
Abstract
An attributing factor to Enterobacterales producing extended-spectrum beta-lactamase (ESBL-E) community spread is human-to-human transmission. This systematic review and meta-analysis aimed to estimate the duration of ESBL-E carriage in the community and the rate of household transmission. Literature search was performed on PubMed, EMBASE, and Scopus. Dose-response meta-analysis was planned to model the proportion of ESBL-E carriers and household transmission over time. Twenty-six studies (n = 2,505 participants) were included. The median carriage duration was 2 months. Approximately 22% (95% confidence interval: 16–28) had persistent carriage after 12 months. Travelers had significantly shorter carriage (median 1–2 months) than discharged hospital patients (median 6 months) at all measured time points. There were insufficient data to robustly meta-analyze household transmission. Nonetheless, five longitudinal studies reported 18.4% to 35.2% of contacts acquired ESBL-E within 4 to 36 months from hospital discharge of index case. Transmission events from travelers to their contacts appeared lower. Travelers with travel-acquired ESBL-E had significantly faster decolonization rate than discharged patients, suggesting that travel-associated import of multidrug-resistant pathogen may have limited contribution to community transmission of ESBL-E. The substantial prevalence of persistent carriers warrant consideration for additional measures to mitigate exposure risk of ESBL-E from discharged patients in the community and from readmitting patients in the hospital.
Introduction
The rapid expansion of Enterobacterales producing extended-spectrum beta-lactamase (ESBL-E) in the community is notable in the last.1,2 Although previously considered as a health care-associated drug-resistant pathogen, a systematic review and meta-analysis by Bezabih et al. found an eightfold increase in global ESBL-E carriage rate in asymptomatic community dwellers from 2003 to 2018. 3 The successful spread of ESBL-E in the community can be attributed to multiple reasons, such as the introduction of highly competent clonal groups with efficient transmission capabilities and survival mechanisms, notably ESBL-producing Escherichia coli ST131.4,5 Other attributing factors include risk factors that facilitate human-to-human transmission of ESBL-E in the community. A Netherlands population-based modeling study reported 60% attributable risk of community-acquired ESBL-producing E. coli to transmission from general community carriers. 6
Risk factors include living in close proximity to an index case or having frequent exposure to high-risk groups, identified as travelers and migrants from endemic countries and discharged hospital patients.6–10 In addition, presence of persistent ESBL-E carriers in the community, who have increased likelihood of recurrent infections,11,12 would lengthen exposure risk in general. Infection with ESBL-E has been associated with higher risk of mortality 13 and, as such, measures to understand and mitigate ESBL-E transmission in the community are vital. These measures should be supported by evidence quantifying ESBL-E human exposure and the extent of persistent carriers in the community, as well as evidence quantifying the extent of within-household transmission. Therefore, this systematic review and meta-analysis aimed to understand the transmission dynamics of ESBL-E by (1) estimating the duration of carriage in community residents and (2) the rate of transmission occurring within household.
Methods
Search strategy
This systematic review and meta-analysis was registered on PROSPERO (CRD42021250896) and followed the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) 14 reporting guidelines (Supplementary Table S1). The literature search was performed in PubMed, Scopus, and EMBASE on April 23, 2021. In general, variant terms for “Enterobacterales,” “ESBL,” “colonization,” and “time factors” were used and combined for the search. Variant terms for “Enterobacterales” included Enterobacteriaceae and MeSH terms of E. coli and Klebsiella pneumoniae, while variant terms for “ESBL” included MeSH terms for beta-lactamases and beta-lactam resistance. Variant terms for “colonization” included carriage, carrier, natural history, and decolonization, while variant terms for “time factors” included duration, rate, median, length, and probability. MeSH terms and Boolean functions were applied where appropriate.
There was no restriction applied to year and language of publication. The detailed search terms used for each database can be found in Supplementary Table S2. A further backward and forward citation search of included articles was performed after to ensure comprehensiveness of the search. All citations were imported into EndNote X9 for duplicates removal followed by exportation to Rayyan for the screening process. 15
Screening and selection criteria
For estimation of ESBL-E carriage duration in the community, the inclusion criteria for studies were (1) study population with ESBL-E colonization or infection, (2) study population residing and followed up in community settings (e.g., general community residents, discharged hospital patients, travelers), (3) follow-up duration of at least 1 month, and (4) follow-up specimens of stool or rectal swabs. The exclusion criteria were (1) intervention studies, (2) data specific to ESBL-E could not be extracted, (3) individuals without ESBL-E carriage included at baseline, (4) follow-up performed with clinical specimens (e.g., urine, blood cultures), and (5) follow-up of patients residing in long-term care facilities or nursing homes.
As a negative trend between natural history of colonization and time was expected, substantial loss to follow-up at time points further from baseline could overestimate the proportion of carriers due to smaller denominator sizes. As such, studies where loss to follow-up of participants were >40% at all measured time points were also excluded from selection.
For estimation of household transmission, the population was defined as household contacts and exposure as the index ESBL-E case. As such, the inclusion criteria for studies were the following: (1) cross-sectional studies where enrolment of index cases with ESBL-E infection or colonization, and carrier state of household contacts was determined at the same time point or (2) longitudinal cohort studies where enrolment of index cases with ESBL-E infection or colonization and follow-up of noncarrier household contacts was performed. The exclusion criteria were the following: (1) any ESBL-E hospital transmission events between index and contact, (2) ESBL-E transmission events between neonates and mothers, and (3) data specific to ESBL-E that could not be extracted.
In cases where studies reported on the same population, the study with the largest sample size was included. Based on these criteria, study screening and selection were performed independently by two reviewers (W.L. and A.M.P.). The abstracts and titles of the search results were first screened and selected before full-text review. The two reviewers resolved selection differences at the end of each screening phase.
Data extraction
For all included studies, general study characteristics such as country, period of enrolment, Enterobacterales species detected, ESBL type detected, definition of baseline, and length of follow-up were collected. Other study population characteristics such as travelers, hospital patients discharged to the community, general community, adults, or children were also documented. For the estimation of ESBL-E carriage duration, the extracted data were number of carriers at baseline, number of carriers at specified time points (at least 1 month from baseline), number of participants followed up at specified time points, median duration of carriage for study cohort, and proportion loss to follow-up from baseline. For the purpose of sensitivity analysis, number of carriers with concordance of ESBL or strain type to initial baseline isolate was also collected.
For estimation of household transmission, the extracted data were number of index cases, number of households enrolled, number of household contacts enrolled, number of colonized household contacts, and number of households where colonized contacts were detected during follow-up. For the purpose of sensitivity analysis, number of colonized contacts or households with concordance of ESBL or strain type to index case was also collected.
Quality assessment
A modified Joanna Briggs Institute quasi-experimental studies assessment tool 16 was used to assess the quality of the included studies based on internal and external validity (Supplementary Table S3). 17 As no comparison to a control group was made based on our study objectives, quality assessment pertaining to comparator group was omitted.
Data analysis
A robust error meta-regression method for dose-response meta-analysis was performed to model the proportion of ESBL-E carriers in the community over time. 18 The robust error meta-regression models were fitted with a restricted cubic spline with four knots as the proportion of ESBL-E carriers over time was expected to be nonlinear. Subgroup analysis was planned to compare between adults and children, and between travelers and discharged hospital patients. Due to the fundamental physiology differences between adults and children, 19 the dynamics of ESBL-E decolonization would likely differ between the two groups. The same applies for the second subgroup analysis, where travelers are likely healthier and asymptomatic with travel-acquired strains compared to sicker hospital patients. 9 The robust error meta-regression method was also planned to estimate proportion of household transmission over time using longitudinal studies.
Sensitivity analysis was also performed to restrict analysis to participants where molecular evidence for concordance of ESBL-E isolates was present. For estimation of ESBL-E carriage duration, concordance was defined by identical ESBL or strain type (using PCR or whole genome sequencing [WGS]) carried by the participant both at baseline and follow-up time points. For estimation of household transmission, concordance was defined by identical ESBL or strain type carried between contact and index case.
Statistical analyses were performed in STATA/SE 16.1 using the remr 20 module. The statistical significance was set at 0.05.
Results
Duration of ESBL-E carriage
A total of 1,503 studies were screened, from which 22 studies were included. The backward and forward citation search further yielded 1,350 studies for screening and an additional 4 studies were included for analysis. The study selection process and exclusion reasons are detailed in Fig. 1. All in all, a total of 26 studies with 2,505 number of participants were included.21–46 There were 14 studies (53.8%) that investigated the duration of ESBL-E carriage in discharged hospital patients, 10 studies (38.5%) in international travelers and 2 studies (7.7%) in the general community.

PRISMA flow diagram for study selection.
Most studies included only adults (n = 13, 56.5%), while only 3 studies restricted their selection to children (13.0%). The follow-up period of the studies ranged from 1 to 36 months. The period of enrolment ranged from 1997 to 2019 and most studies were conducted in the European countries. E. coli and K. pneumoniae were the most frequently detected ESBL-E species. In studies where molecular identification of ESBL type was performed, the CTX-M enzyme was the most commonly detected. The characteristics of these studies are summarized in Table 1.
Summary of Study Characteristics for Estimation of Enterobacterales Producing Extended-Spectrum Beta-Lactamase Carriage Duration
Top two prevalent Enterobacterales species detected in the study cohort.
Follow-up time points were excluded from the final meta-analysis as loss to follow-up >40% from baseline.
ESBL-E, Enterobacterales producing extended-spectrum beta-lactamase.
Although all but three studies had cohorts that were at least 80% representative of the corresponding study population, most of the included studies had low generalizability as inclusion criteria, such as age and type of patients, were applied to sample selection. On the contrary, the internal validity of the included studies was lacking in the reliability of outcome ascertainment, as most studies did not demonstrate concordance of ESBL and strain type across follow-ups (Supplementary Table S4).
The dose-response relationship between proportion of ESBL-E carriage and time is presented in Fig. 2. In general, 50% (confidence interval [95% CI]: 41–59) of the participants lost ESBL-E carriage after 2 months. Twenty-four percent (95% CI: 15–34) of the participants remained as carrier at the 6-months follow-up time point and this proportion of carriers remained relatively stable up till the 18-month time point (20%, 95% CI: 13–27). It was estimated that 17% (95% CI: 5–30) and 13% (95% CI: −12 to 38) of participants remained as persistent carriers 24 and 36 months from baseline, respectively (Supplementary Table S5).

Proportion of ESBL-E carriage over time. ESBL-E, Enterobacterales producing extended-spectrum beta-lactamase.
There were 17 studies, where laboratory testing was performed to confirm concordance of ESBL type (by PCR) or ESBL-E strain (by PCR or WGS) carried by the individual participant across the time points. The proportion of participants estimated to maintain carriage at 6 months was 17% (95% CI: 13–22), this was lower but not significantly different from the main analysis. The same was observed at the 12-month time point (19%, 95% CI: 15–24), suggesting that the prevalence of new ESBL-E infection in the study cohorts was likely low.
A subgroup analysis comparing carriage rate between hospital patients and travelers was performed (Fig. 3). ESBL-E carriage was significantly lower at all studied time points in travelers compared to discharged hospital patients. The median duration of carriage fell before the 2-month time point for travelers, which was much shorter compared to the 6-month time point observed for discharged hospital patients. At the 12-month time point, the proportion of participants that remained ESBL-E carriers was double for hospital patients (32%, 95% CI: 22–42) compared to travelers (15%, 95% CI: 11–19) (Supplementary Table S6). As there were only 3 studies available for children population, there was insufficient data for subgroup comparison of carriage duration between adults and children.
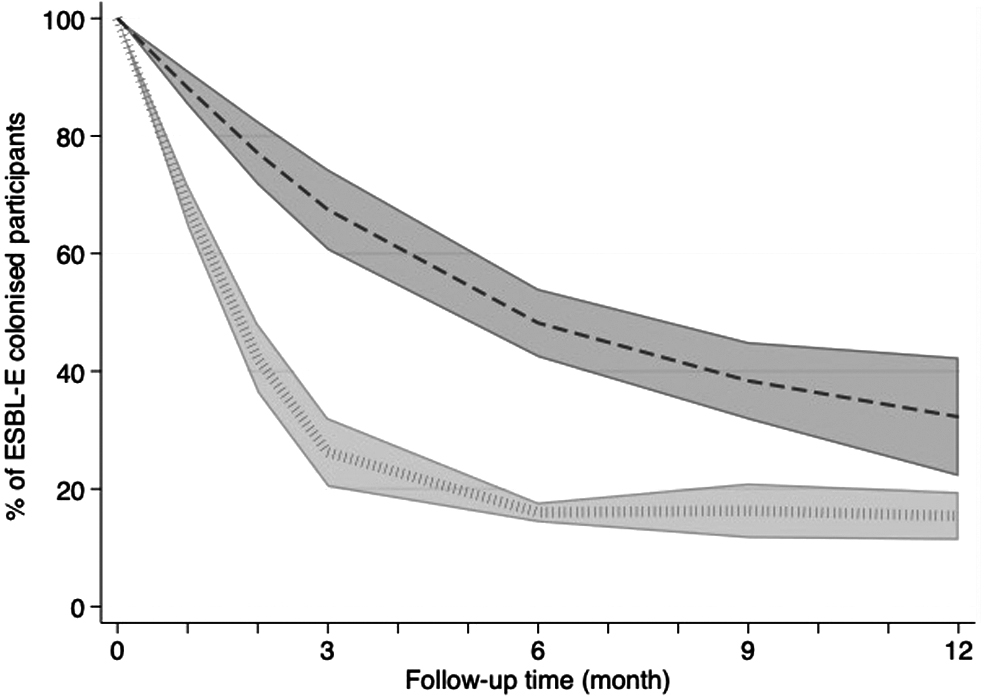
Comparison of ESBL-E carriage duration between discharged hospital patients (dotted line) and travelers (dashed line) over time.
Household transmission
Of the studies screened, there were only 11 studies reporting data on household transmission, including 5 cross-sectional studies and 6 longitudinal studies.22,24,33,35,37,47–52 These also included two studies pertaining to travelers as index and eight studies pertaining to discharged hospital patients as index cases. Due to the limited number of observations available, a reliable dose-response metaregression trend could not be generated. Nonetheless, the summary of study characteristics and individual study results can be found in Table 2. For cross-sectional studies, ∼24% of household contacts were also positive for ESBL-E at the time of index hospital patient diagnosis.49,51
Summary of Study Characteristics and Results of Household Enterobacterales Producing Extended-Spectrum Beta-Lactamase Transmission Rate
UTI, urinary tract infection.
For prospective cohort studies where contacts were initially noncarriers at baseline, ∼18.4% to 35.2% of contacts became carriers within 4 to 36 months range of follow-up time from discharge of index hospital patient.22,35,37,47,48 Transmission of ESBL-E from index patient to contact was assumed to have happened in ∼18.3% to 42.1% of enrolled households in this period. On the contrary, ESBL-E transmission from return travelers to household contacts appeared lower, with only 18.2% and 7.7% of contacts acquiring carriage after 6 and 12 months, respectively, from traveler's return.22,24
Discussion
In general, the median duration of ESBL-E carriage was ∼2 months, with an estimated 17% of participants having persistent carriage even after 2 years. Interestingly, travelers had shorter duration of travel-acquired ESBL-E carriage compared to discharged hospital patients, with a median decolonization time of <2 months in the former group compared to 6 months in the latter. There was insufficient data to estimate the pooled rate of ESBL-E transmission occurring within households. Nonetheless, between 7.7% and 35.2% of household contacts were reported to be new carriers within 36 months from baseline. Household transmission of ESBL-E was observed in 18.3% to 50.0% of households.
All the travel-related studies included in this systematic review and meta-analysis had the highest prevalence of participants returning from Asian countries. This is consistent with a previous systematic review and meta-analysis that reported South Asia as the highest multidrug-resistant Enterobacterales acquisition destination. 53 The results pertaining to traveler's carriage are, hence, highly reflective of travel acquisition from Asia region. This systematic review and meta-analysis reported a faster decolonization rate in travel-acquired ESBL-E compared to discharged hospital patients residing in the community. There are several postulations for this observation, including travelers being healthier in general and likely with fewer exposures to health care-associated risk factors, such as nosocomial infection and further antimicrobial intake, for acquiring or maintaining carriage of ESBL-E.
Although travel-acquired importation of multidrug-resistance pathogen has been a public health concern in recent years, the fast decolonization rate of travelers reported here suggests that importation of ESBL-E may not be as major of a concern for community spread. Compared to discharged patients from hospital, the results suggest that discharged patients impose a longer risk of ESBL-E exposure in the community. The substantial prevalence of persistent carriers would also have implications for introduction of ESBL-E into hospital settings for readmitted patients. It would appear that hospital surveillance and infection control practices are warranted for patients with the history of ESBL-E.
The results in this systematic review and meta-analysis were consistent with a previous systematic review and meta-analysis performed by Bar-Yoseph et al., 54 which also observed a faster decolonizing rate in travelers compared to hospital patients. However, we reported lower carrier rates at all time points (3, 6, 12 months) except for the 1-month time point. The faster decolonizing rates reported in our study can be attributed to differences in meta-analysis statistical methods performed and slight differences in the inclusion and exclusion criteria for selection of studies. In addition, while the previous systematic review and meta-analysis reported a limitation where molecular evidence for persistent carriage was not demonstrated in most studies, our systematic review and meta-analysis were able to extract sufficient data on this aspect to perform a sensitivity analysis.
We have shown that proportion of ESBL-E carriers with concordance of ESBL or strain type across studied time points were lower but not significantly different from the main analysis. This suggests that the included study cohorts were likely not influenced by new ESBL-E infections or exposures. This sensitivity analysis also allowed for a more valid representation of intraindividual duration of ESBL-E carriage with concordance of ESBL or strain type of isolates ensured over the follow-up period.
There were some limitations to this systematic review and meta-analysis. First, there were insufficient data on household transmission for robust error metaregression to be performed robustly. Although individual study results could only be briefly summarized, studies were highly heterogenous with regard to study design, baseline definition, and follow-up length. There is a gap for future longitudinal studies investigating household transmission between index cases and noncarrier household contacts to quantify transmission occurring within household settings. Second, although selection criteria were in place to remove influence of factors that could alter intestinal carriage, there was a small subset of participants included in this meta-analysis that were readmitted or had antibiotic intake during the follow-up period. This is unavoidable, as it would be unethical for individual study to restrict clinical treatment to participants. As such, the carriage duration reported here may be biased by these clinical exposures.
Third, most studies assume ESBL-E eradication in participant after a negative culture was obtained and participant was analyzed as noncarrier from thereon. This assumption could be erroneous due to gaps in sample collection and laboratory detection techniques. For instance, two of our included studies have observed participants that returned a positive culture in further follow-up after testing negative.36,44 As such, the carriage duration reported here may be underestimated by studies that assume noncarrier status in participants after a single negative culture. Next, results specific to travelers may be largely generalizable to ESBL-E acquired in Asian countries only. We also could not elucidate the relationship between duration of travel and duration of ESBL-E carriage due to limited and heterogenous data.
Finally, there was variability in the definition of baseline from studies estimating the carriage duration of ESBL-E in discharged hospital patients. Half of the included studies defined its baseline as point of positive culture result and as such, results on community carriage duration specific to discharged hospital patients may have been slightly inflated by their length of hospital stay.
Nonetheless, this is the first systematic review and meta-analysis to model duration of ESBL-E carriage over time as a continuum. 18 This produces a more precise estimation of the relationship between carriage and time. It was interesting to note that the loss of carrier state was exponential in the first 3 months before stabilizing after 6 months. Our results also included few follow-up time points beyond 12 months, where it was estimated that ∼22% of people could remain as persistent carriers. The results can be better validated with future longitudinal studies of similar design and long follow-up length. The substantial prevalence of persistent carriers would have implications for transmission of ESBL-E in the community and public health measures should be considered to mitigate this risk, especially from discharged hospital carriers.
Conclusion
In conclusion, the median duration of ESBL-E carriage was ∼2 months from baseline. Nonetheless, ∼22% of carriers could maintain persistent carriage even after 12 months. Travelers with travel-acquired ESBL-E had significantly faster decolonization rate (median duration: before 2 months) compared to discharged hospital patients (median duration: 6 months). The longer carrier status of discharged patients may impose higher exposure risk of ESBL-E in the community. Although travel-associated multidrug-resistance acquisition has been a major concern for public health, this study showed that travelers had short carrier status for ESBL-E and may have limited contribution to community transmission. Since there were limited data to estimate the rate of household transmission, additional prospective studies are warranted to investigate this trend.
Footnotes
Acknowledgments
The study authors acknowledge and thank librarian Lars Eriksson for his help in building the search strategy.
Authors' Contributions
D.L.P., P.N.A.H., L.F.-K., and W.L. conceived the aim of this systematic review and meta-analysis. W.L. performed the database search. W.L. and A.M.P. were responsible for study screening and selection. W.L. did the data extraction and quality assessment. W.L. and L.F.-K. performed the statistical analysis. W.L. drafted the article. All authors reviewed and provided inputs for the article. All authors approved the final version of the article.
Disclosure Statement
D.L.P. has received research grants from Merck, Pfizer, and Shionogi outside of the submitted work. He has also received personal fees from Merck, Pfizer, Shionogi, Shionogi, Lysovant, The Medicines Company, Entasis, VenatoRx, Biomerieux, and Accelerate. P.N.A.H. has received research grants from Merck, Sharpe and Dohme (MSD), Sandoz, and Shionogi Ltd., outside of the submitted work, as well as personal fees from Pfizer and Sandoz. All other authors have none to declare.
Funding Information
W.L. and A.M.P. are receiving scholarship support from University of Queensland for Doctor of Philosophy candidature. L.F.-K. was supported by Australian National Health and Medical Research Council Early Career Fellowships (APP1158469). P.N.A.H. is receiving support from NHMRC Early Career Fellowship (GNT1157530) and D.L.P. from an NHMRC Investigator Grant.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.