
Abstract
Background:
Multidrug-resistant (MDR) bacteremia is a serious health care-associated infection with significant morbidity and excess hospitalization costs. Our aim is to study the association between incidences of MDR bacteremia, antibiotic consumption, and infection control measures in a hospital from 2013 to 2018.
Methods:
We analyzed the following indices: (1) incidence of bacteremia (carbapenem-resistant Acinetobacter baumanii, Pseudomonas aeruginosa, and Klebsiella pneumoniae, methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococci); (2) use of antibiotics; (3) consumption of disinfectant solutions for hand hygiene; and (4) isolation rates of MDR carrier patients.
Findings:
The use of advanced antibiotics (p = 0.001) and carbapenems (p = 0.008) decreased significantly in all hospital departments but the incidence of total MDR bacteremia did not change significantly. Increased use of hand disinfectant solutions was statistically associated with decreased incidence of total MDR bacteremia (incidence rate ratio [IRR]: 0.94, confidence interval [95% CI]: 0.90–0.99, p: 0.020) in all hospital. Also, increased isolation rates of MDR carrier patients 2 months before correlated with decreased incidence of bacteremia due to carbapenem-resistant gram-negative pathogens (IRR: 0.35, 95% CI: 0.18–0.66, p: 0.001) in adults intensive care unit.
Conclusion:
In our hospital, hand hygiene and isolation of MDR carrier patients controlled MDR bacteremia.
Introduction
Bacterial bloodstream infections (BSI) due to nosocomial multidrug-resistant (MDR) pathogens have a serious effect on hospital length of stay, deaths, and health care costs comprising ∼30–50% of all BSI cases in high-income countries. 1 The six leading MDR pathogens associated with a fatal outcome (Escherichia coli, followed by Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa) were responsible for 929,000 deaths attributable to antimicrobial resistance in 2019 globally. 2
According to two-point prevalence surveys conducted in 2016 and 2017 for studying health care-associated infections in acute-care hospitals across Europe, 6.2% of isolates were carbapenem-resistant Enterobacteriaceae, while in Greece this percentage reached 43.7%. 3 Also, a surveillance survey conducted in acute-care hospitals in Greece showed a mean incidence of carbapenem-resistant pathogens of 0.48 per 1,000 patient-days in acute-care hospitals and a crude 28-day mortality rate of 34.4%, which indicates a significant public health problem. 4
The association between antibiotic consumption and MDR pathogens has been investigated the last decade during antimicrobial stewardship programs (ASP), in observational or interrupted time-series studies.5–8 Also, clinical and economic outcomes were evaluated from the implementation of hospital-based ASPs. 9 Because the abuse of antimicrobial agents in acute-care settings can stimulate the emergence and prevalence of MDR pathogens, interventions to improve antibiotic prescribing practices for hospital inpatients have been largely applied in the past decade.10–13
The current study aimed to evaluate specific infection control measures and outcomes in association with the incidence of MDR bacteremia in patients hospitalized in a hospital in Athens during the implementation of an ASP.
Materials and Methods
Study design
The study was conducted prospectively in a 300-bed tertiary-care hospital in Athens, Greece, during a six-year period (January 2013 through December 2018). The hospital has (1) one Adults Clinic (with Internal Medicine, Surgery, Hematology, and Oncology Departments and one intensive care unit [ICU]); (2) one Obstetrics and Gynecology Clinic (with one neonatal ICU); and (3) one Pediatrics Clinic (with one pediatric ICU).
Interventions
The following interventions were applied during the 6-year study period: (1) surveillance of carbapenem-resistant P. aeruginosa, Acinetobacter baumanii, and K. pneumoniae, methicillin-resistant S. aureus (MRSA), and vancomycin-resistant Enterococci (VRE); (2) formulary restriction and preauthorization for advanced antibiotics; (3) promotion of hand hygiene; and (4) screening and isolation of MDR carrier patients. The program was evaluated on a monthly basis.
Outcomes
The following outcomes were estimated on a monthly basis: (1) incidence of bacteremia (cases/1,000 patient-days); (2) antibiotic consumption (defined daily doses [DDDs]/100 patient-days); and (3) consumption of disinfectant solutions for hand hygiene (L/1,000 patient-days). Data were collected prospectively.
Detection of bacteremia and microbial resistance
Bacteremia was detected through Gram stains and blood cultures. The automated VITEK 2 system (Biomerieux) was used for the isolation, identification, and antibiotic susceptibility testing. The CLSI breakpoints were used. The assay (Kirby–Bauer test, MIC semiautomated testing, E-test) used to determine antibiotic susceptibility was recorded.
Definitions
Bacteremia was defined as a laboratory-confirmed bloodstream infection, either primary (not related to an infection at another body site) or secondary (thought to be seeded from a site-specific infection at another body site). 14 A new episode of bacteremia due to a different pathogen strain or due to the same pathogen strain but with different phenotype of resistance within a month period was considered a new episode of bacteremia. The incidence of total bacteremia derives from the sum of total Gram-positive and Gram-negative bacteremia. The incidence of total resistant Gram-positive bacteremia consists of the sum of the incidence of MRSA and VRE bacteremia. The incidence of total carbapenem-resistant Gram-negative bacteremia is the sum of the incidence of carbapenem-resistant P. aeruginosa, A. baumanii, and K. pneumoniae bacteremia.
The 2018 version of the World Health Organization Anatomical Therapeutic Chemical/DDD index was used to present data on antibiotic consumption (Nos. of DDDs per 100 patient-days). The following antibiotics were defined as advanced antibiotics: carbapenems, colistin, tigecycline, fosfomycin, linezolid, daptomycin, ceftaroline, ceftazidime-avibactam, and ceftolozane-tazobactam. For hand hygiene, the following were used: scrub disinfectant solutions with chlorhexidine, alcohol 70% disinfectant solutions with chlorhexidine, and/or simple soap. Percentage of isolated patients per 100 admissions was used for estimating isolation rate of MDR carrier patients.
Statistical analysis
We investigated time trends in the intervention and outcome variables during the 6-year study period. Time since January 2013 (beginning of the study) was the independent variable in the regression models and entered through appropriate restricted cubic splines. In each case, the dependent variable was the variable under investigation (intervention or outcome). Fourier series terms of time (first and second order) were also entered in the models to capture potential seasonality effects. In all cases, standard errors and corresponding confidence intervals (95% CIs) were estimated using the robust (sandwich) variance estimator to adjust potential violations of models' assumptions. Estimated values for beginning and end of the study period and corresponding 95% CIs were estimated through a simplification of the models. Spline time terms were replaced by a single linear time trend or two piecewise linear terms to capture average long-term trend.
A linear regression model was applied for consumption of antibiotics and consumption of disinfectants. Poisson regression models were used with number of cases as dependent variable and the appropriate number of patient-days as an offset after logarithmic transformation, for cases where the outcome of interest was bacteremia rates. Binomial regression models were used with number of cases as dependent variable and the appropriate number of hospitalizations as binomial denominator, for cases in which the percentage over total number of hospitalizations was the outcome of interest (isolations). We introduced appropriate independent variables into the models to investigate the associations between outcomes and interventions.
The effects of the independent variables were initially tested separately for current (“month 0”) and lagged values (months -1, -2 and -3). If the effects were statistically significant (p < 0.05) or indicative (0.05 <p<0.10) for more than one case (e.g., in month 0 and in month-1) and association direction was the same (e.g., positive for both), average value was used as independent variable. In cases where direction of the association was different (e.g., positive for “month 0” and negative for “month-1”), results of the respective models are presented separately. p-values have not been adjusted for multiple testing. The Stata version 14.2 (Stata Corp., TX) was used for analyses.
Ethics
The study was approved by the Ethics Committees of the National and Kapodistrian University of Athens (Approval No: 1718016673-25/01/2018) and Athens Medical Center (Approval No: ΚΜ140678-26/07/2017).
Results
From January 2013 through December 2018, 95,228 admissions were recorded in the hospital. Regarding bacteremia, 1,671 (7.58%) cultures were positive out of a total number of 22,044 blood cultures. The incidence of bacteremia was as follows: 4.10/1,000 patient-days for total bacteremia, 0.04/1,000 patient-days for total resistant Gram-positive bacteremia, and 0.24/1,000 patient-days for total carbapenem-resistant Gram-negative bacteremia. The incidences of MDR bacteremia are displayed in Figs. 1 and 2.
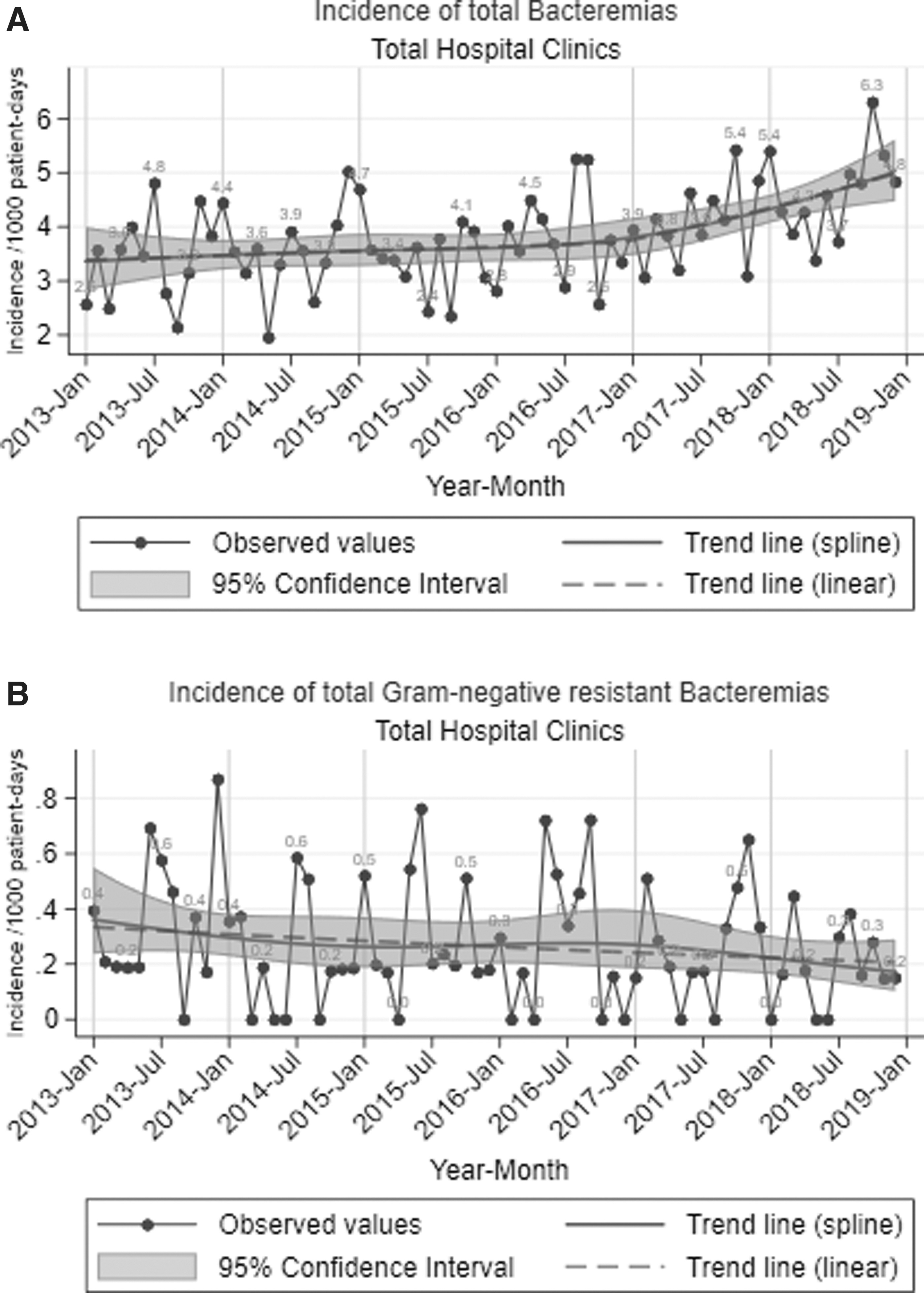
Observed values and estimated time trends for bacteremia in a hospital, January 2013 to December 2018:

Observed values and estimated time trends for bacteremia in an adult's ICU, January 2013 to December 2018:
Table 1 depicts time trends of MDR bacteremia during the entire study period. The incidence of total bacteremia significantly increased in all Hospital Clinics and Departments (p = <0.001), in Adults Clinic (p = 0.001) and Departments (p = 0.004), and in Adults ICU (p = <0.001), which is consistent with the increased number of blood cultures and hospital admissions during the 6-year study period (data not shown). However, there was no significant change in the incidence of total MDR bacteremia. For carbapenem-resistant bacteria, the trend was stable for A. baumanii and K. pneumoniae, but decreased significantly for P. aeruginosa in all Hospital Clinics and Departments, and in Adults Clinic and Departments (p = 0.027, 0.042, 0.031, and 0.051, respectively).
Time Trend of Multidrug-Resistant Bacteremia Per 1,000 Patient-Days in a Hospital, January 2013 to December 2018
All estimates derived from Poisson regression models with robust standard errors, seasonality terms and linear or piecewise linear long-term trend:
log(N) = β0 + β1t− + β2t+ + β3 × sin(2πt/12) + β4 × cos(2πt/12) + β5 × sin(4πt/12) + β6 × cos(4πt/12) + log(patient-days) with N being the number of cases and t being time since study start in months (t− and t+ piecewise linear time terms; when piecewise linear long-term trend was not required a single time term was used). % Relative changes/year derived as [exp(12 × β1,2) − 1] × 100%.
CI, confidence interval; CR, carbapenem-resistant; EVEP, estimated value end period; EVSP, estimated value start period; ICU, intensive care unit; MDR, multidrug-resistant; N/A, not applicable.
In Adults ICU, no significant change was noted regarding total carbapenem-resistant Gram-negative pathogens. A linear model was not applied for resistant Gram-positive pathogens given the fact that the respective incidence was very low and stable during the 6-year period.
Time trends of antibiotic consumption are shown in Table 2. A statistically significant reduction was observed for all antibiotics and nonadvanced antibiotics in total hospital departments and in separate clinics and departments (p = <0.001 for all comparisons). The consumption of advanced antibiotics and carbapenems only decreased significantly in total hospital (p = 0.001 and 0.008, respectively). In contrast, consumption of all antibiotics, nonadvanced antibiotics, and carbapenems in particular increased significantly in Adults ICU (p = <0.001, 0.007, and 0.025, respectively).
Time Trend of Antibiotic Consumption (Defined Daily Doses/100 Patient-Days) in a Hospital, January 2013 to December 2018
All estimates derived from linear regression models with robust standard errors, seasonality terms and piecewise linear long-term trend:
E[Y] = β0 + β1t− + β2t+ + β3 × sin(2πt/12) + β4 × cos(2πt/12) + β5 × sin(4πt/12) + β6 × cos(4πt/12) with E[Y] being the expected consumption value and t being time since study start in months (t− and t+ piecewise linear time terms). Absolute changes/year derived as β1,2 × 12.
DDD, defined daily dose.
Table 3 shows the temporal 6-year trend of consumption of disinfectant solutions for hand hygiene. The use of alcohol disinfectant solutions increased significantly in all Hospital Clinics and Departments p = <0.001) and in Adults Clinic Departments separately (p = <0.001). Similarly, the consumption of all hand disinfectant solutions increased significantly in all Hospital Clinics and Departments (p = <0.001), Adults Clinic (p = <0.001), and Adults ICU (p = 0.001). Finally, there was a significant increase in the consumption of scrub disinfectant solutions in Adults Clinic Departments and ICU (p = 0.004 and 0.001, respectively).
Time Trend of Consumption of Hand Disinfectant Solutions (L/1,000 Patient-Days) in a Hospital, January 2013 to December 2018
All estimates derived from linear regression models with robust standard errors, seasonality terms and piecewise linear long-term trend:
E[Y] = β0 + β1t− + β2t+ + β3 × sin(2πt/12) + β4 × cos(2πt/12) + β5 × sin(4πt/12) + β6 × cos(4πt/12) with E[Y] being the expected consumption value and t being time since study start in months (t− and t+ piecewise linear time terms). Absolute changes/year derived as β1,2 × 12.
Table 4 shows the 6-year time trend of isolation rates of MDR carrier patients per 100 admissions. The isolation rate of MDR carrier patients increased significantly in Total Hospital Departments and in Adults ICU (p = <0.001). In Adults Clinic a significant increase was observed until April 2015 and in Adults Departments until February 2015 (p < 0.001 for both comparisons).
Time Trend of % Isolations Per 100 Hospital Admissions Over Time in a Hospital, January 2013 to December 2018
All estimates derived from binomial logistic regression models with robust standard errors, seasonality terms and piecewise linear long-term trend: logit(π) = β0 + β1t− + β2t+ + β3 × sin(2πt/12) + β4 × cos(2πt/12) + β5 × sin(4πt/12) + β6 × cos(4πt/12) with π being the probability of isolation and t being time since study start in months (t− and t+ piecewise linear time terms). % Relative changes/year derived as [exp(12 × β1,2) − 1] × 100%.
Table 5 shows the correlation between total bacteremia and antibiotic consumption. In total Hospital Clinics, the consumption of carbapenems (p = <0.001) and advanced antibiotics (p = 0.010) significantly correlated with increased incidence of total bacteremia. In Adults Clinic, the consumption of fosfomycin, ceftolozane-tazobactam, and all antibiotics significantly correlated with increased incidence of total bacteremia (p = 0.031, 0.50, and 0.025, respectively). In Adults ICU, the consumption of fourth generation cephalosporins (p = 0.047), monobactams (p = 0.005), colistin (p = <0.001), linezolid (the current month, p = 0.037), fosfomycin (p = 0.004), advanced antibiotics (p = <0.001), and all antibiotics (p = 0.035) significantly correlated with increased incidence of total bacteremia. Interestingly, the consumption of linezolid 3 months before (p = 0.013) and nonadvanced antibiotics (p = 0.045) significantly correlated with decreased incidence of total bacteremia.
Incidence of Total Bacteremia and Correlation with Consumption of Antibiotics, January 2013 to December 2018
Symbol ◊ denotes whether the association refers to the current month consumption (month 0) value, lagged values (months -1, -2, -3) or averaged values over >1 month. IRR refer to increases in consumption denoted in column labeled “per (n) DDD.”
All estimates derived from Poisson regression models with robust standard errors, seasonality effects and spline terms of time: log(N) = β0 + β1V + β2S1(t) + β3S2(t) + β4S3(t) + β5 × sin(2πt/12) + β6 × cos(2πt/12) + β7 × sin(4πt/12) + β8 × cos(4πt/12)+log(patient-days) with N being the number of cases, t being time since study start in months, S(t) being spline terms of t and V referring to the current month covariate (month 0) value, lagged values (months -1, -2, -3) or averaged values over >1 month. IRRs derived as [exp(n × β1) − 1] × 100% with n given in column labeled “per (n) DDD.”
IRR, incidence rate ratio; ns, not-significant.
Table 6 shows the correlation between total carbapenem-resistant Gram-negative bacteremia and antibiotic consumption. The pattern of correlation is repeated in total Hospital Clinics and Departments, and in Adults Clinic and Departments, and Adults ICU. Antibiotics used to treat carbapenem-resistant Gram-negative infections, such as monobactams, carbapenems, colistin, tigecycline, fosfomycin, and all advanced antibiotics, are correlated with increased incidence of bacteremia due to carbapenem-resistant Gram-negative pathogens.
Incidence of Total Carbapenem-Resistant Gram-Negative Bacteremia and Correlation with Consumption of Antibiotics, January 2013 to December 2018
Symbol ◊ denotes whether the association refers to the current month consumption (month 0) value, lagged values (months -1, -2, -3) or averaged values over >1 month. IRRs refer to increases in consumption denoted in column labeled “per (n) DDD.”
All estimates derived from Poisson regression models with robust standard errors, seasonality effects and spline terms of time: log(N) = β0 + β1V + β2S1(t) + β3S2(t) + β4S3(t) + β5 × sin(2πt/12) + β6 × cos(2πt/12) + β7 × sin(4πt/12) + β8 × cos(4πt/12) + log(patient-days) with N being the number of cases, t being time since study start in months, S(t) being spline terms of t and V referring to the current month covariate (month 0) value, lagged values (months -1, -2, -3) or averaged values over >1 month. IRRs derived as [exp(n × β1) − 1] × 100% with n given in column labeled “per (n) DDD.”
CR, carbapenem-resistant.
Table 7 shows the correlation between bacteremia and infection control interventions. An increase in the consumption of scrub disinfectant solution the current month and 1 or 2 months before significantly correlated with decreased incidence of total bacteremia in all Hospital Departments (p = 0.011). In addition, an increase in the consumption of all hand disinfectant solutions the past month correlated with reduced incidence of total bacteremia (p = 0.020). Furthermore, every increase of isolation of patients with MDR pathogens in Adults Clinic and Departments 3 months before correlated with increased incidence of total bacteremia (p = 0.001 and <0.001, respectively).
Incidence of Different Bacteremia and Correlation with Infection Control Interventions, January 2013 to December 2018
Symbol ◊ denotes whether the association refers to the current month (month 0) value, lagged values (months -1, -2, -3) or averaged values over >1 month. IRRs refer to increases denoted in column labeled “per (n) units.”
All estimates derived from Poisson regression models with robust standard errors, seasonality effects and spline terms of time: log(N) = β0 + β1V + β2S1(t) + β3S2(t) + β4S3(t) + β5 × sin(2πt/12) + β6 × cos(2πt/12) + β7 × sin(4πt/12) + β8 × cos(4πt/12) + log(patient-days) with N being the number of cases, t being time since study start in months, S(t) being spline terms of t and V referring to the current month covariate (month 0) value, lagged values (months -1, -2, -3) or averaged values over >1 month. IRRs derived as exp(n × β1) with n given in column labeled “per (n).”
In addition, every increase in isolations of patients with and MDR pathogens in total Hospital and Adults Clinic Departments 2 months before correlated with increased incidence of total carbapenem-resistant Gram-negative bacteremia (p = <0.001 and 0.009, respectively). Interestingly, in Adults ICU, every increase in isolation of patients with MDR pathogens the current month correlated with increased incidence of total bacteremia and total carbapenem-resistant Gram-negative bacteremia (p = 0.020 and <0.001, respectively), while 2 months before correlated with reduced incidence of carbapenem-resistant Gram-negative bacteremia (p = 0.001).
Discussion
In this observational study, we aimed to assess the association between infection control interventions and outcomes with different MDR bacteremia in a 300-bed tertiary-care hospital in Athens, Greece. Interventions have been included in routine clinical practice with institutional support and consisted of surveillance of antibiotic resistance, preauthorization for prescribing advanced antibiotics, screening and isolation of MDR carrier patients, and promotion of hand hygiene. Of these interventions, isolation of MDR carrier patients and hand hygiene have contributed to reduce the incidence of carbapenem-resistant pathogens during the study period.
A variety of antibiotic resistance surveillance systems have been described in the literature with different characteristics.15,16 ASPs have been implemented to optimize the use of antimicrobial agents in health care settings, improve patient outcomes, and reduce antibiotic-associated adverse events, as well as the selection pressure associated with antimicrobial use. 17 In our hospital, an ASP began in 2013, and since its implementation, the incidence of hospital-acquired infection significantly decreased, 18 including Clostidioides difficile infections. 19
Recent studies posed questions regarding the sustained impact of ASP not only in antibiotic resistance but also in economic and ecological indices, reducing costs, and mortality of hospital-acquired MDR bloodstream infections.20–22 In our study, we focused on providing quantitative data on antimicrobial consumption and clinical outcomes in a center with an active ongoing institutional and education-based ASP. The most significant interventions were the increase in the consumption of hand disinfectant solutions, which indicates increasing adherence to hand hygiene, and increase isolation of MDR carrier patients. In addition, the most important outcome was the statistically significant reduction in total hospital of all antibiotics, including carbapenems. In Adults Clinic, the reduction was significant for nonadvanced antibiotics, while in Adults ICU, the intervention of restricted formulary did not have any downstream effect.
The impact of these 6-year interventions and outcomes on the incidence of MDR bacteremia resulted in a decreasing trend, although not statistically significant. The incidence of total bacteremia significantly increased in the Adults ICU, yet, the incidence of carbapenem-resistant Gram-negative pathogens did not increase significantly. This finding depicts a trend to control MDR bacteria dissemination, but with the need of continuing strategy interventions with different drawing frequency, evaluation, and implementation than the rest of the hospital. 23
From the results of the correlation between the incidence of bacteremia and antibiotic consumption, most antibiotics used to treat carbapenem-resistant Gram-negative infections such as monobactams, carbapenems, colistin, tigecycline, and fosfomycin, separately and as a sum correlated with increased incidence of total carbapenem-resistant Gram-negative bacteremia in total Hospital Clinics and Departments and Adults Clinic and ICU. Interestingly, the increased incidence of total bacteremia is correlated with increased consumption not only with all antibiotics but also with advanced antibiotic in Adults Clinic and ICU, depicting early decisions for empiric therapy of advanced lines of antibiotic treatment. In our study, only linezolid 3 months before and nonadvanced antibiotics were associated with decreased incidence of total bacteremia.
In addition, the consumption of disinfectant solutions for hand hygiene statistically correlated with reduced incidence of total bacteremia, which indicated the importance of this control measure in the epidemiological hospital surveillance. Regarding the isolation of MDR carrier patients, this measure 2 months before correlated with increased incidence of carbapenem-resistant Gram-negative bacteremia, probably because of prolonged hospitalization of hematology patients in total hospital departments and adult clinic departments, while it correlated 2 months before with decreased incidence in adults ICU, implying shorter hospitalization in mix type of patients and infection control effectiveness.
A clear strength of our study is the prospective collection of data during a period of 6 years. The analysis of findings per clinic and department allowed more accurate conclusions. However, this study has some limitations that must be mentioned. First, as a single-center study, there may be local factors that preclude extrapolation to other centers. Second, many models have been fitted and many hypotheses have been tested since we investigated associations between multiple outcomes and many potential predictors in several clinics. Given that adjusting p-values for multiple testing is controversial, we decided to present unadjusted p-values which cannot exclude some inflation of the type I error beyond the typical 0.05 level. 24
Conclusions
We studied the impact of infection control measures implemented in the context of an ASP, on the incidence of MDR bacteremia. We found that the increased use of disinfectant solutions for hand hygiene significantly correlated with a decreased incidence of total bcteremia, indicating the importance of this measure in the epidemiological hospital surveillance. Also, increased isolation of MDR carrier patients 2 months before correlated with a reduction of the incidence of carbapenem-resistant Gram-negative bacteremia in Adults ICU, showing effectiveness in infection control. Time-series data offered the potential to estimate the impact of interventions over time and to guide infection control interventions in health care facilities.
Footnotes
Acknowledgment
We are thankful to the Infection Control Committee of the hospital.
Authors' Contributions
A.P. and M.K. were involved in the conception of the study. A.P. was involved in data acquisition and wrote the article. H.K. and T.P. contributed to data acquisition and methodology. G.K. and A.P. checked and approved the authenticity of the raw data. I.K. and N.P. analyzed the data. H.C.M. contributed to the writing of the article. G.C., P.G.K., and A.T. reviewed and edited the article. M.K. was involved in the supervision of the study and reviewed and edited the article. All authors read and approved the final article.
Disclaimer
The opinions presented in this article are those of the authors, and do not necessarily represent those of their institutions.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.