
Abstract
The burden of antimicrobial resistance (AMR) is considerable in many low- and middle-income countries (LMICs), and it is important to describe the antimicrobial stewardship program (ASP) activities found in these countries and report their impact. Importantly, as these programs target prescribing behavior, the factors influencing prescription of antimicrobials must also be taken into account. This scoping review aimed to (1) describe hospital-based ASP activities, (2) report methods used to measure the impact of ASPs, and (3) explore factors influencing antimicrobial prescribing behavior in LMICs. PubMed was searched from database inception until April 2021. Factors influencing antimicrobial prescribing behavior were canvassed using the Capability-Opportunity-Motivation and Behavior framework. Most of ASP studies in LMICs were predominantly conducted in tertiary care and university-based hospitals. Audit of antimicrobial prescriptions with feedback and restrictive-based strategies was the main reported activity. Total antimicrobial consumption was the main method used to measure the impact of ASPs. Positive outcomes were observed for both clinical and microbiological outcomes; however, these were measured from nonrandomized controlled trials. Dominant factors identified through the behavioral framework were a limited awareness of AMR as a local problem, a perception that overprescription of antimicrobials had limited consequences and was mainly driven by a motivation to help improve patient outcomes. In addition, antimicrobial prescribing practices were largely influenced by existing hierarchy among prescribers. Our scoping review suggests that LMICs need to evaluate antimicrobial appropriateness as an added measure to assess impact. Furthermore, improvements in the access of microbiology and diagnostic facilities and ensuring ASP champions are recruited from senior prescribers will positively influence antimicrobial prescribing behavior, helping improve stewardship of antimicrobials in these countries.
Introduction
The increasing prevalence of antimicrobial resistance (AMR) has been the center of attention globally,1,2 with low- and middle-income countries (LMICs) being significant hotspots.3,4 Both from a clinical and economic perspective, the high burden of AMR is well documented,5,6 with the societal costs associated with AMR being potentially underestimated. 7 Unfortunately, the alarming rise of AMR occurs in an era where there is a limited number of new antimicrobials being developed and approved for clinical use. 8 In the context of LMICs, antimicrobial options may be even more limited because of significant barriers to access. 9 It is, therefore, essential that the efficacy of currently available antimicrobials be maintained as long as possible.
Inappropriate use, including overuse of antimicrobials in humans, is one of the major drivers of accelerating AMR, with hospitals being of primary focus.10,11 The concept of antimicrobial stewardship programs (ASPs) was first mentioned in 199712 and, to date, many guidelines on its implementation in hospitals have been published.13–15 Previous systematic reviews and meta-analyses have documented that hospital-based ASPs could help in optimizing judicious use of antimicrobials.14,16–18 The majority of this evidence have come from well-equipped hospitals, such as tertiary care and university-based hospitals, in high-income countries. The ASP activities undertaken at these hospitals may not be readily translatable to hospitals in the LMIC setting, particularly among resource-challenged hospitals, such as those in rural areas. 19
It should be noted that the mission of any hospital-based ASP is to minimize inappropriate use of antimicrobials, while ensuring optimal patient care.12,13,15,20 This can be sustained through judicious prescribing behavior. Thus, it is important to canvass the range of factors influencing prescription of antimicrobials in daily clinical practice,21,22 which may include factors other than just knowledge and skills.21–24 Other factors, such as interprofessional relationships and hierarchy, may also influence antimicrobial prescribing behavior.21,24 To determine the impact of newly implemented hospital-based ASPs, trends in antimicrobial consumption and appropriateness are often collected and reported by health care facilities.14,15,18,19
The aims of this scoping review were to (1) describe hospital-based ASP activities in LMICs, (2) report methods used to measure the impact of hospital-based ASPs in LMICs, and (3) explore factors associated with antimicrobial prescribing behavior in these countries.
Methods
Our review followed the six-step framework for scoping reviews described by Arksey and O'Malley, 25 with the exception of the optional consultation phase (Step 6).
We addressed the following questions in the scoping review (Step 1):
What activities are reported in hospital-based ASPs implemented among LMICs? What are the methods used to measure the impact of hospital-based ASPs in LMICs? What are the factors influencing antimicrobial prescribing among hospital-based clinicians in LMICs?
Studies conducted in countries classified as low, lower-middle, and upper-middle income, as per the classification system by the Worldbank, 26 were included in this review. The search strategy (Step 2) was undertaken using the PubMed database to identify health-related articles from database inception until April 2021. Extensive key words were used during the search process (Supplementary Table S1) and they were combined by using Boolean operators “AND” and “OR.”
To answer the first and second questions of this scoping review, studies were included (step 3) if they described any activity aimed to optimize antimicrobial prescriptions in the hospital setting and provided information evaluating the impact of these activities. 27 Studies exploring the third question, including knowledge, perceptions, attitudes of hospital-based clinicians toward antimicrobial prescription, and other related aspects of antimicrobial prescription, including AMR and ASP, were deemed to be included in the scoping review if they were conducted exclusively in an LMIC setting. Studies using both/either quantitative (e.g., survey) and/or qualititative (e.g., in-depth interview or focus group discussion) approaches were reviewed in this scoping review.
Studies specifically conducted solely in the outpatient setting of the hospital were excluded from our scoping review. In addition, articles published in languages other than English, Review articles, and Letters to the Editor or Editorials were also excluded from the scoping review.
One author (E.S.) screened all titles and abstracts for potential articles in April 2021 and repeated this step in July 2021 to recheck selections. Upon review of article title and abstract, E.S. reviewed the full-text version according to the inclusion and exclusion criteria. Consultation with another author (M.O.C.) was made if there was uncertainty in selection of potential articles either at the stage of titles and abstracts screening or full-text screening. A “snowballing” search from the reference lists of the final articles to identify additional articles was also conducted.
Data from included studies (step 4 and 5) were extracted and charted using previously defined themes: literature details [e.g., author(s) and year of publication], identity of studies (e.g., country of research sites and number of research sites), characteristics related to study method (e.g., type of survey, interventional vs. observational), variables related to the research questions (e.g., hospital characteristics, duration of observation, and ASP activities), measures to describe the impact of ASP: clinical, microbiological, and antimicrobial measures (e.g., type of consumption measures, defined daily dose [DDD], days of therapy [DOT], antimicrobial-free days, grams or vial of antimicrobial, and antimicrobial prescription prevalence). 27
Identification of factors influencing the antimicrobial prescribing behavior was mainly directed by the Capability-Opportunity-Motivation and Behavior (COM-B) behavioral model. 22 Each component in the COM-B model consists of more than one domain factors influencing the antimicrobial prescriptions (Supplementary Fig. S1). The description of each component in the COM-B model and several domain factors influencing antimicrobial prescriptions in Lorencatto's study (Supplementary Table S2) was used as the guidance to extract data. 21 During the full-text review, new emerging factors, in addition to the listed factors in Lorencatto's study, were identified and classified accordingly. 28 We also used Theoretical Domains Framework as a guidance to further classify each new emerging domain. 28
A descriptive summary was used to present hospital-based ASP activities, the measured impact of such activities, and the factors influencing antimicrobial prescribing behavior. Tables and charts were used to summarize findings where applicable.
Results
The database search yielded 1,481 records, of which 142 were included for full-text review (Fig. 1). Finally, 65 studies29–93 were included to answer Review Questions 1 and 2, while 37 studies94–130 were used to address Review Question 3. Forty-eight of the 65 included records on hospital-based ASPs were published ≥2015.
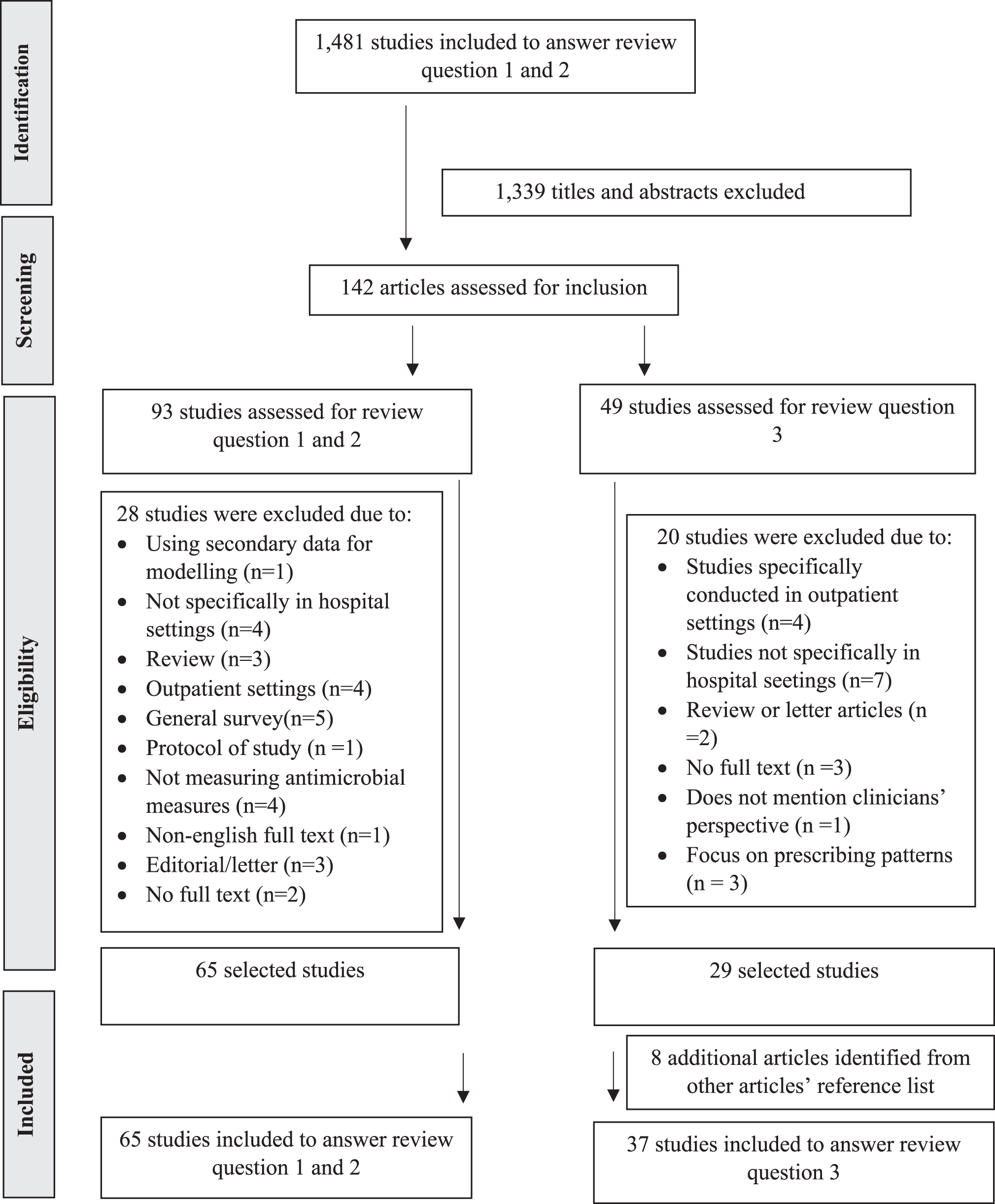
Study selection for the scoping review.
Hospital-based ASP activities in LMICs
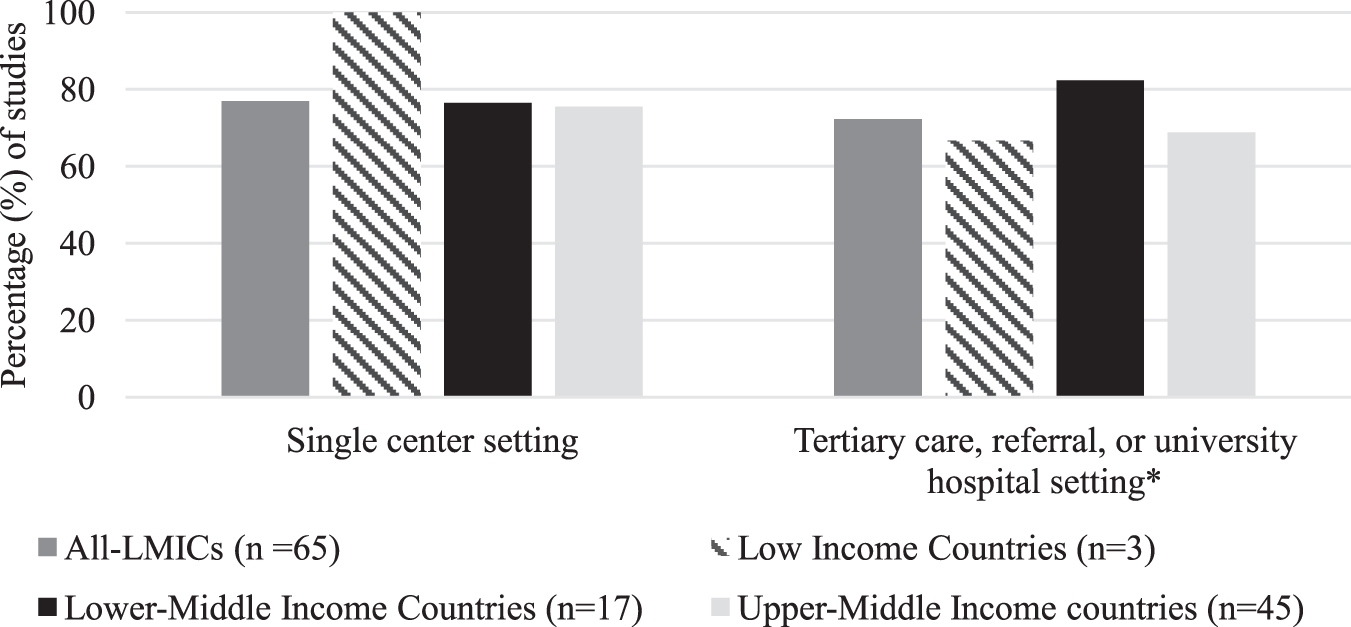
There were 65 records documenting hospital-based ASP activities in LMICs (Table 1).29–93 The majority of these studies (n = 53, 81.5%)29–39,41,43–45,48–50,52–61,63–70,72–76,78,79,81,82,84–90,92,93 used “before-after” or “pre-post” as the study design, while seven studies (10.8%)42,46,47,51,62,89,91 used ecological assessment over certain period of time (duration of assessment ranging from 4 to 7 years). Only one study used an active control in the study and the data were selected nonrandomly. 92 Research on ASPs in LMICs are mostly conducted in either tertiary-care or university-based hospitals, with the majority being single-center studies (Fig. 2). Only three articles, which are from middle-income countries, conducted studies in rural or district hospitals.61,70,75 Two studies were inter-related, in that the second study was a follow-up to the first.57,93
NS indicated that no description of the settings was given in the article; NI indicated that no description was given of the population being studied.
Including: poster, leaflet, and brochures.
The detailed information about pharmacists intervention was not described.
With penalties if targets were not achieved.
Implementing “zero mark up” policy, which means that hospitals were not allowed to get profit from selling medications, including antibiotics.
ICU, intensive care unit; NI, no information; NS, not specified.
Hospital-based ASP activities in LMICs mostly rely on audit of antimicrobial prescriptions with feedback and restrictive-based strategies.29–41,43–51,53–78,81–87,89–91 Two studies mentioned pharmacokinetic monitoring and dosing optimization strategies based on pharmacokinetic/pharmacodynamic (PK/PD) principles as part of their assessment of appropriateness of antimicrobial prescriptions.34,37 In addition to restrictions and/or audit with feedback, several studies from China implemented penalties in hospitals if ASP targets were not achieved.62,73,76,87,91 Implementation of guidelines or treatment protocol was used as the main stewardship activity in five studies,52,75,79,80,88 while dissemination of an antibiogram with education session was implemented as the main stewardship activity in one study. 42
Two ASP projects, one in Nepal and the other in Ethiopia, received support from high-income countries.29,35 In both these studies, health care professionals from high-income countries provided training and regular direct supervision on the audit-feedback sessions, for local health care professionals. These health care professionals also assisted in the development of institutional treatment guidelines.
Use of a multidisciplinary team was an important governance strategy in LMICs,29,30,32,37,39,41,43,51,53,64,65,67–70,73,83 with many studies involving health care professionals with infectious disease (ID) qualifications, such as ID clinicians, or pharmacists with an interest in ID.38–40,43,45,56,58,63,69 “Physician champions” (including senior medical doctors/heads of department) and pharmacists were given the mandate to audit and provide feedback or approval on antimicrobial prescriptions in some of the studies.31,35,36,40,49,52,60,62,66,71,72,74,75,81,82,84,86
Methods used to measure the impact of ASPs
Methods used to evaluate the impact of hospital-based ASPs in LMICs included antimicrobial consumption and associated costs, the appropriateness of antimicrobial prescriptions, clinical outomes, and microbiological outcomes (Table 2). Positive outcomes were documented after ASP implementation, including a decrease in total antimicrobial consumption and costs30–33,35–39,41–46,48–51,62,64,68,73,76,88,92 and improvement in the appropriate use of antimicrobials.34,37,39,63,67,74,77,79,80,82–86
Presented as different measurement, including the rate of antimicrobial prescriptions.
Including the rate of compliance to the guidelines.
!Only presented the trend of tigecycline; the trends of other antimicrobials were not presented.
!!Only presented the trend of carbapenems; the trends of other antimicrobials were not presented.
Days of therapy/1,000 patient-days (DOT/1,000 PDs); bproportion of prescriptions; cdefined daily dose/100 bed-days (DDD/100 BDs); dDDD/1,000 PDs; eDDD; fDDD/100 PDs; gDDD/100 occupied-days; hgrams; ivials; jantibiotic days; kDDD/100-inpatient days.
In addition to measuring the impact on antimicrobial consumption, some studies also assessed clinical outcomes29,32,35,37,40,41,43,47,50–57,65,67–75,80–84,87–89,93 and microbiological outcomes39,42–48,50,56,57,59,62–65,71,73,84,87,91,93 (Fig. 3). Several metrics were used to describe the impact of ASPs on the clinical outcomes, including length of stay (LOS) in the hospital or in a specific unit within a hospital (such as intensive care unit [ICU]),29,34–37,40,43,44,47,50,53,54,56,58,67,69,71–73,75,80–84,87–89,92 in-hospital mortality,29,34,35,37,40,41,43,44,47,50,51,53,55–58,65,68,69,71,73,74,80,82,88,93 hospital-acquired or nosocomial infections,43,47,50,51,53,57,71,73,93 device-associated infections, 59 surgical site infections,54,83,84 Clostridium difficile infections,56,70 Candidemia, 56 hospital readmission,37,41,50,51,56 recurrent infections after discharged, 58 and overall clinical improvements.65,80
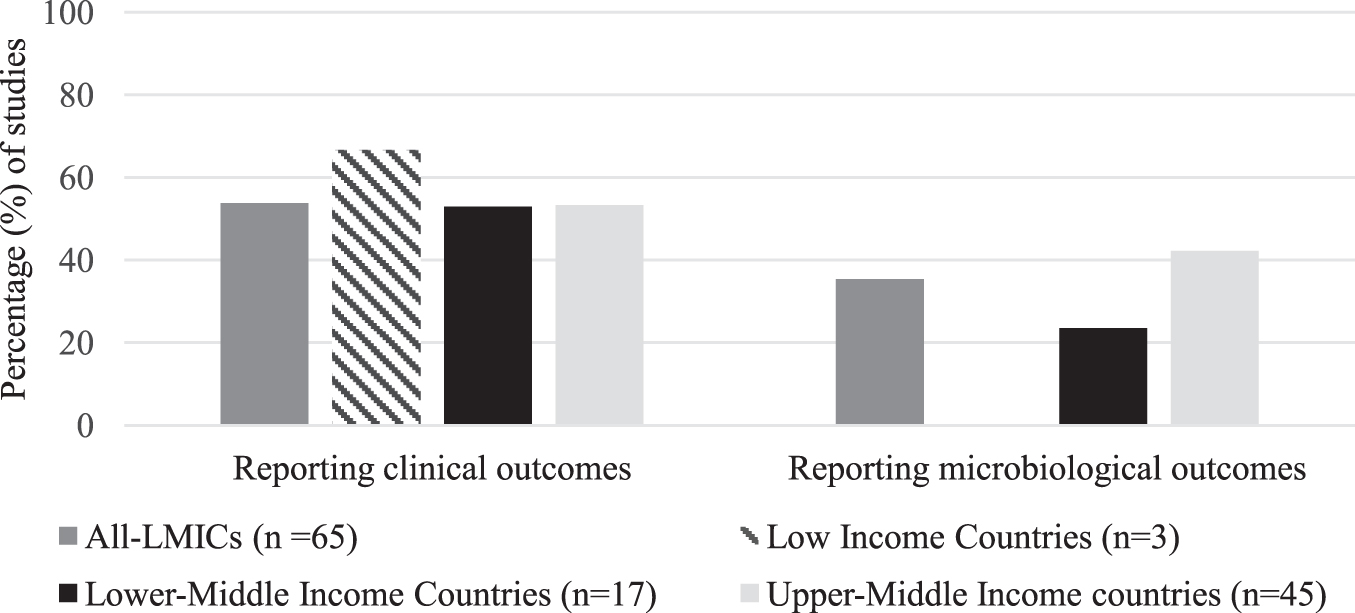
Clinical and microbiological outcomes used to measure the impact of ASPs in LMIC.
In terms of mortality, three studies specifically evaluated infection-related mortality.44,56,93 With regard to microbiological outcomes, few metrics were used, including the type of pathogens being cultured, the resistance patterns of bacteria, prevalence of multidrug, extended drug, or pan-drug resistance.39,42–51,55–59,62–65,71,73,84,87,91,93
Factors influencing antimicrobial prescribing among hospital-based clinicians in LMICs
Thirty-seven studies from 20 LMICs were included in the final descriptive analysis (Table 3).94–130 Factors influencing antimicrobial prescribing behavior were charted using the COM-B framework (Table 4), while examples of supporting data (including quotes from participants in included qualitative studies) for each factor are provided in Supplementary Table S3. In the Capability (C) component, limited awareness toward the problem of resistance intrahospital was frequently cited as the contributing factor of (over) prescribing antimicrobial prescriptions.94–103,106,112,117,120,124,126,127,129
Classification was made according to World Bank's Classification; mixed approach means that the study was conducted by using both qualitative and quantitative approach.
Lower-middle income countries.
Upper-middle income countries.
NI, no information.
The definitions were adapted from Cane et al. 28
AMR, antimicrobial resistance; COM-B, Capability-Opportunity-Motivation and Behavior; LMICs, low- and middle-income countries.
In the Motivation (M) component, hospital-based physicians thought that overprescription of antimicrobials would not result in any harm to the patients.102,110,112 Moreover, antimicrobial prescribing in the hospital was strongly driven by the motivation to help improve patient outcomes and be seen to be proactive in providing patient care.96,105,107,108,110,125
With regard to the Opportunity (O) component, resource factors influencing the prescription of antimicrobials included unavailability of microbiology facilities,96,106,125 unhygienic or unsterilized conditions,100,105,107,125 lack of antimicrobial policy,103,105,126,128 patients' clinical condition at the point of first medical contact,95,100,105–108,125,126 and intake of antimicrobials before hospital admission.101,125 In addition to this, prescribing behavior among other health care colleagues105,108,110,111,124 and hierarchical structure105,108,118 within the medical field were found as factors under the social influences domain (O component).
Discussion
Below, we discuss the gaps in existing literature and also suggest the implications of our findings, which can be of interest to ASP practitioners, researchers, and policy makers in LMICs.
Hospital-based ASP activities in LMICs
Evidence of ASP initiatives could be found in LMICs29–93 and the number of records from LMICs published after the implementation of the Global Action Plan on AMR was higher compared to before its release.29–37,42,46,47,49–56,58,59,62–71,73,75–84,86,87,91–93 The World Health Organization launched the Global Action Plan on AMR in May 2015, which underscored the importance of a “one health” approach to tackle the accelerating AMR problem by involving international and domestic multisectoral stakeholders. 20 This Global Action Plan provided further direction to develop measurable action plans, including in-hospital settings, to combat the threat of AMR. 20
It should be noted that reported ASP activities in LMICs were predominantly from tertiary, referral, or university-based hospitals.29,31–34,37,39–44,46–48,50–60,62,64,65,69,71–73,76–81,83–88,93 This finding should call attention of global stakeholders to the needs of resource-challenged hospitals, such as rural hospitals. It can be speculated that ASP activities are not viewed as core or essential services in many LMIC hospitals, and so it is more likely that better resourced hospitals, such as larger, metropolitan hospitals have the capacity to implement ASPs compared to their rural counterparts. 131
Strengthening this argument is the imbalance ratio between the number of health care professionals and the demand for direct medical services commonly found in resource-challenged hospitals, particularly those located in the rural areas.132–135 A potential confounder to this finding is publication bias, in that, well-resourced hospitals, such as tertiary or university hospitals, are more likely to have the resources to publish findings, especially successfully implemented ASPs.
Nevertheless, there were three studies in rural or district hospital(s) that could be used as references to successfully structure ASP activities in resource-challenged hospitals.61,70,75 The core ASP activity implemented in these studies was found to be audit with feedback. A persuasive-based strategy such as this can be an effective starting point to implement a hospital-based ASP. 14 Furthermore, it allows opportunities to interact with clinicians without restricting what they can prescribe. 136 The three studies noted above involved different health care professionals to provide feedback. For example, the study in a rural community hospital in Georgia involved ID clinicians, 70 while the study in Malaysian district hospitals 75 and Kenyan rural hospitals 61 involved feedback from pharmacists and nurses, respectively.
Feedback may be provided as direct face-to-face communication or as written feedback, 61 with each approach having its advantages depending on the hospital context. Face-to-face communication helps build rapport between clinicians and allows feedback to be expedited, while written feedback may be a more practical alternative in settings where clinicians have a high patient load and may not have time to meet each other and discuss clinical cases.
The availability of a Center of Excellence (CoE) for hospitals in LMICs may offer substantial advantages to enhance the uptake of ASPs. The concept of a CoE in ASP was initiated in the United States in 2017 by the Infectious Diseases Society of America (IDSA).137,138 The main purpose of ASP CoEs is to provide examples of institution with exceptional stewardship practices, of which other hospitals can learn from. 137 Some hospitals in the United States, including community hospitals, were granted status as CoEs for ASP implementation. 138 However, it may be difficult for smaller LMIC hospitals to follow the ASP activities derived from CoEs in high-income countries due resource challenges, differences in health care hierarchy, and interprofessional relationships, as well as prescribing behavior.20,22,23
What might be needed by these LMIC hospitals is how to tailor ASP deployment to local clinical contexts and what activities to prioritize. Moreover, high-income hospital CoEs could serve as training and referral centers, forming partnerships with resource-challenged counterparts.30,35,37,38,41,46 Finally, besides providing an advisory role, the CoEs may further advocate for the urgency of ASP implementation and the resources required to implement ASP to the state or district government. Endorsement and support from local government may help further enhance the diffusion of ASP implementation in LMICs, particularly for those hospitals lacking sufficient resources. 139
Methods to measure the impact of hospital-based ASPs
Evidence from LMICs document that hospital-based ASP activities may impact on antimicrobial, clinical, and microbiology outcomes.29–93 A critique of these methods, however, is necessary to determine whether there is truly an impact on improving inappropriate use of antimicrobial to curtail AMR development, while ensuring optimal care of patients.
The impact of ASPs on antimicrobial consumption was mostly reported as “total antimicrobial consumption.” It should be anticipated, however, that reporting total antimicrobial consumption might not fully capture changes in prescribing trends among antimicrobial classes/agents, which are important contributors to the ongoing development of AMR. 140 Therefore, a more descriptive analysis is required, highlighting prescribing trends in those antimicrobials that may have more of an ecological impact on AMR in the hospital.
Among studies presenting the trends in different antimicrobial classes/agents, it could be seen that the decremental consumption might not always be observed in all types of antimicrobials.30–33,35,36,38,39,41–51,53,55,56,62,63,69 Some of these studies were exclusively conducted among high-risk groups of patients, such as those in the ICU or severe burns, and a decrease in antimicrobial consumption might not be feasible due to the critical nature of their condition, and thus the ongoing need for broad-spectrum antimicrobial therapy.35,42,44,56 Antimicrobials such as amikacin, gentamicin, levofloxacin, moxifloxacin, and meropenem were found to trend downwards after ASP implementation, even though these changes in consumption might not always achieve statistically significant differences compared to the “before” period.31,32,35,36,38,42–51,53,55,56,62,63,68,69,73,76,88
Some studies in LMICs might also indicate the problem of “squeezing the antimicrobial balloon,” which describes an increase in consumption of certain antimicrobials/antimicrobial classes as a consequence of restricting other antimicrobials. One example could be found from a study in Malawi emphasizing that efforts to reduce utilization of 3rd generation cephalosporins saw an observed rise of other broad-spectrum antimicrobials, including ciprofloxacin and amoxicillin-clavulanic acid. 30 Other studies found that carbapenem restriction was followed by an incremental rise in consumption of another antipseudomonal antimicrobial, piperacillin-tazobactam.45,50
Different type of consumption measures were used in the studies from LMICs and the DDD with different denominators (such as 1,000 patient-days or 100 bed-days) were the most frequently used, either as a single metric or combination with other metrics (such as proportion of antimicrobial prescriptions). DDD is “the assumed average maintenance dose per day for a drug used for its main indication in adults.” 141 One potential benefit of using DDD is the ability to benchmark the level of consumption between hospitals, regions, and countries. However, DDD values themselves may not truly represent the actual dose of antimicrobials prescribed in daily clinical practices.142.
It is worth mentioning that, in addition to the problems of overusing antimicrobials, inadequate antimicrobial exposure is listed as another major driver of developing resistant bacteria.143,144 Therefore, if the mission is to tackle the problem of AMR, only measuring consumption may not be the optimal method to ensure judicious use of antimicrobials.
Assessing the appropriateness of therapy, including antimicrobial selection, timing, and route of administration, was of interest among most studies included in this scoping review.35,36,39,40,54,56,60,61,66,67,72,74,75,83,84,86,92 For studies reporting the appropriateness of antimicrobial dosing, assessment was mainly based on reference treatment guidelines,29,32,34,37,57,59,63,69,79,82,87,93 which often assume that standard dosing regimens are applicable to the majority of patients. Of note, however, is that standard dosing may result in variability of exposure in certain patient groups, such as the critically ill, or between different ethnicities.145,146
Dedicated pharmacokinetic monitoring and dosing optimization strategies based on PK/PD principles are recommended as a hospital-based ASP activity by the IDSA and the Society for Healthcare Epidemiology of America, but may not be practical for many LMIC hospitals. 15 Two studies in our scoping review mentioned the use of PK monitoring and PK/PD approaches to assess the appropriateness of antimicrobial treatment.34,37 However, a detailed explanation of how this was undertaken was not clearly described.
With regard to clinical outcomes, LOS and mortality rate were frequently evaluated to measure the impact of ASP among studies from LMICs.29,34–37,40,41,43,44,47,50,51,53–58,65,67–69,71–75,80–84,87–89,92,93 In general, ASP implementation did not negatively impact measured metrics. This information may prove useful when negotiating with the key stakeholders to initiate ASP as current evidence suggests that ASP will not negatively impact patient-centered outcomes. Reporting mortality to emphasize the safety of ASP implementation is indeed important, particularly among patients with severe illness, such as those in the ICU. 147
In LMIC studies that did report associated positive clinical outcomes, it is important to note that these studies adopted either a “before-after,” ecological, or quasi-experimental study methodology without the use of any randomization. Even though these methodologies could be appropriate for studies where randomization is relatively difficult to implement, such as for ASP implementation, these types of studies might not be able to control immeasurable confounding factors, which could only be controlled by randomization. 148 In addition, it is worth acknowledging that most studies did not specifically measure infection-related LOS or mortality.44,56,82,93 This will make any observed association between ASP and positive clinical outcomes difficult to interpret.
Compared to its impact on antimicrobial consumption and clinical outcomes, the impact of hospital-based ASPs on microbiological outcomes was less reported among included studies. Some studies reported the percentage of pathogens susceptible against a single antimicrobial, which may limit the ability to identify the effect of changing prescribing behavior on pathogen resistance profiles.42,44,45,47–49,62,65,84 Reporting the prevalence of multidrug-resistant organisms (MDROs) before and after introduction of a hospital-based ASP might be more appropriate, given this is a central aim of antimicrobial stewardship. 149
Although the prevalence of MDROs was measured in some studies within our scoping review, initial screening of infection or colonization with MDROs was not performed at the time of hospital admission.39,43,50,51,56,58,59,63,64,71,73,91 The inability to differentiate between community- versus hospital-acquired MDROs will limit the ability to measure the true impact of hospital-based ASP activities. Furthermore, these measurements, either single drug or multidrug resistance, could be subjected to the influence of infection prevention and control programs, another important strategy in containing AMR within hospitals.
Factors influencing antimicrobial prescribing among hospital-based clinicians in LMICs
Our structured approach based on the COM-B framework found that antimicrobial prescribing in hospital settings is influenced by overarching internal and external prescriber factors.21,22 The “capability” and “motivation” components could represent internal factors, while the “opportunity” component represents external factors.21,22 Conducting this type of analysis, which is based on a comprehensive framework, allows the full range of behavioral factors to be canvassed.150.
The COM-B framework was successfully used to map influencing factors of antimicrobial prescribing behavior in a previous review by Lorencatto et al., which included four articles from high-income countries. 21 Similar findings were found between our review and the review by Lorencatto et al., including limited awareness toward treatment guidelines and limited competence to choose adequate dosing regimens (both categorized under “capability”); demands of antimicrobial prescriptions from patients and limited diagnostic facilities (both categorized under “opportunity”); and prescribers' wanting to ensure not only the best outcomes for their patients but also their fears toward worsening clinical conditions or complications (both categorized under “motivation”).
Despite these similarities, we found unique interlinkages between C, O, and M components, which characterize driving factors of antimicrobial prescriptions in LMICs (Supplementary Fig. S1). Our review found that prescribers in LMICs may not always consider the implications of antimicrobial prescribing in their local settings in the development of AMR.94–103,106,112,117,120,124,126,127,129 In addition, prescribers consider factors outside their day-to-day antimicrobial prescribing, such as self-medication, prescriptions from unlicensed practitioners, and patient nonadherence, as the main drivers of AMR.95,96,100,101,104,112,115 Antimicrobial intake before hospital admission was found as an important influencing factor,101,125 with antimicrobial self-medication previously listed as a major public health concern in LMICs.151,152
Unsurprisingly perhaps, evidence from LMICs highlighted that the decision to prescribe antimicrobials has been strongly driven by the motivation to save patients and preserve their long-term medical careers.96,105,107,108,110,125 As has previously been acknowledged, it is not always possible to clearly differentiate between infections and noninfections,107–109 and the level of uncertainly is potentially higher in LMICs due to unavailability of facilities to conduct microbiology test, particularly in the rural hospitals. Given this dilemma, there is a propensity to err on the side of caution and prescribed antimicrobials with coverage against a wide variety of organisms.108,125
Other important findings in our scoping review that led to prescribers initiating antimicrobial therapy were in patients with a deteriorating clinical condition at the first medical contact and arriving from environments with poor hygiene (such as those living in low socioeconomic conditions).95,100,105–108,125,126 For these patients, there is often limited access to tertiary health care facilities and this might potentially lead them to try alternative medicines to cure their condition before arriving to hospial. 153 Therefore, it could be understood that patients in LMICs are more often relatively sicker at the first medical encounter compared to those in higher income countries.
Perhaps similar to their counterparts in higher income countries, antimicrobial prescribing in LMICs was influenced by prescriber's colleagues in the hospital.105,108,110,111,124 The perception to “fit in” with peers may represent a culture of collectivism. In sync with this collectivism was the hierarchical structure that is commonly found in the medical profession, especially in teaching hospitals consisting of junior, in-training, and senior medical staff. For junior prescribers, directives from their senior colleagues will mostly dictate antimicrobial prescribing patterns.105,108,118
The pressure on junior doctors to follow these directives may potentially be higher in LMICs due to higher “power distance” culture found commonly in these countries (Supplementary Table S4).105,108,118 Countries with a relatively high score on “power distance” and low score on “individualism” in the Hofstede's cultural domain are usually characterized by a strong hierarchy and sense of “collectivism.” To gain broad acceptance, some hospital-based ASP coordinators in LMICs have recruited senior prescribers as antimicrobial stewardship “champions,” who can help change antimicrobial prescribing patterns to ensure judicious use.
Limitations
Despite the above potential implications from our findings, this scoping review has limitations. First, as we conducted the literature search using one database and only included articles written in English, we may have missed out on including all relevant studies pertaining to our three questions. This is a significant limitation of our scoping review since non-English-speaking LMICs may indeed disseminate their findings locally and in their native language. Furthermore, to ensure a more comprehensive search, we did use an extensive combination of search terms and performed “snowballing” searches from included studies' reference lists.
Second, the data extraction was predominantly undertaken by one author, which may have been subjected to error. To minimize this error, the author used a standard extraction form and carried out a second data extraction a few months later. Third, we could not specifically describe the impact of barriers to access newer broad-spectrum antimicrobials or other essential antimicrobials in LMICs on the implementation of hospital-based ASP activities. Whether the problems of “squeezing the antimicrobial balloon” and unnecessary antimicrobial prescriptions are more frequently found in the hospitals with formidable barrier to access antimicrobials requires further clarifications.
Conclusions
Our scoping review has summarized a range of hospital-based ASP activities implemented in LMICs, with audit and feedback and/or restriction-based strategies being the most common of these. To measure the impact of these activities, studies in LMICs reported different metrics on antimicrobial consumption, as well as clinical and microbiological outcomes, with microbiological outcomes being the least reported. The problems of “squeezing the antimicrobial balloon” and unnecessary antimicrobial prescriptions were observed postimplementation of ASPs in LMIC hospitals. Hospital-based prescribers in LMICs had limited awareness toward the problem of AMR intrahospital and perceived that overprescription of antimicrobials in their practices had limited consequences on the development of resistant pathogens.
Antimicrobial prescriptions were driven largely by a motivation to help improve patient outcomes. Limited microbiology and diagnostic facilities could potentially blunt the effort to survey AMR and reduce overprescription of antimicrobials, respectively. A key influence on the decision to prescribe antimicrobials was the prescribing culture among colleagues and directives from “power holders” within the medical profession, namely senior clinicians. For effective hospital-based ASPs to be sustained in LMICs, further efforts are required to measure its impact on evaluating appropriateness of antimicrobial therapy and to involve senior prescribers to positively influence antimicrobial prescribing behavior.
Footnotes
Acknowledgments
J.A. Roberts would like to acknowledge funding from the Australian National Health and Medical Research Council for a Centre of Research Excellence (APP1099452) and a Practitioner Fellowship (APP1117065), as well as an Advancing Queensland Clinical Fellowship. All other authors: none to declare.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.