogenic, and extraintestinal pathogenic) and four phylogenetic groups (A, B1, B2, and D). 20 UPEC, have been shown to belong to the extraintestinal pathogenic class and predominantly, to phylogenetic group B2, and less commonly to phylogenetic group D. Even though rare, UPEC strains have been identified in phylogenetic groups A and B1. Conversely, commensal strains primarily belonged to phylogenetic group A or B1.19,21 Group distributions vary based on country, sex, and clinical settings.6,22–24 For example, in a community-acquired UTI study conducted in Italy, B1 was the most common group identified in female patients. 10 In this study, no phylogenetic group differences were observed between males and females, that is, group B2 was predominant in both males and females.
UTIs tend to be more prevalent in women. 14 These differences are related to the “fecal-urethral hypothesis.” They may also be related to differences between men and women with respect to genitourinary anatomy. 12 The urinary tract structure in men offers greater protection against bacterial invasions in most cases.25,26 However, men have a greater associated morbidity. 8 The influences of sex on susceptibility to the diverse clinical syndromes of UTI and its severity are complex.27,28 In a study on bacteremic UTI in Korea, mortality was found to be higher in males. 4 Olson et al reported that estrogen did not influence the risk of occurrence of chronic cystitis, but testosterone mediated UTI severity in male mice, and that UPEC more effectively colonize at male mice bladder.
Thus, the male mice showed a higher level of susceptibility to chronic cystitis, severe acute pyelonephritis, and renal abscess. 13 Zychlinsky Scharff et al also reported the characteristics of UTIs in men and women using mouse models. Their results indicated that in female mice, UTIs could easily develop, but are often quickly resolved. In contrast, in male mice, UTIs tended to persist, possibly owing to the influence of testosterone. 8 It has also been demonstrated that androgens inhibit proinflammatory macrophages, allowing UTI-causing bacteria to continue the renal scarring process. 29
In most studies on UTI differences according to sex, comparisons were made according to sex within each group of community-acquired infection or health care-associated infection.10,15,30–32 Possibly, this is because most of the community-acquired UTI cases were female patients with fewer underlying diseases. Thus, accurate analysis might have been difficult due to associated factors. However, in this study, subgroup analyses within each category of infection were performed alongside overall analyses involving all the patients with UTI, and interestingly, multivariate analysis using a generalized linear model showed significant results according to sex. In this study, we observed that hlyA and cnf1 were more prevalent in males.
In some studies on UTI, the “special pathogenicity hypothesis” has been suggested, as opposed to the “fecal-urethral hypothesis,” considering the genetic differences between fecal and urethral E. coli. 22 Notably, UPEC contain several virulence genes that are associated with adhesins, toxins, iron acquisition, and protection. 33 In terms of pathogenic invasion, adhesion molecules are important for disease progression, play an initial role in attachment to the uroepthelium. 34 Further, hlyA and cnf1 are categorized as toxins that are important for mediating bacterial invasion via pore formation in membranes, dissemination, and bacterial persistence in the bladder,35,36 while hlyA has been shown to induce damage to the uroepithelium and augment tissue hemorrhage in murine bladder.
Further, cnf1 causes bladder inflammation through submucosal edema, 35 while hlyA reportedly causes programmed cell necrosis by altering mitochondrial dynamics. 37 It also causes the progression of bacteremia into fulminant sepsis caused by UPEC. 6 In a mouse model, the introduction of UPEC into the bladder has also been shown to significantly alter host gene expression, increasing the expression levels of proinflammatory cytokines, including interleukin-6, macrophage inflammatory protein 2, keratinocyte-derived cytokine, and tumor necrosis factor-α. It can also trigger noncytokine-mediated induction of a proinflammatory response, independent of cnf1 and/or hlyA.36–38 Considering the virulence factors of male and female UPEC, hlyA and cnf1 showed greater expression levels in males, while kpsMTII showed a greater expression level in females, confirming the existence of differences in virulence factors according to sex. However, our results further indicated that these differences in virulence factors owing to sex did not show any correlation with poor treatment outcomes.
A study in France corresponding to the 2007–2012 period indicated that UPEC showed greater resistance to ciprofloxacin and cotrimoxazole in males than in females. 39 Further, a study in Spain (2007–2009) revealed that UPEC shows greater resistance to ciprofloxacin in young men than in females without a history of exposure to ciprofloxacin during puberty. 11 This suggests that the high percentages of antibiotic resistance in men may be related to several other factors as well as previous antibiotic use. It has also been demonstrated that phylogenetic group B2 is associated with biofilm formation and antibiotic resistance. 40 In this study, higher proportions of health care-associated infection and phylogenetic group B2, as well as higher antimicrobial resistance percentages, were observed in males. Thus, further research is needed to identify which factors, including phylogenetic group, biofilm formation, or other virulence factors, exert a greater influence on antimicrobial resistance in males.
This study had several limitations. First, this study was retrospective, primarily relying on medical records and microbial cultures for analysis. Second, the patients included in this study were at a tertiary hospital; therefore, their conditions may have been more severe than those of patients in a primary medical center. Third, among all the UTI cases, only patients with UTIs caused by E. coli were included; thus, the proportion of E. coli among UTIs could not be accurately determined. Regardless of these limitations, in this study, we identified differences in the predisposing factors, clinical manifestations, antimicrobial susceptibility, and genotypic features of UPEC between males and females in a tertiary hospital in South Korea. Further multicenter studies, involving a greater number of cases of UPEC UTI are needed to validate these findings.
Footnotes
Acknowledgments
We thank Eun-Sil Park for the data fill-up. We also thank Editage for English language editing.
Authors' Contributions
M.H.: Conceptualization, data curation, investigation, methodology, formal analysis, and writing—review and editing. H.a.K.: Investigation, methodology, and writing—review and editing. J.Y.L.: Formal analysis and writing—review and editing.
Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This work was financially supported by Boryung Pharmaceutical Co., Ltd. (250346).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.