
Abstract
Streptococcus pneumoniae remains a significant cause of morbidity and mortality worldwide despite the overall success of the vaccine programs. In Tunisia, pneumococcal conjugate vaccines (PCV)10 was introduced in the national immunization program in April 2019. We sought to determine the relationship between serotypes and antimicrobial nonsusceptibility of S. pneumoniae isolates recovered from clinical samples in the prevaccination period in the south of Tunisia. A total of 504 nonduplicate S. pneumoniae isolates collected between 2012 and 2018 were tested for antimicrobial susceptibility, among them 439 (87.1%) were serotyped. The most common serotypes were 19F (17.8%), 14 (15.3%), 3 (9.1%), 19A (8.2%), and 23F (7.3%). The proportions of isolates with serotypes covered by PCV7, PCV10, and PCV13 were 55.4%, 56.3%, and 77.9%, respectively. Three-quarters (74.4%) of pneumococcal isolates were nonsusceptible to penicillin, and about half (54.8%) were multidrug resistant. Penicillin nonsusceptibility was observed for all 19A and 23F isolates, and was significantly associated with serotypes 19F (odds ratio [OR]: 33.7) and 14 (OR: 8.7). A significant association with multidrug resistance was noted for serotypes 19A (OR: 10), 19F (OR: 9.4), 23F (OR: 8.6), and 6B (OR: 5.2). The alarming rates of pneumococcal antimicrobial nonsusceptibility and the strong association with the most prevalent serotypes compel microbiologists to monitor the impact of the PCV10 introduced recently in our national immunization program.
Introduction
Streptococcus pneumoniae is a major bacterial pathogen of severe infections in children and adults worldwide. It causes both invasive pneumococcal diseases (IPDs) such as bacteremia and meningitis, and non-IPDs such as acute otitis media and nonbacteremic pneumonia. 1 In the prevaccination period and exactly in 2000, ∼14.5 million episodes of serious pneumococcal infections were estimated to have occurred, and the pneumococcal disease caused ∼826,000 deaths in children <5 years of age. 2 The pneumococcal capsular antigens are the major virulence determinant and the target of vaccination.
Currently, there are >90 known serotypes defined on the basis of differences in the capsular polysaccharide composition. These serotypes are unequal in prevalence. 3 As antibodies to the capsule are protective, pneumococcal conjugate vaccines (PCVs), which are constructed against the most prevalent serotypes, have caused great reductions in pneumococcal disease. 3 Since 2000, the 7-, 10-, and 13-valent PCVs have been used successfully in routine childhood vaccination programs across the world. 4
Population-based surveillance studies have shown that the PCV implementation reduced IPDs and non-IPDs due to pneumococcus with vaccine serotypes (VTs) among vaccinated children and unvaccinated individuals through the direct and indirect protection effect. 4 Nevertheless, pneumococcal vaccines provide serotype-specific protection. Their widespread implementation has brought shifts in the relative prevalence of serotypes with an increase in non-VTs.3,5 Thus, S. pneumoniae remains a significant cause of morbidity and mortality, especially among those at the extremes of age. 3 Of the estimated 5.83 million deaths among children <5 years of age globally in 2015, 294,000 (uncertainty range, 192,000–366,000) were estimated to be caused by pneumococcal infections.
Disease and mortality rates are higher in developing than in industrialized settings, with most deaths occurring in Africa and Asia. 5 In Tunisia, PCV7 was introduced as a voluntary vaccination in 2008, followed by PCV10 and PCV13 in 2012. These vaccines were only available in the private sector, and the vaccination rate was very low (<5%). Since April 2019, PCV10 has been introduced in the national immunization program for childhood vaccination with two primary doses at age 2 and 4 months and a booster dose at age 11 months (2 + 1 schedule).
Antimicrobial resistance in S. pneumoniae is one of the global public health concerns.4,6 The pattern of resistance varies among serotypes and geographic regions. 6 Worldwide, in the prevaccination era, most antimicrobial-resistant clinical isolates belong to serotypes 6B, 9V, 14, 19F, and 23F.6,7 However, despite the overall success of the vaccine programs, the emergence of antimicrobial-resistant non-VTs pneumococci has been reported in many countries.8,9
Since PCVs are directed at specific serotypes, it is essential to monitor the serotype distribution and antimicrobial resistance rates of pneumococci to assess the impact of a given pneumococcal vaccine. The aim of the present work was to determine the relationship between antimicrobial nonsusceptibility and serotypes of S. pneumoniae isolates recovered from clinical samples in the prevaccination period in the south of Tunisia.
Materials and Methods
Pneumococcal isolates
Between January 2012 and December 2018, a total of 504 nonduplicate S. pneumoniae isolates recovered from clinical specimens were collected at the microbiology laboratory of Habib Bourguiba University Hospital, Sfax—Tunisia. This hospital serves ∼1 million inhabitants in Sfax and other people coming from southern Tunisia. Of these pneumococcal isolates, 125 (24.8%) were invasive, collected from sterile body sites, including blood (51%), cerebrospinal fluid (30.4%), other body fluids (11%), and abscesses (7.6%). The study was approved by the Ethics Committee of Habib Bourguiba University Hospital.
Three hundred seventy-nine isolates (75.2%) were noninvasive, mostly recovered from respiratory samples (66.5%): sputum, endotracheal aspirate, and bronchoalveolar lavage, followed by ear samples (24.7%), ocular samples (6.2%), and various pus (2.6%). For 466 isolates with known age, 35.2%, 45.7%, and 19.1% were recovered from patients <5, 5–64, and >64 years of age, respectively.
Bacterial identification was based on standard procedures, including colony morphology, Gram staining, bile solubility, and optochin susceptibility. Quality control was assessed by S. pneumonia ATCC 49619 strain.
Serotyping
Serotyping was performed by sequential multiplex PCR using primers as described previously. 10 A primer pair targeting the cpsA, a gene of the capsular polysaccharide biosynthesis locus found in almost all pneumococcal serotypes, was used as an internal control. 10 Depending on the amplification pattern obtained, multiplex PCRs were followed by confirmation using a simplex PCR performed for each serotype.
Isolates that could not be serotyped by multiplex PCR were serotyped by simplex PCR using primers targeting other serotypes as described previously. 11 One representative of each serotype was confirmed by sequence analysis. Isolates determined as 6A/B, 9V/A, and 7F/A (vaccine serotypes) by the multiplex PCR method were typed to the serotype level using PCR sequencing and/or pneumococcal capsule-specific antisera (ImmuLex™ Pneumotest). Serotypes that could not be identified by our PCR were considered as “not typeable with the used method.”
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed using the disk diffusion method on Mueller–Hinton agar supplemented with 5% sheep's blood and 20 mg/L β-NAD (Mueller Hinton Fastidious Agar) according to the Antibiogram Committee of the French Microbiology Society (CA-SFM 2018) guidelines. All isolates were tested against oxacillin (1 μg), erythromycin (15 μg), lincomycin (15 μg), pristinamycin (15 μg), gentamicin (500 μg), chloramphenicol (30 μg), tetracycline (30 μg), norfloxacin (10 μg), trimethoprim/sulfamethoxazole (1.25–23.75 μg), rifampicin (5 μg), vancomycin (5 μg), and teicoplanin (30 μg).
Penicillin-nonsusceptible pneumococcus (PNSP) was defined as an isolate with a zone size for oxacillin (1 μg) <20 mm. Minimum inhibitory concentrations (MICs) against penicillin G, amoxicillin, cefotaxime, and levofloxacin were determined for all isolates by Etest method (bioMérieux SA, Marcy l'Etoile, France). The same breakpoints, CA-SFM 2018, were applied for all isolates.
The breakpoints for β-lactams were shown as follows: penicillin (susceptible: MIC ≤0.064 μg/mL, resistant: MIC >2 μg/mL), amoxicillin (susceptible: MIC ≤0.5 μg/mL, resistant: MIC >2 μg/mL), and cefotaxime (susceptible: MIC ≤0.5 μg/mL, resistant: MIC >2 μg/mL). For all tested antibiotics, isolates identified as intermediate or resistant were grouped together as nonsusceptible. Multidrug-resistant (MDR) pneumococcus was defined as resistance to three or more classes of antimicrobial agents. 12 S. pneumoniae ATCC49619 was used as a quality control strain.
Statistical analysis
Data were analyzed using IBM SPSS Statistics version 20.0. Chi-square or Fisher's exact test was used for proportions comparison, as appropriate. Changes over time (2012–2018) in serotype distribution and antimicrobial nonsusceptibility were assessed for statistically significant differences using the chi-square test for trend. A p-value of ≤0.05 was considered statistically significant.
Serotype-specific antimicrobial nonsusceptibility of S. pneumoniae isolates was determined; odds ratios (ORs) with 95% confidence intervals were calculated.
Results
Serotype distribution
Of the 504 pneumococcal isolates, 439 (87.1%) were serotyped. The remaining 65 isolates had not been preserved or had not grown. We identified 33 serotypes/serogroups. Only five isolates (1.1%) were not typeable using our PCR method. The most common serotypes were 19F (17.8%), 14 (15.3%), 3 (9.1%), 19A (8.2%), and 23F (7.3%).
The proportion of serotypes covered by PCV7, PCV10, and PCV13 were 55.4%, 56.3%, and 77.9%, respectively (Table 1). There were no significant differences in the proportions of the most frequent serotypes between IPD and non-IPD isolates (Table 1). The serotype distribution did not differ significantly between the three age groups except for serotype 6B (p = 0.049) that was significantly most common among children <5 years of age. The vaccine coverage of PCV7, PCV10, and PCV13 was significantly higher in children aged <5 years than in the two other age groups (p = 0.007, p = 0.011, and p = 0.001, respectively) (Table 1).
Serotypes Distribution and Antimicrobial Nonsusceptibility Rates of Pneumococcal Isolates by Site of Isolation and Age Category
Other serotypes, 15A, 34, 16F, 35F, 15B/C, 6C, 13, 23A, 31, 38, 28A, 33F, 7C, and 20. Bold for vaccine serotypes.
IPD, invasive pneumococcal disease; MDR, multidrug-resistant; NT, not typeable with the used method; PCV, pneumococcal conjugate vaccines.
Between 2012 and 2018, a statistically significant decrease in the proportion of serotype 19F (p = 0.006) was observed. Meanwhile, a statistically significant increase in serotype 19A (p = 0.037) was noted during this time period (Fig. 1).
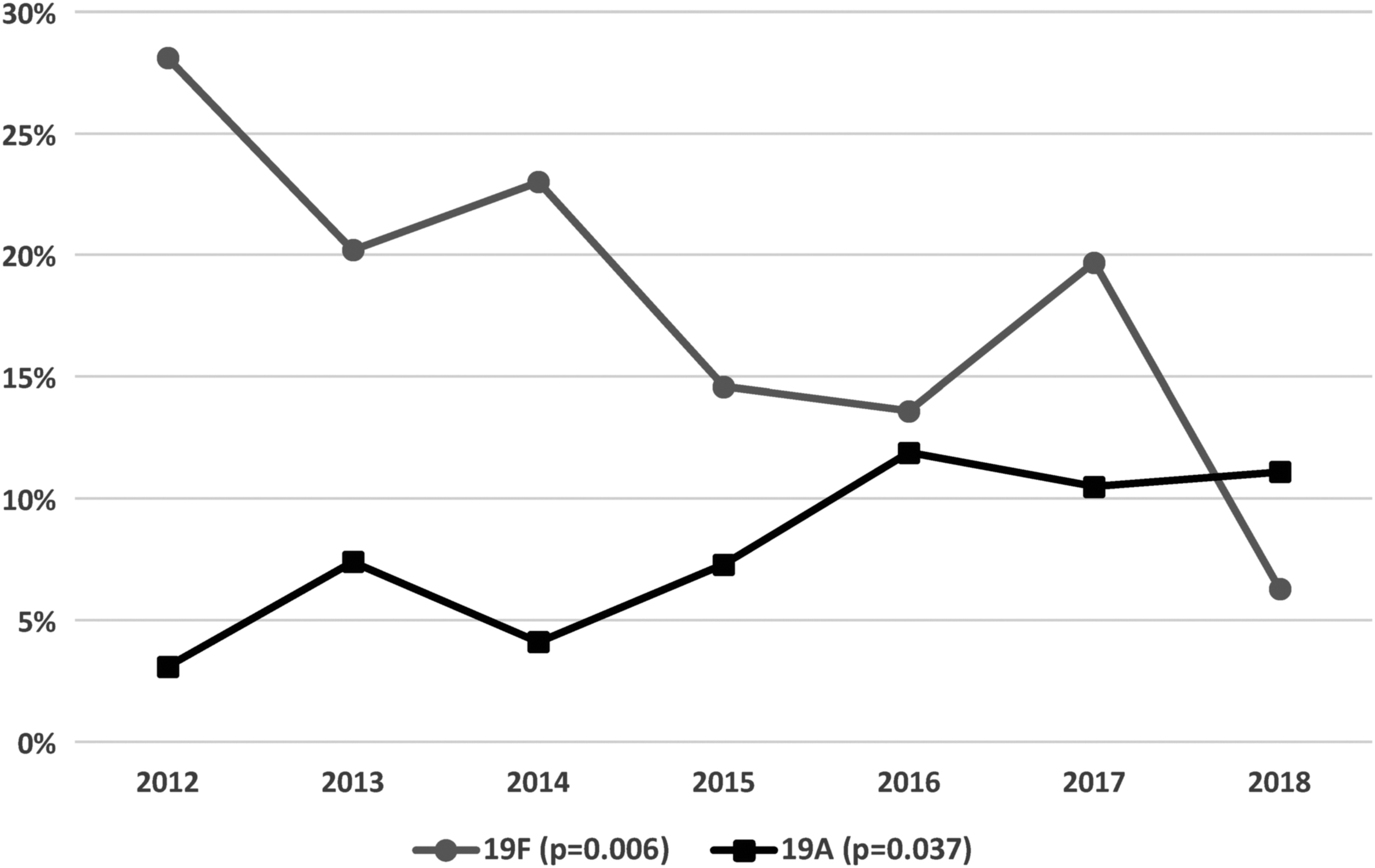
Annual distribution of serotypes 19F and 19A of Streptococcus pneumoniae isolates between 2012 and 2018.
Antimicrobial susceptibility
PNSP was identified in 74.4% of pneumococcal isolates (intermediate: 64.7%; resistant: 9.7%). Nonsusceptibility to amoxicillin and cefotaxime was detected in 48.6% (intermediate: 37.9%; resistant: 10.7%) and in 14.1% (intermediate: 13.7%; resistant: 0.4%), respectively. For antibiotics other than β-lactams, nonsusceptibility rates were 44.6% for tetracycline, 28.8% for trimethoprim/sulfamethoxazole, and 1.8% for rifampicin.
Resistance rates for erythromycin and lincomycin were 68.7% and 56.5%, respectively. For chloramphenicol, resistance rate was 7.1%. Resistance to levofloxacin was observed only in three isolates. No acquired resistance was observed for pristinamycin, vancomycin, teicoplanin, or gentamicin. The overall MDR S. pneumoniae rate was 54.8%. Most MDR isolates showed nonsusceptibility to β-lactams (98.6%), macrolides (99.6%), and tetracycline (75.4%).
Penicillin (p = 0.033), erythromycin (p = 0.029), and tetracycline (p = 0.042) nonsusceptibility was significantly higher among noninvasive isolates than invasive isolates. Moreover, a significantly higher MDR rate was noted in noninvasive isolates (p = 0.003) (Table 1).
Antimicrobial nonsusceptibility rates were significantly higher in children aged <5 years for penicillin (p = 0.033) and cefotaxime (p = 0.043) (Table 1).
Time trends of antimicrobial nonsusceptibility rates between 2012 and 2018 showed a significant decrease for cefotaxime (p < 0.001) and trimethoprim/sulfamethoxazole (p < 0.001). No significant change in the annual rates of MDR S. pneumoniae was noted (p = 0.348).
Relationship between serotypes and antimicrobial nonsusceptibility
Serotypes 19F, 14, 19A, and 23F were significantly associated with penicillin nonsusceptibility (Table 2). A significant association with nonsusceptibility to erythromycin was noted for serotypes 19F, 6B, 19A, and 23F. Three serotypes, 19F, 19A, and 6B, were associated with nonsusceptibility to tetracycline.
Serotypes Specific Antimicrobial Nonsusceptibility of Streptococcus pneumoniae Isolates
Significant and OR cannot be calculated.
CI, confidence interval; NS, not significant; OR, odds ratio.
Serotype 9V had the highest OR for trimethoprim/sulfamethoxazole nonsusceptibility followed by serotypes 14, 23F, and 6B. The three levofloxacin-resistant isolates belonged to serotypes 19F, 14, and 6A. Serotypes 19A, 19F, 23F, and 6B exhibited significantly higher rates of MDR. However, a significant association with antimicrobial susceptibility was noted for serotype 3 isolates. For MDR isolates, vaccine coverage of PCV7, PCV10, and PCV13 was 73.8%, 74.2%, and 90.2%, respectively.
Discussion
Surveillance studies of pneumococcal serotype distribution are necessary to monitor the epidemiology of S. pneumoniae and to assess the effectiveness of pneumococcal vaccines. S. pneumoniae capsular polysaccharide, the most important virulence factor, is the basis of serotyping. The prevalence of different serotypes is partially explained by the biochemical characteristics of the capsular polysaccharide. More prevalent serotypes are heavily encapsulated and increasingly resistant to neutrophil-mediated killing. These serotypes are 3, 6A, 6B, 14, 19A, 19F, and 23F.13,14
Differences in serotype distribution between countries are due to several factors. They may include the PCV introduction in the national immunization program, the difference in the vaccination rate, the use of antimicrobials (types and doses of antibiotic used), and the presence of antimicrobial-resistant clones. 8
Five serotypes of both PCV7 and PCV10 (19F, 14, 23F, 6B, and 9V) and three additional PCV13 serotypes (3, 19A, and 6A) were predominant in this study. The proportions of isolates with serotypes covered by PCV7, PCV10, and PCV13 were 55.4%, 56.3%, and 77.9%, respectively. Our results were compared particularly with reports from countries in the prevaccination period. In fact, in Tunisia, PCV7 was licensed in 2008, and was replaced by PCV10 and PCV13 in 2012.
However, these vaccines were only available in the private sector, and the vaccination rate was very low (<5%). PCV10 was incorporated into the national immunization program in April 2019. Worldwide, before PCV7 introduction, the most common serotypes were 6B, 9V, 14, 19F, 23F, and 6A.14,15 Similar findings were noted in Tunisian studies.16,17
According to the literature, a significant association of serotypes/serogroups 1, 4, 7F, 8, 9V, 12F, and 14 with invasive diseases was reported.18,19 It was suggested that capsular serotype may have an important impact on the ability of pneumococci to cause invasive diseases. 18 In our study, no significant differences in the proportions of the most frequent serotypes between IPD and non-IPD isolates were noted.
Regarding patient age, in agreement with the literature, our data show that serotype 6B was more common among children <5 years of age. In addition, vaccine coverage of PCV7, PCV10, and PCV13 was higher in children aged <5 years. Before PCV introduction, serotypes included in the PCV7 formulation were responsible for ∼90% of IPDs in young children in the United States and Canada, and ∼60% in all other regions except Asia (45%). Serotypes 6B, 9V, 14, 19F, and 23F predominated among the youngest age group and are considered as pediatric serotypes.19,20
In this study, between 2012 and 2018, the proportion of serotype 19F decreased significantly. Meanwhile, serotype 19A increased significantly. Worldwide, an increase in the prevalence of serotype 19A has been noted after the PCV7 introduction. 14 However, the emergence of MDR 19A clones like ST-320 isolates was reported before the introduction of pneumococcal vaccines in some countries.14,21,22
In our study, nonsusceptibility rates to the tested antibiotics of 504 pneumococcal isolates were high, especially for penicillin (74.4%) and erythromycin (68.7%). This can be due to antibiotic overuse in our setting.6,14,23 According to a global study, the highest rates of penicillin resistance were observed in Africa (64.3%), the Middle East (46.4%), and North America (38.5%), while the highest rates of erythromycin resistance were observed in Africa (64.3%), Asia/Pacific (28.8%), and North America (23.5%). 24
A relationship between antimicrobial resistance and pneumococcal serotypes has been reported in the literature.6,7,14,24 Before PCV introduction, most clinical isolates with high-level resistance to β-lactam antibiotics belonged to serotypes 6B, 9V, 14, 19F, and 23F.7,24 These resistant isolates often pertained to clonal groups that have also acquired resistance to other drugs, including erythromycin, chloramphenicol, trimethoprim-sulfamethoxazole, and tetracycline.7,25
These observations are consistent with our study in which serotypes 19F, 14, 23F, 19A, 6B, and 9V were associated with nonsusceptibility to at least one of these antibiotics: β-lactams, macrolides, tetracycline, and trimethoprim-sulfamethoxazole. In addition, serotypes 19A, 19F, 23F, and 6B exhibited higher rates of MDR. Despite evidence of a strong association between resistance patterns and serotypes, the genes encoding capsular polysaccharide can be exchanged between strains by transformation leading to capsular switching.7,26 Thus, it is possible that serotypes that were not associated with multidrug resistance may become members of highly resistant clones.
Capsular switching has particular implications for the conjugate pneumococcal vaccine, which confers protection against a limited number of serotypes. 7 In the prevaccination period, the highest rates of resistance occurred in VTs, which were the most prevalent serotypes. 14 In our study, the proportions of MDR isolates with serotypes covered by PCV7, PCV10, and PCV13 were 73.8%, 74.2%, and 90.2%, respectively. These results are in accordance with findings from other countries before PCV introduction or with low uptake of PCV.27–32
In this study, we found that noninvasive isolates had a higher MDR level than invasive isolates. The suggested short duration of colonization for invasive strains may explain this observation. 19 In fact, in the nasopharynx, pneumococcal strains are likely to be exposed to prolonged antibiotic pressure and to other commensal species with the ability of genetic transformation leading to the acquisition of resistance. 33
In accordance with the literature, serotype 3 was associated with antimicrobial susceptibility in this study. A constitutively high level of expression of the polysaccharide capsule in serotype 3 may impede invasiveness and the acquisition of resistance genes during colonization.19,34
Despite the overall success of the vaccine programs, pneumococcal disease treatment concerns have persisted. After the introduction of PCV into national immunization programs, VTs declined in prevalence while non-VTs increased. 14 Indeed, increased antimicrobial resistance has been observed in non-VTs, particularly serotype 19A after PCV7 introduction.8,14 Increased prevalence of resistant non-VTs may occur if antimicrobial resistance is acquired de novo or through capsular switching events, or if pre-existing resistant serotypes undergo clonal expansion. 14
In conclusion, our study showed the predominance of VTs in the south of Tunisia, the alarming rates of pneumococcal antimicrobial resistance, and the strong association between VTs and antimicrobial nonsusceptibility. Vaccination can reduce pneumococcal diseases prevalence. However, rationalizing the use of antibiotics is an important strategy to decrease the development of pneumococcal antimicrobial resistance.
Footnotes
Authors' Contributions
All authors have contributed to and agreed on the content of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Research Laboratory for Microorganisms and Human Disease (MPH LR03SP03)—Ministry of Higher Education and Scientific Research, Tunisia.