
Abstract
Data on Point Prevalence Surveys (PPSs) in India are limited yet. We report findings of a PPS conducted in a core “National Antimicrobial Consumption Network site” under National Centre for Disease Control - WHO project “Point prevalence survey of antimicrobial consumption at healthcare facilities.” A cross-sectional survey was conducted as per the “WHO methodology for PPS on antibiotic use in hospitals” in a tertiary care hospital in India in December 2021. Data were collected using predesigned and pretested questionnaire in separate hospital, ward, and patient forms. Eight hundred two inpatients (excluding ICUs) were covered out of whom 299 (37.3%) were on antibiotics with 11.7% receiving 3 or more antibiotics. Surgical prophylaxis (SP) (42.5%) and community acquired infections (32.8%) were the most common indications for antibiotic use. Of the patients, 92.5% received SP for more than 24 hrs. Most commonly prescribed antibiotics were penicillins with beta-lactamase inhibitors (22.3%). Of the total antibiotic prescriptions, 81.5% were from WHO essential medicines list and 12% from “not recommended” WHO AWaRe classification. Of the antibiotic prescriptions, 84.6% were parenteral. Few prescriptions complied with standard treatment guidelines (1.9%), documented indication for antibiotic use (11.6%), and stop/review date (4.4%) in notes. Double anaerobic cover accounted for 6.8% of the total prescriptions. Some identified areas for improvement were: formulation of hospital antibiotic guidelines, promoting culture of sending cultures, improvement in surgical antibiotic prophylaxis, decreasing use of antibiotic combinations and double anaerobic cover, fostering IV to oral switch of antibiotics, and ensuring effective communication among health care workers by documenting adequate information in medical notes.
Introduction
Antimicrobial resistance (AMR) was attributed to more than 1.2 million deaths globally in 2019 according to the landmark Global Research on Antimicrobial Resistance (GRAM) study. 1 Indiscriminate use of antimicrobials is the major driving force for extensive emergence and spread of resistance. 2 An alarming rise in antimicrobials' consumption was reported between 2000 and 2015 globally (65%), as well as in India (103%). 3 This is a serious affair given the emergence of multidrug resistant (MDR) and extensively drug resistant (XDR) pathogens in India. 4 Such concerns with rampant antimicrobial use and startling rise in AMR have ensued initiatives at various international and national levels5–9 with India being no exception.10–12 WHO launched the “Global Action Plan on Antimicrobial Resistance (GAP-AMR)” in 2015. 5 The Ministry of Health and Family welfare, India released its “National Action Plan on Antimicrobial Resistance” in 2017 (2017–2021) and listed surveillance of antimicrobial use in health care facilities for optimizing the use of antimicrobials under its fourth strategic priority. 10
Antimicrobial utilization data are crucial to map out strategies to promote their rational use and narrow down AMR. 13 Challenges associated with continuous antimicrobial surveillance such as time and resource extensiveness limit the applicability of this approach in vast majority of hospitals worldwide. 13 A viable alternative is to collect antimicrobial utilization data at a specific point in time using point prevalence survey (PPS) methodology. PPS is a validated method for measuring the antibiotic prescribing practices and other information relevant to management of infectious diseases and identifying targets for intervention. 14
PPSs on antibiotic use have been widely conducted in hospitals around the world.15–20 Results from the Global-PPS (2015) conducted across 53 countries in 303 hospitals revealed 34.4% prevalence of antimicrobial usage. 21 European Surveillance of Antimicrobial Consumption-PPS (ESAC-PPS), another pan-European survey conducted over 3 years, proved instrumental in identifying the targets for quality improvement. 22 The data on PPSs in India are, however, not much extensive yet.23–27
In India, National Centre for Disease Control (NCDC), New Delhi is the focal point for implementation and coordination of the AMR program. 10 NCDC in partnership with WHO Country Office for India has implemented a project on “Point prevalence survey of antimicrobial consumption at healthcare facilities” to quantify and analyze the trends of antimicrobial use in 36 tertiary care health centers attached to medical colleges across 27 states and union territories, which have been identified as National Antimicrobial Consumption Network (NAC-NET) sites. A “core group” has also been created comprising of six sites across different zones of the country, which will impart training to other sites. The present study reports the findings of the PPS conducted in one of the collaborating “Core NAC-NET sites.”
Patients and Methods
Study design and setting
The study was conducted as per the “WHO methodology for PPS on antibiotic use in hospitals”. 14 Prior approval from institute ethics committee (EC/NEW/INST/2020/874) and hospital management was obtained for conducting the survey.
The study site, Pt. B D Sharma Postgraduate Institute of Medical Sciences (PGIMS), Rohtak is a 2,080-bedded tertiary care hospital catering to population from Haryana and adjacent states (∼0.4–0.5 million annual admissions). Establishment of antimicrobial stewardship program is under process in the hospital. The microbiology department in hospital is well equipped with facilities for microbiological testing. Currently, local antibiotic prescribing guidelines are nonexistent, and antibiotics are mostly prescribed by consultants as per national/international guidelines.
A cross-sectional study was conducted in December 2021 using a predesigned and pretested PPS questionnaire. Case sheets of the patients admitted in medicine, surgery, obstetrics/gynecology, orthopedics, pediatrics, and ear, nose, and throat wards were considered for inclusion in the survey. Surgical wards were not surveyed following a weekend or public holiday due to relatively lesser number of elective procedures during these days, which can lead to erroneous data regarding surgical prophylaxis (SP).
All patients admitted in respective wards at 9:00 am on the day of survey were included; the patient/s had to be admitted at least since midnight. Exclusion criteria were patients admitted after 9:00 am or discharged before 9:00 am or due for discharge on the day of survey; daycare admissions such as for endoscopy or other minor procedure. Patients admitted in intensive care units (ICUs) were not included in the survey.
Data collection
Data were collected by trained medical undergraduate and postgraduate students, project nodal officer, and pharmacist using separate forms as described by “WHO methodology for PPS on antibiotic use in hospitals”: hospital form (number of acute/nonacute/ICU beds, overall admissions in the year before survey); ward form (denominator: number of admitted patients; and numerator: number of eligible patients, that is, patients receiving an antibiotic prescription); and patient form for all eligible patients. The patient form recorded data on patient demographic details (age, gender), underlying diagnosis, and antibiotic prescription details (name, dosage regimen, route of administration, duration of treatment, empirical or targeted therapy, compliance with treatment guidelines etc.).
Data were extracted from patients' case sheets and treatment charts. Any further information, if needed, was obtained from the ward resident or consultant in charge. Data were collected using google forms having provision of recording upto five antibiotics; for cases exceeding five prescriptions manual data recording on paper format had to be done. Data collection was restricted to antibiotic agents administered through nontopical routes only. No discussion or personal judgment on antibiotic prescribing was permitted during the survey. No personal identifiers were recorded to maintain data anonymity.
Data management & analysis
For the data obtained, following parameters were analyzed: (i) number (%) of patients on antibiotics; (ii) number (%) of antibiotic prescriptions for different indications namely community acquired infections (CAI), hospital-associated infection (HAI), SP, medical prophylaxis (MP; e.g., prevention of opportunistic infections in immunocompromised patients, prevention of bacterial infections in patients with late-stage cirrhosis, upper gastrointestinal bleeding, and acute necrotizing pancreatitis) and others; (iii) number (%) of patients on double anaerobic cover; (iv) quality indicators as described by “Global Point Prevalence Survey of Antimicrobial Consumption and Resistance” 28 : overall and ward-wise prevalence of antibiotic use; proportion of patients with hospital-associated infection (HAI); number (%) of parenteral antibiotic prescriptions; prolonged antibiotic prescribing for SP; prevalence of antibiotic use according to the WHO Essential Medicine List (EML) 2021 and AWaRe (Access, Watch, Reserve) classification 2021; and (v) additional quality indicators: documentation of reason for antibiotic use and stop/review date in notes; number (%) of antibiotics used as empiric/prophylactic/definitive treatment; and compliance with national/local treatment guidelines.
Statistical analysis
The data were collected using google forms and saved as excel files. Descriptive statistical analysis was carried out on Microsoft Excel. Data were expressed as discrete parameters namely counts or percentages. No statistical hypothesis was tested.
Results
The total number of beds in the sampled departments was 1,004 with a bed occupancy rate of 80% (802/1,004) on the days of survey. The departments with highest number of beds were obstetrics/gynecology, surgery, and medicine with 240, 230, and 216 beds, respectively. The highest prevalence of antibiotic use was reported in medicine wards (48%) followed by pediatrics (45.6%) and surgery (42.3%) (Fig. 1). Of the total 802 patients included, 299 were on antibiotics (37.3%) with 35 patients receiving 3 or more antibiotics (35/299: 11.7%). Total number of antibiotic prescriptions recorded was 482 with an average of 1.62 antibiotics prescribed per patient (range of number of antibiotics: 0–5).

Prevalence of antibiotic use in different wards. Admitted patients: total number of patients admitted in respective wards on the day of survey; Eligible patients: patients receiving an antibiotic prescription.
SP (127/299; 42.5%) was the overall most common indication for antibiotic use followed by CAI requiring hospitalization (98/299; 32.8%) and MP (45/299; 15%) (Fig. 2). However, there was variation in the indication of antibiotic use among individual wards (Fig. 3).
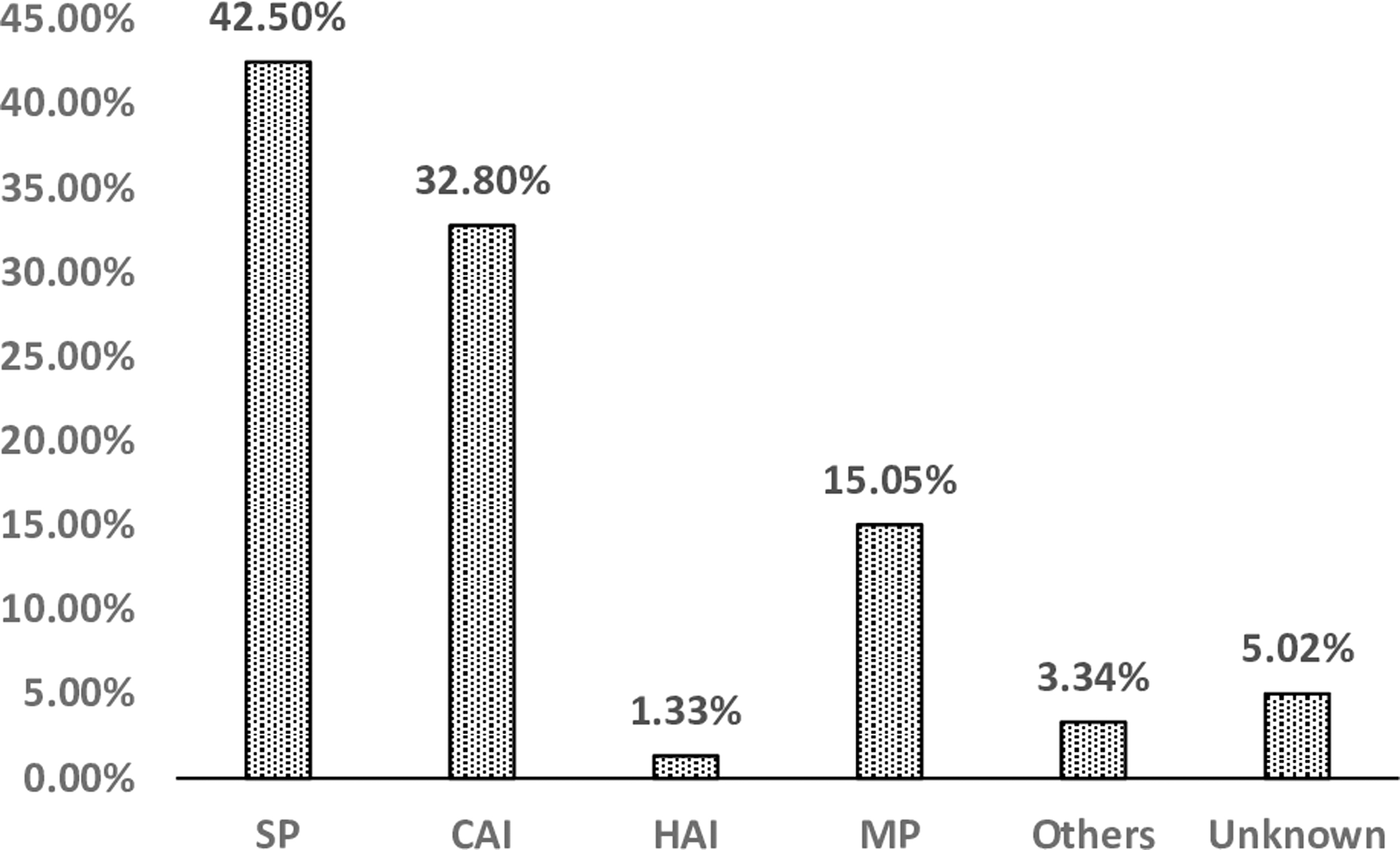
Percentage distribution of antibiotic use for different indications. CAI, community acquired infections; HAI, hospital-associated infection; SP, surgical prophylaxis; MP, medical prophylaxis.

Different indications for antibiotic use stratified by ward types. CAI, community acquired infections; HAI, hospital-associated infection; SP, surgical prophylaxis; MP, medical prophylaxis.
Most commonly prescribed antibiotics were combinations of penicillins with beta-lactamase inhibitors (22.3%) followed by 3rd generation cephalosporins (21.5%) and aminoglycosides (12.1%) (Fig. 4). The percentage distribution of various highly frequently prescribed antibiotic classes for various indications is depicted in Fig. 5. There was difference with respect to the choice of antibiotics used in various specialty wards (Fig. 6).

Overall antibiotic consumption according to WHO-ATC (Anatomical Therapeutic Chemical) class. Others include: doxycycline (J01AA02), 4th generation cephalosporins (J01DE), 2nd generation cephalosporins (J01DC), sulfamethoxazole/trimethoprim (J01EE01), penicillins with extended spectrum (J01CA), and polymyxins (J01XB).
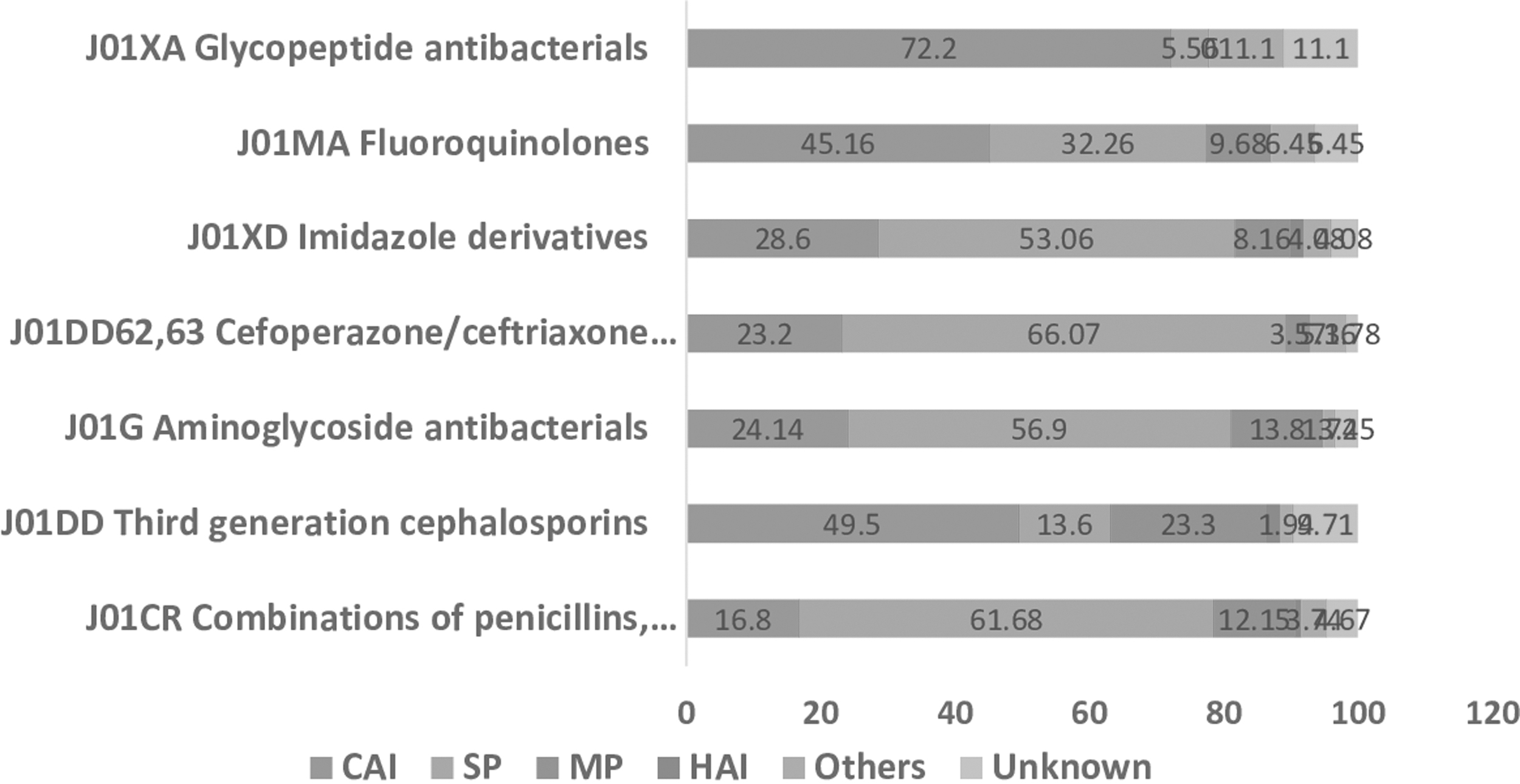
Percentage distribution of high frequency use antibiotic classes stratified according to indication.
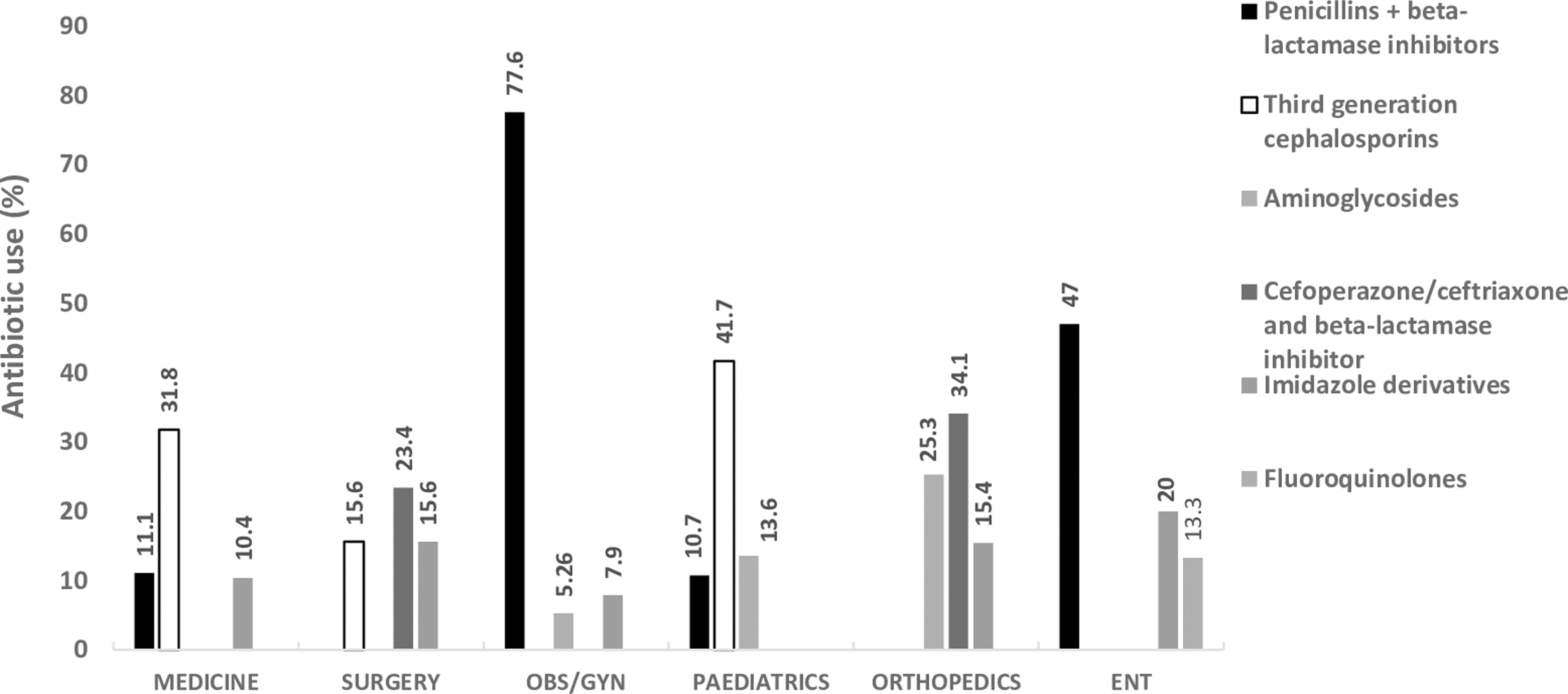
Percentage distribution of top three most common antibiotic prescriptions across different wards.
The most common indications for prophylactic use were obstetrics/gynecological conditions (38.6%), trauma (31.9%), gastrointestinal conditions (8%), late-stage cirrhosis/upper gastrointestinal bleed (7.4%), and neonatal conditions (6.1%). A total of 195 (40.4%) antibiotic prescriptions were for SP with an average of 1.62 antibiotics prescribed per patient (range: 1–3). Of the patients, 40.2% (51/127) received more than one antibiotic for SP. The most frequently prescribed antibiotics for SP included amoxycillin/clavulanic acid (27.5%), cefoperazone/ceftriaxone+ beta-lactamase inhibitor (21.6%), and amikacin (17.5%). For more than 24 hrs, SP was observed in 92.5% patients. For MP, amoxycillin/clavulanic acid (43.1%) and 3rd generation cephalosporins (38.5%) were the most common antibiotics prescribed.
Various CAI for which antibiotics were prescribed included respiratory tract infections (22.4%), gastrointestinal tract infections (17.3%), central nervous system infections (11.2%), hepatobiliary infections (10.2%), and skin/soft tissue infections (9.2%). For the treatment of CAI, 3rd generation cephalosporins and beta-lactam/beta-lactamase inhibitors were the frequently used antibiotics.
Of the total antibiotic prescriptions, 81.5% (393/482) and 67.6% (326/482) were from WHO EML and National List of Essential Medicines (NLEM) 2015. Among the antibiotics prescribed, those not included in both WHO EML and NLEM were cefpodoxime, cefepime, ceftriaxone/sulbactam, cefoperazone/sulbactam, levofloxacin, ofloxacin, ciprofloxacin/tinidazole, and rifaximin, while those not included in NLEM (included in WHO EML) only were amikacin, meropenem, and cefuroxime. The percentage distribution as per WHO AWaRe classification (2021) was: access (44%), watch (41%), reserve (2.7%), and not recommended (12.2%) (Fig. 7).
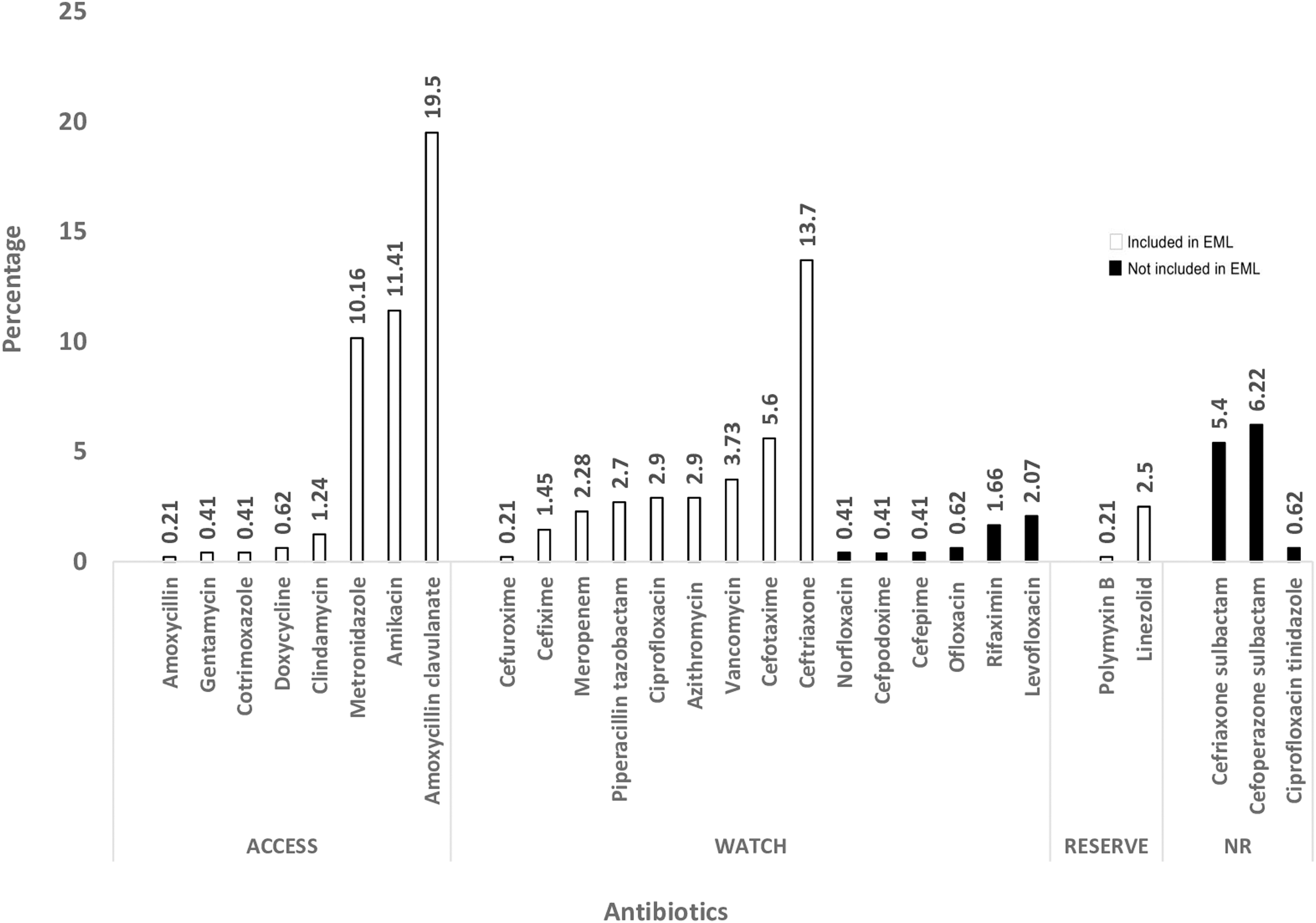
Prevalence (percentage) of antibiotic use classified at antibiotic level according to WHO-AWaRe classification. NR, not recommended; EML, Essential Medicine List (WHO).
Parenteral route of administration accounted for 84.6% (408/482) of the total antibiotic prescriptions. Few prescriptions had a clear documentation of reason for antibiotic use (56/482; 11.6%) and stop/review date (21/482; 4.4%) in notes. Antibiotic prescriptions for definitive use were observed in 2.5% (12/482) cases. Only 1.9% (9/482) of the total antibiotic prescriptions complied with standard national treatment guidelines. Double anaerobic cover accounted for 6.8% (33/482) of the total prescriptions with beta-lactam/beta-lactamase inhibitors and metronidazole (6%) being most commonly used drug combinations.
Discussion
Typically, there is a paucity of antimicrobial utilization data across India, which urgently needs to be addressed as the first stage to reduce inappropriate antimicrobial use. The present study evaluated the antibiotic prescribing practices for inpatients in our tertiary care hospital situated in North India.
The prevalence of antibiotic use (37.3%) reported in our survey is comparable to a teaching tertiary care hospital in central India (31.9%), 26 but is however lesser compared to an oncology center in eastern India (62% in 2014 and 69.1% in 2017). 29 Few multicentric PPSs conducted across India also reported higher prevalence of antibiotic use (50.3% and 57.4%)23,24 with rates ranging from 38.3% to 71.4% among individual centers in one survey. 23 One reason for such disparity may be the noninclusion of ICUs in our survey in contrast to other studies. ICUs, on account of catering to critically ill patients, are associated with huge antibiotic consumption as evident from 90% to 100% reported prevalence.16,30
PPS conducted in other parts of the world have reported variable prevalence of antibiotic use ranging from 29.2%, 33.6%, and 56% in multicentric surveys in Japan, 17 South Africa, 15 and China, 16 respectively, to 67.7% and 78.2% in single tertiary care referral centers in Kenya 31 and Nigeria, 30 respectively. Antibiotic use prevalence among individual wards in our study was however comparable to other surveys.16,30,31 Data on consumption of other groups of antimicrobials namely antivirals, antifungals, antimycobacterials etc. were also excluded from the present survey.
SP (35.4%) was the most common indication for antibiotic use, which was comparable to other surveys in India.23,24 More than half of the total patients surveyed (464/802: 57.8%) were admitted in surgical speciality wards namely surgery, orthopedics, and obstetrics/gynecology. Beta-lactam (amoxycillin and 3rd generation cephalosporins)-beta-lactamase inhibitor combinations were the most frequently prescribed agents for SP. There is a concern with high usage of these antibiotics for SP due to their not being indicated for this condition. The choice of antibiotic for SP shows wide variation across surveys conducted in different parts of the world.15,24,26,30 First generation cephalosporins are antibiotics of choice for many surgical procedures due to favorable cost, safety profile, and spectrum of activity. 32
Many factors govern the choice of antibiotic for SP such as the likely organisms contaminating the surgical site for a specific procedure, colonization with resistant organisms, and patient related factors such as antibiotic allergies etc. For instance, the use of relatively broad-spectrum agents for prophylaxis may be driven by the existent or discerned high prevalence of resistant bugs. An in-depth analysis of such factors may throw light on the plausible rationality or appropriateness of agents and regimens prescribed, which was however not possible with current insufficient microbiological and other relevant data in our setting.
In more than 90% cases, SP was continued for more than 24 hrs. This practice is not concordant with the various international guidelines recommending against the prolongation of SP postoperatively for the prevention of surgical site infections (SSIs).32–35 In fact, inappropriate or suboptimal use of antibiotics for SP is associated with antibiotic inefficacy and emergence of MDR organisms which in turn lead to increased risk of SSIs with consequent rise in treatment cost and morbidity. Ours being a tertiary care referral hospital with high rate of emergency surgeries in whom probability of infection cannot be precluded, antibiotics may well be prescribed empirically for a suspected infection. Another reason for continuation of prophylactic regimen after completion of surgery is postoperative fever as reported by Panditrao et al, 23 which was however not recorded in our survey due to paucity of information pertaining to indication for antibiotic use in majority of the medical notes.
Antibiotic use for SP is often contemplated as “low hanging fruit” in the field of antimicrobial stewardship. Considering the worrisome areas of concern with respect to duration and choice of antibiotics coupled with nonexistence of hospital policy for SP at present, targeting refinement in SP is the need of hour in our setting. Key strategies in this area would be formulation of hospital surgical antibiotic prophylaxis guidelines and educational interventions to promote rational antibiotic use among surgical patients.
Very few antibiotic prescriptions were based on culture and sensitivity tests despite the presence of functioning microbiology laboratories in our hospital. This may partly be explained by numerous discouraging factors for planning targeted antibiotic therapy such as lack of rapid diagnostics, antibiotic intake at earlier health care service contact before being referred here, over-the-counter antibiotic intake, longer turnaround time of microbiology reports etc. Hence, an important interventional strategy for effective antibiotic stewardship in this direction would be to promote the “culture of sending cultures”.
HAIs have been recognized as one of the major impetus for antibiotic use, especially so in lower middle income countries owing to extensive emergence and spread of MDR and XDR pathogens.31,36–38 Very few cases of HAIs accounting for antibiotic use identified in our survey may in fact reflect failure on part of clinician to accurately label an infection as HAI rather than a genuine phenomenon. Our observation in this context is also in disagreement with high incidence (19.2%) of HAI associated antibiotic prescriptions reported by Singh et al in a PPS across 16 private hospitals in India. 24 Another multicentric survey reported high variation in the rate of HAIs across five surveyed tertiary care hospitals (0.9% to 32.6%). 23
Antibiotics from the “Watch” and “Reserve” categories of the WHO AWaRe classification (2021) 39 were prescribed less often in contrast to few other reports,15,23 which may partially be explained by noninclusion of ICUs in our survey. However, “access” group of antibiotics was used quite less as against the WHO-defined common global target of >60% of overall antibiotic use 40 which may partially be explained by the spectrum of infective illnesses encountered in our tertiary care hospital. An exigency to favor the use of narrow spectrum “access” antibiotics in comparison to “watch” and “reserve” ones cannot be ignored to combat AMR. Fixed dose combinations of broad-spectrum antibiotics (3rd generation cephalosporins/beta-lactamase inhibitors; ciprofloxacin/tinidazole) accounted for more than 10 percent of total prescriptions, which is an area of concern as their use is neither evidence based nor recommended by WHO and various international guidelines. 39
Except for parenteral administration which had comparable frequencies, most of the quality indicators were not at par with similar surveys conducted within and outside India. High rate of parenteral antibiotics among inpatients may be ascribed to disease severity, contraindications for oral intake etc. In addition, 3rd generation cephalosporins and aminoglycosides, commonly prescribed antibiotics in this survey, are often available as parenteral formulations. The potential untoward effects associated with parenteral route such as prolonged hospitalization, catheter-related complications, health care expenses, and so on have been major drivers for targeting minimization in parenteral antibiotic use and IV to oral switch as key goals for antibiotic stewardship practices in hospitals. There is a need to encourage proper documentation regarding reasons for prescribing, stop/review date etc. in medical notes to ensure effective communication among health care workers.
A handful of prescriptions were reported as guideline compliant, referring to the choice of antibiotic prescribed. The reasons for noncompliance may be multifactorial namely local resistance patterns, concerns over therapy failure, diagnostic uncertainty etc. For majority of the prescriptions, nonavailability of relevant guidelines was the listed outcome for this indicator which suggests the pressing need to develop department-level antibiotic guidelines to optimize antibiotic use and continual monitoring of their implementation by means of periodic surveys or audits. The practice of redundant antibiotic use, for example, unwarranted duplicative therapy was not uncommon as is evident from a relatively high incidence of double anaerobic cover (6.8%) compared to an earlier survey (2.7%). 23 This suggests a room for improvement moving forward, and we plan to monitor this in the future.
We acknowledge a number of limitations in our study. The exclusion of ICUs led to discordant results in some parameters from other surveys conducted locally and globally. However, analogous figures were obtained when discrete data from individual (non-ICU) wards reported in some of them were compared with our study. Extraction of data from paper files and asking the floor resident for nonavailable information make the task quite laborious for study team. The study was also challenging in terms of mixed patient population, types and severity of infections, institutional factors like nonexistence of local antibiotic guidelines, and logistical challenges with targeted laboratory based antibiotic treatment—all of which have a bearing on antibiotic use patterns, thus necessitating caution while interpreting the results.
Conclusions
Few areas of improvement identified in our setting include: promoting the culture of sending cultures, formulation and implementation of hospital antibiotic guidelines, improvement in surgical antibiotic prophylaxis, increasing awareness in identifying HAIs, promoting the use of “access” group of antibiotics, decreasing use of antibiotic combinations and double anaerobic cover, fostering IV to oral switch of antibiotics, and ensuring effective communication among health care workers by documenting adequate information in medical notes. Maintenance of electronic medical record systems is an area to be prioritized especially in resource limited settings. The information, thus gathered, could serve as the basis and guidance for further more comprehensive and inclusive point-prevalence surveys driving establishment of antimicrobial stewardship interventions in ours, as well as other centers, with settings as our own.
Footnotes
Acknowledgments
The authors thank Dr. Geeta Gathwala (Director, PGIMS) and Dr. Ishwar Singh (Medical Superintendent, PGIMS) for granting permission to conduct PPS at our site. The authors acknowledge other members of the team who contributed to data collection: Deepak Nehra, Pankaj Kaushik, Sumit Kumar, Saurabh Patil, Bharat Pant, Komal, Rahul Deb, Himani, and all the undergraduate students.
Authors' Contributions
All authors made substantial contributions to all of the following: (1) the conception and design of the study, acquisition of data, and analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version submitted.
Disclaimer
The material has not been published or submitted for publication elsewhere.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.