
Abstract
We aimed to assess the factors associated with 30-day mortality in patients with vancomycin-resistant Enterococcus faecium (VREf) bloodstream infection (BSI) who received treatment with linezolid in an 11-year retrospective cohort of patients with VREf BSI. A univariate and stepwise multivariate logistic regression analysis was performed to determine 30-day mortality factors. Moreover, a Cox proportional hazards analysis of predictor covariates of mortality was performed. Eighty patients were included in the final analysis; 42 (53%) died and 38 (47%) survived 30 days after the index bacteremia. Thirteen patients of 42 (31%) died in the first 7 days. The Acute Physiology and Chronic Health Evaluation II (APACHE II) score was significantly associated with 30-day mortality (adjusted odds ratio [aOR], 1.46; 95% confidence interval [CI]: 1.22–1.76; p < 0.001) in the multivariate analysis. Moreover, VREf BSI persisting for more than 48 hours was a strong factor related to 30-day mortality (aOR, 19.6; 95% CI: 1.46–263; p = 0.01). Adequate control of infection source showed a trend to be protective without reaching significance in the multivariate analysis (aOR, 0.19; 95% CI: 0.04–1.0; p = 0.05). The Cox proportional hazards analysis confirmed the same significant mortality predictor besides linezolid treatment within the first 48 hours as a protective factor (hazard ratio 0.46; 95% CI: 0.23–0.92, p = 0.02). Severely ill patients with high APACHE II score and persistent bacteremia have a higher risk of failure with linezolid therapy.
Introduction
Vancomycin-resistant Enterococcus sp. (VRE) is a leading etiologic agent of health care-associated infections, with vancomycin-resistant Enterococcus faecium (VREf) becoming the most prevalent. 1 During the last decade, VRE-causing bloodstream infections (BSIs) have progressively increased and spread across Europe and United States, with rates varying from 31% to 82%.2,3 Moreover, VREf BSIs have been associated with higher mortality (odds ratio, 1.80) than vancomycin-susceptible E. faecium and increased hospital length of stay. 4 These findings might be explained by high resistance rates and a limited number of effective antimicrobials for VRE BSI, 5 since an appropriate antibiotic selection within the first hours of enterococcal BSI is vital to treatment success. 6
The cornerstone of treatment is based on linezolid and daptomycin; the former is a bacteriostatic oxazolidinone with broad-spectrum activity against Gram-positive organisms, including VRE, and was approved by the FDA for bacteremia due to VRE. Whether linezolid is the best option for VRE BSI remains controversial. 7 Several systematic reviews and meta-analyses with data until 2012–2014, which included about 3,229 patients, showed lower mortality rates with linezolid than daptomycin, although these meta-analyses included studies with obvious heterogeneities among groups and treatment selection bias.8–10
A recent large retrospective cohort study that included 644 patients showed in the Poisson regression analysis that linezolid was associated with higher 30-day mortality (risk ratio [RR], 1.15; 95% confidence interval [CI]: 1.02–1.3) than daptomycin therapy. 11 Therefore, given the lack of the appropriate guidelines for selecting the best antibiotic treatment for each patient with VRE BSI, the purpose of this study was to assess the factors associated with treatment failure measured as 30-day mortality in patients with VREf BSI treated with linezolid. These results will provide the clinical and microbiologic characteristics of patients who might be candidates for alternative antibiotic therapies.
Methods
Setting, study population, data collection, and definitions
We conducted a retrospective cohort study to assess clinical risk factors associated with failure to linezolid therapy for VREf BSI. The study was carried out between January 2007 and January 2018 at the Instituto Nacional de Ciencias Medicas y Nutricion Salvador Zubiran, a tertiary care center in Mexico City, Mexico.
We did a retrospective review and retrieving of the electronic medical database. The data collected were as follows: demographics; clinical such as comorbidities, time and place of bacteremia onset (a health care-associated infection was considered if the date of bacteremia onset occurred on or after the 3rd calendar day of hospital admission 12 ), primary (central line-associated BSI) or secondary bacteremia which were defined according to the most recent manual from the Centers for Disease Control and Prevention, 12 source control (defined as the appropriate identification and management of the primary or secondary source of bacteremia) as reported by the clinicians, and illness severity; microbiological features; antimicrobial treatment, and time to start linezolid therapy after the positive blood culture was drawn.
Outcomes such as all-cause mortality at 7- and 30 days, and length of bacteremia which was defined as the time in days between the index VREf-positive blood culture and the first negative blood culture (persistent bacteremia was defined as the positivity of follow-up blood cultures >48 hours after the index VREf-positive blood culture was drawn).
The included patients were ≥18 years old, with at least one positive blood culture for E. faecium that met the definition of resistant to vancomycin and susceptible to linezolid; therefore, they received treatment with linezolid to conventional dosage empiric or based on the antimicrobial susceptibility results. Exclusion criteria were: (1) patients with duplicate episodes; only the first episode was considered. (2) Patients that received sequential treatment with linezolid (i.e., a patient who started treatment with another antibiotic with activity against VREf and further linezolid was added) or a combination of therapy with linezolid and another antibiotic agent active against VREf. (3) Patients with incomplete medical records.
Identification and antimicrobial susceptibility
Blood cultures were performed in Aerobic/F medium (Becton Dickinson, Shannon, County Clare, Ireland), and detection with BD BACTEC™FX 200 (BD Diagnostic Systems, Sparks, MD) BacT/Alert 3D system was used for the analysis of blood cultures. The identification of the species and susceptibility to vancomycin and linezolid were performed using VITEK 2 system and the AST-GP67 card (bioMérieux, Durham, NC) with antibiotic breakpoints according to updated Clinical and Laboratory Standards Institute Guidelines for Performance Standards for Antimicrobial Susceptibility Testing criteria (CLSI M100). 13 Linezolid minimal inhibitory concentration (MIC) was classified as follows: susceptible, ≤2 μg/mL; intermediate, 4 μg/mL; and resistant, ≥8 μg/mL.
Statistical analyses
Numeric variables were expressed as means or standard deviations if there was a normal distribution or as medians and ranges if there was a nonparametric distribution. Student's t test or Mann–Whitney test was performed. The categorical variables were expressed by absolute and relative frequencies, and comparisons were made by the chi-square test.
A stepwise logistic regression analysis was performed, and results in the univariate analysis with p ≤ 0.1 were included in the multivariate analysis, which was adjusted for multiple potential confounders to identify risk factors associated with mortality at 30 days after the VREf BSI episode treated with linezolid. Moreover, a Cox proportional hazards analysis of predictor covariates of 30-day mortality was performed, and for adjustment of differences on treatment duration, the subjects were right censored at the end of linezolid treatment. p-Value <0.05 was considered statistically significant. All statistical analyses were performed using R software 3.6.1 (R Core Team, 2019; http://www.R-project.org/).
Results
There were 107 patients with nonduplicate episodes of VREf BSI, of which 27 were excluded (Fig. 1). Eighty patients met inclusion criteria whose 219 VREf isolates had a MIC ≤2 μg/mL in 98% (214/219) and a MIC of 4 μg/mL in 2% (5/219). Forty-two patients (53%) died, and 38 (47%) survived 30 days after the index bacteremia.
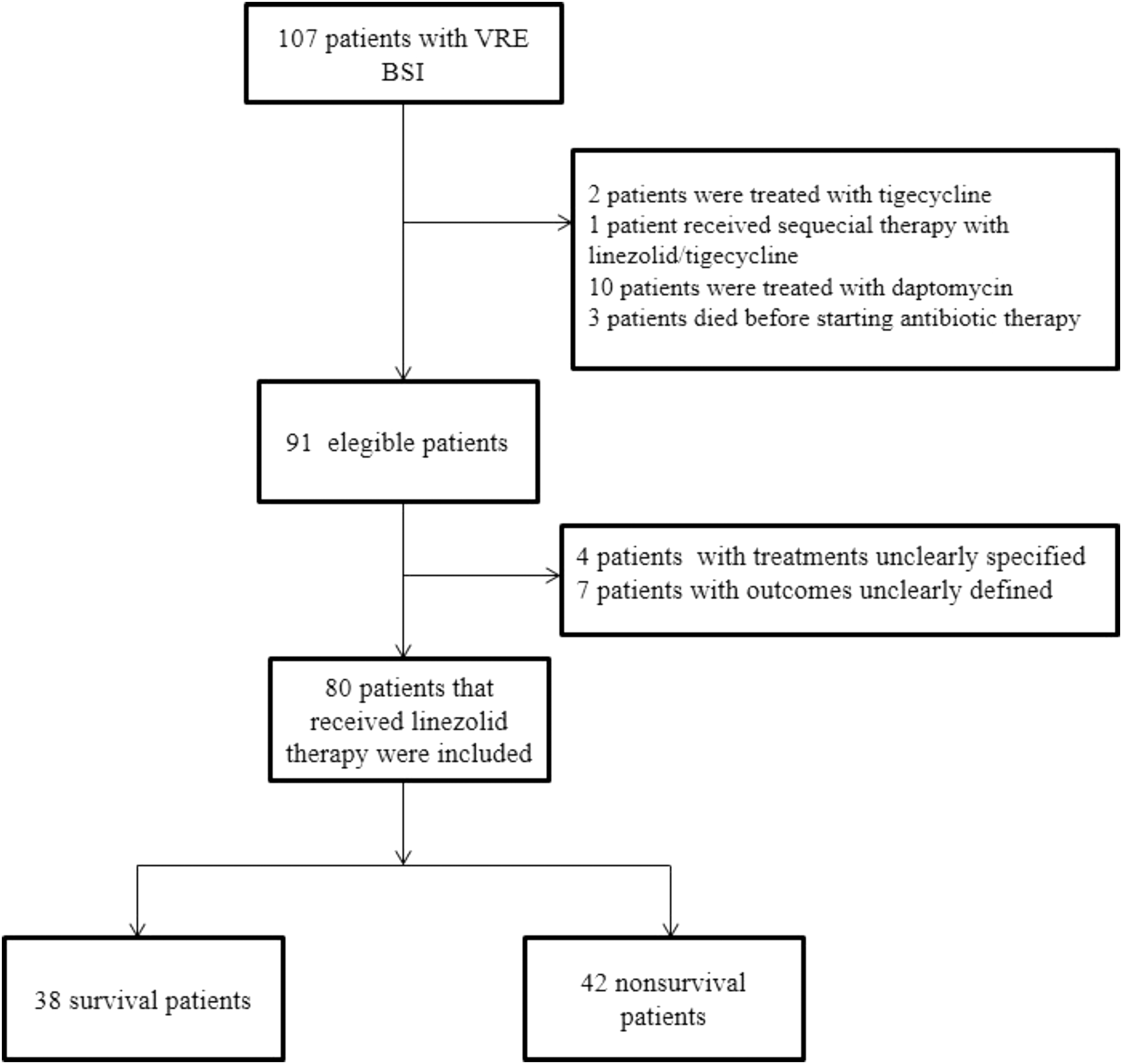
Flowchart of cases included with vancomycin-resistant Enterococcus faecium bacteremia treated with linezolid. One of the patients treated with tigecycline received a combination with linezolid and meropenem, and two patients treated with daptomycin received linezolid as well.
The median age of the studied population was 48 years without significant differences between survivor and nonsurvivor patients. There was a higher proportion of females with 41/80 (51%) patients and comprised 20/42 (48%) nonsurvivor patients. All the VREf BSI episodes included were health care-associated onset. The main hospital location was the general ward, with 28/38 (74%) among survivors, and the intensive care unit was in 25/42 (60%) of nonsurvivors. The median Charlson comorbidity index in both groups was three, and in a total of 57 patients (71%), their index score was minor to 5. More common underlying diseases were type-2 diabetes mellitus, cancer, liver disease, hematological malignancies such as acute lymphoblastic leukemia, and lymphoma (Table 1).
Baseline Patient Demographic Data and Clinical Characteristics by the Outcome of Patients with Vancomycin-Resistant Enterococcus faecium Bloodstream Infections Treated with Linezolid
Tacrolimus, mycophenolate, cyclosporine, and biologic agents.
AML, acute myeloid leukemia; APACHE II, Acute Physiology and Chronic Health Evaluation II; CKD, chronic kidney disease; HIV, human immunodeficiency virus; ICU, intensive care unit; IQR, interquartile range; NPH, nocturnal paroxysmal hemoglobinuria.
There were 25 central line-associated BSI, and the principal source of secondary bacteremia was intra-abdominal, particularly from the biliary tract. All patients had an invasive device represented for central venous catheter (100%), nasogastric tube (95%), urinary catheter (100%), endotracheal cannula (38%), and percutaneous biliary drainage catheter (27%). The percentage of patients who underwent surgical procedures before the bacteremia episode reached up to 62% in the survivors and 47% in the nonsurvivors (Table 1). The use of immunosuppressive medication was presented in half of the overall cohort. Nineteen patients (45%) in the nonsurvivors and six (16%) in the survivors had the use of at least two immunosuppressive drugs (Table 1).
The median duration of linezolid therapy was significantly lower in nonsurvivors (10 days; interquartile range [IQR], 5–14) than survivors (13 days; IQR, 10–14; p = 0.01). The nonsurvivor patients had a median Acute Physiology and Chronic Health Evaluation II (APACHE II) score significantly higher than survivor patients. The length of bacteremia was 2 days (IQR, 1–3 days) determined in 29/42 (69%) of nonsurvivors and 2 days (IQR, 1–2 days) among 17/38 (45%) survivors. There were no significant differences in the rest of the baseline characteristics (Table 1). The adverse events were present in low proportion, with only 2/80 (2.5%) patients presenting thrombocytopenia. One patient was in the survivor group and the other in the nonsurvivors.
Thirteen of 42 patients (31%) died in the first 7 days after the first positive blood culture for VREf. A higher number of patients who died in the first 7 days had immunosuppression-associated conditions than the survivors beyond 7 days (73% vs. 42%, p = 0.03). In addition, more patients had bacteremia persisting more than 48 hours (38% vs. 12%, p = 0.031), a higher median APACHE II score (29 vs. 19 points, p = 0.001), and a low number of patients who had an appropriate maneuver to control the infection source (31% vs. 73%, p = 0.007).
In the univariate analysis of significant risk factors for 30-day mortality, bacteremia persisting >48 hours and APACHE II score were strong risk factors. Starting appropriate treatment within 48 hours of the index bacteremia was a significant protective factor against mortality (Table 2).
Factors Associated with 30-Day Mortality in Vancomycin-Resistant Enterococcus faecium Bloodstream Infections Treated with Linezolid
Tacrolimus, mycophenolate, cyclosporine, and biologic agents.
Calculated in the first 24 hours since the positive blood culture was drawn.
Time in hours elapsed since the positive blood culture was drawn.
aOR, adjusted odds ratio; APACHE II, Acute Physiology and Chronic Health Evaluation II; CI, confidence interval; OR, odds ratio.
The multivariate analysis showed that variables such as APACHE II score and persistent BSI for more than 48 hours remained significant risk factors. Adequate control of infection source was a protective factor in the univariate analysis; however, in the multivariate analysis of 30-day mortality, it only showed a small trend to be protective without reaching significance (Table 2). The multivariate Cox proportional hazard analysis of 30-day mortality factors also showed that APACHE II score (hazard ratio [HR] 1.11; 95% CI: 1.05–1.17, p < 0.001) and persistent BSI for more than 48 hours (HR 2.48; 95% CI: 1.16–5.28, p = 0.01) were strongly associated with 30-day mortality. Starting appropriate treatment within 48 hours of the index bacteremia showed to be protective (HR 0.46; 95% CI: 0.23–0.92, p = 0.02).
Discussion
The mortality rate of patients with VREf BSI treated with linezolid was as high as 53% in this study. Mortality was strongly associated with the disease severity represented by a higher APACHE II score in the index bacteremia and persistent BSI. These factors remained the most significant ones for 30-day mortality. Interestingly, adequate control of infection source and early initiation of therapy showed a trend of decreasing mortality in patients treated with linezolid.
The preferred antibiotic treatments for VRE BSI are mainly limited to linezolid and daptomycin with discordant results from several meta-analyses that favored linezolid8–10 and large retrospective studies that showed lower mortality with daptomycin.11,14 A more recent meta-analysis by Shi et al. compared linezolid versus daptomycin showing similar clinical and microbiological outcomes. 15 Nowadays, the availability of the two drugs is broad because they have been sold as generic since 2015–2016, and a cost-effectiveness analysis showed similar cost/life saved and cost/quality-adjusted life year. 16
Overall, the optimal regimen for VRE BSI is a matter of controversy; thus, the focus of this study was based on linezolid therapy, which showed a high mortality rate (31%) for VREf BSI during the first 7 days. A retrospective cohort study previously demonstrated this high early mortality rate with linezolid (12%). 11 In addition, another study showed that a slower early clearance of bacterial load, monitored by real-time quantitative polymerase chain reaction, was significantly associated with mortality in VRE BSI. 17 In both studies, the comparator was a bactericidal agent such as daptomycin, and linezolid was associated with a lower rate of bacterial clearance (−0.41 vs. −0.56 Δ log10 copies/mL/day) 10 and higher mortality.
The bacteriostatic properties of linezolid could explain the latter compared to a rapid bactericidal such as daptomycin. However, there is evidence that suggests no relevant differences in clinical outcomes between linezolid and other bactericidal agents.18,19
Moreover, the initiation of linezolid therapy within the first 48 hours of VREf BSI onset showed to be a protective factor with a tendency to decrease mortality in the logistic regression analysis. In the Cox proportional hazard model, early initiation of linezolid treatment reduced mortality by ∼54%. Adverse outcomes due to delay of adequate therapy were shown in a study by Zasowski et al. 6 A breakpoint for adequate therapy was defined at 48 hours; beyond this time, the 30-day mortality had a threefold increase. In the initial treatment of seriously ill patients, the possibility of VRE should be suspected for the initiation of timely treatment with linezolid in standard or individualized doses, 20 as well as another appropriate alternative with bactericidal properties.
We found that persistent bacteremia was a significant factor associated with mortality in patients receiving linezolid therapy. Two retrospective cohort studies of patients treated with linezolid found a median duration of bacteremia of about 3–4 days associated with higher mortality.11,14 These findings suggest that in cases of persistent bacteremia for >48 hours, an alternative antibiotic treatment would be used, as was demonstrated in a study about sequential therapy starting with linezolid and followed by daptomycin with minor mortality in comparison with continuous linezolid (RR, 1.29; 95% CI: 1.03–1.63). 14
The 30-day mortality analysis showed that the patient's underlying conditions, such as the illness severity, were a leading factor associated with mortality when linezolid was given for VREf BSI. Linezolid therapy has shown more 30-day mortality in a retrospective study 11 ; in this study, the mortality was significantly associated in the regression model with APACHE II score (odds ratio [OR] 1.03; 95% CI: 1.02–1.03), and intensive care unit admission (OR 1.31; 95% CI: 1.08–1.60). 11
Conversely, a meta-analysis that included three studies, which adjusted for APACHE ll score, showed significantly lower 30-day all-cause mortality with linezolid therapy. 9 However, the studies included in this meta-analysis had important heterogeneities in the study population with the risk of selection bias. Overall, these findings might suggest that patients severely ill would have high 30-day mortality with linezolid therapy.
Adequate control of infection sources had a trend to be protective in the logistic regression analysis of this study. However, this finding was not observed in retrospective studies with linezolid therapy. In comparative studies of VRE BSI treatment adjusted for this variable, the mortality remained higher with linezolid therapy. 11 In contrast, two retrospective cohort studies showed that the group with infectious disease consultation was associated with more interventions for source control (20% vs. 7%; p = 0.01) and lower mortality (12% vs. 27%; p = 0.007) in enterococcal BSI independent of the antibiotic treatment. In VRE BSI, the group with infectious disease consultation had lower 30-day mortality, which was similar in the group of linezolid (28%) and daptomycin (26%).14,21
Unfortunately, the data about infectious disease consultation in relation to source control of our study were not obtained; however, based on our findings, we believe that aggressive control of infection sources should be sought in severely ill patients on linezolid therapy where no other treatment options are available.
The limitations of this study are its retrospective design and its limited sample size. The nonsurvivor patients were more severely ill with a higher APACHE II score; however, this variable remained significantly associated with 30-day mortality after adjusting by multiple death predictors. Despite these limitations, our findings give essential information about the controversial topic regarding the best selection of treatment for severely ill patients with VRE BSI.
In conclusion, while the best antibiotic treatment for VRE BSI remains controversial, we would consider alternative antibiotics other than linezolid in severely ill patients or with persistent VRE BSI. Well-designed prospective randomized studies on this topic are needed to give these severely ill patients better therapy choices.
Ethical Approval
The institutional review board of the Instituto Nacional de Ciencias Medicas y Nutricion Salvador Zubiran, Mexico, approved this study with the registry code INF-2766-18-18-1. Because of the nature of the study, informed consent was waived.
Footnotes
Acknowledgment
B.A.L.-L. belongs to the program of Maestría y Doctorado en Ciencias Médicas, Odontológicas y de la Salud, UNAM.
Disclosure Statement
We have no conflicts of interest to disclose.
Funding Information
B.A.L.-L. thanks the CONACYT for the grant (CVU, 896545). This study was supported by internal funding.