
Abstract
Objectives:
This study reported a fatal stent-associated respiratory tract infection (SARTI) caused by carbapenem-resistant hypervirulent Klebsiella pneumoniae (CR-hvKP).
Case:
A bare-metal stent in the left main bronchus and a Y-shaped stent graft in the tracheal bronchus were placed successively in a 50-year-old woman due to shortness of breath after undergoing multiple chemotherapy treatments for lung cancer. Unfortunately, the followed SARTI and lung abscess in our patient caused by CR-hvKP eventually led to the death of the patient, despite our aggressive clearing of phlegm and potent antibiotics. The genomic analysis showed it was caused by a KPC-2-producing extensively drug-resistant K64-ST11 hypervirulent K. pneumoniae harboring several virulence and antimicrobial resistance genes.
Conclusion:
This study highlights the risk of SARTI caused by CR-hvKP in immunocompromised individuals.
Introduction
An endobronchial stent is often used in clinical practice to relieve tracheobronchial stenosis caused by nonsmall cell lung cancer, which can significantly improve the patient's respiratory function and improve the quality of life. 1 Stent placement can cause various complications, among which stent-associated respiratory tract infection (SARTI) is the most common. 2 Staphylococcus aureus and Pseudomonas aeruginosa are the dominant pathogens of SARTI, which can directly affect patients' outcomes.3,4 Whereas SARTI caused by carbapenem-resistant hypervirulent Klebsiella pneumoniae (CR-hvKP) is rare after searching the previous literature to the best of our ability in Pubmed.
Hypervirulent K. pneumoniae (hvKp), first identified in Taiwan in 1986, belongs to the family Enterobacteriaceae and is increasingly reported worldwide. 5 Recently sequence type (ST)11 CR-hvKP infections have been reported widely in China.6–8 To the best of our knowledge, this is the first reported clinical case of severe SARTI caused by ST11 CR-hvKP.
Case Presentation
A 50-year-old woman was admitted to the respiratory ward at a tertiary hospital located in China complaining of dry cough with hoarseness in July 2020. Her medical history included transurethral ureteroscopic holmium laser lithotripsy in our hospital for hydronephrosis and ureteral calculi about half a year before hospitalization. She was a housewife without habit of tobacco and alcohol. She had no hypertension or type 2 diabetes or similar underlying disease. No relevant family history, traveling history, or animal contact was reported. Her initial vital signs were as follows: blood pressure of 110/80 mmHg, pulse of 90 bpm, respiratory rate 14 breaths per minute, and body temperature 36.5°C.
There were no abnormal findings on physical examination but right supraclavicular, bilateral neck, and bilateral axillary lymphadenopathy. We took a supraclavicular lymph node biopsy, and the pathologist told us it was metastatic adenocarcinoma and came from the lung by immunohistochemistry. We perfected the systemic image examination and found no evidence of tumor metastasis in the skull, abdomen, and bones of the whole body. Even lung computed tomography (CT) examination only suggested there were some small nodules scattered in her lungs.
The tumor tissue was subjected to next-generation sequencing, and no gene mutations such as epidermal growth factor receptor, anaplastic lymphoma kinase, and c-ROS oncogene 1 receptor tyrosine kinase were found. The patient chose pemetrexed in combination with platinum-based chemotherapy once a month because of stage IV lung adenocarcinoma. The patient experienced neutropenia once during chemotherapy, which quickly returned to normal after the use of a granulocyte colony-stimulating factor.
On month 5, the patient presented with symptoms of chest tightness and shortness of breath for the first time. Chest CT and bronchoscopy revealed there was significant stenosis in her left main bronchus due to external bronchial pressure (Supplementary Material). Owing to the emergency, we placed a bare-metal stent in the patient's left main bronchus. The patient's symptoms of chest tightness and shortness of breath were immediately relieved. On month 15, the patient presented with symptoms of chest tightness and shortness of breath again and more seriously; chest CT and bronchoscopy revealed that her left and right main bronchi were too narrow for a bronchoscopy lens to enter (Supplementary Material).
After thorough deliberation, we placed a Y-shaped stent graft in the patient's tracheal bronchus using a rigid bronchoscope (Fig. 1A–C). After the operation, the patient can breathe smoothly under the condition of low-flow oxygen inhalation, but the patient had a lot of phlegm, which was difficult to cough up on the second day after the operation. Two weeks after the operation, the patient had difficulty breathing again, so we did a bronchoscopy for her. We found that a large amount of yellow thick sputum was attached to the patient's stent and even crusted, we used the bronchoscope to suck up the sputum as much as possible, and used a freezer to remove the sputum scab (Fig. 2A, B).

After Y-shaped stent graft placement in tracheal bronchus, the left and right main bronchi were obviously more open than before.
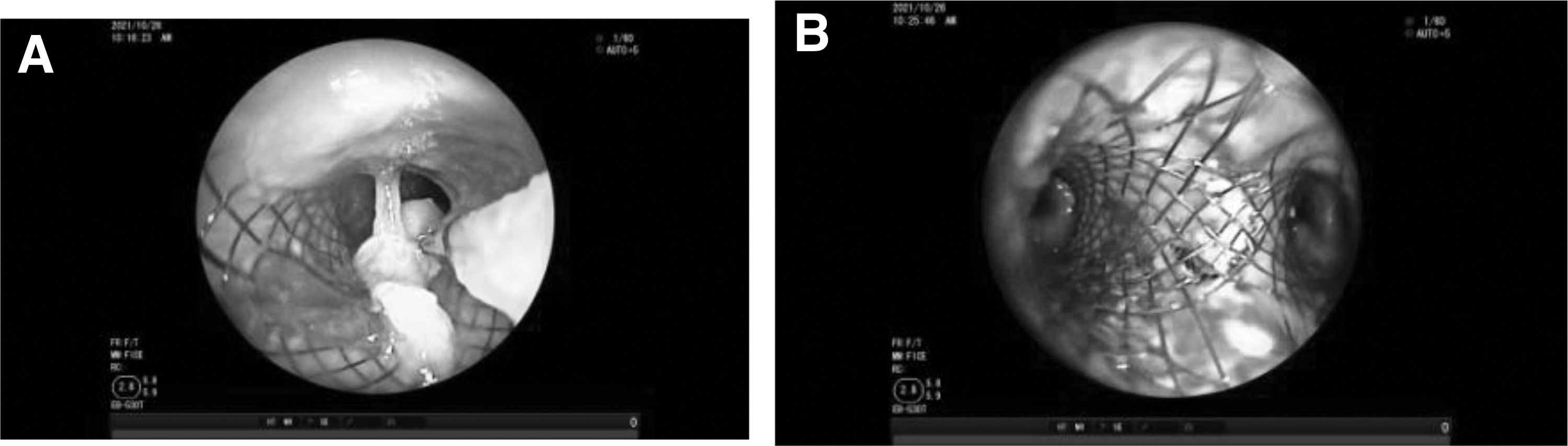
Two weeks after stent placement, a large amount of yellow thick sputum was attached to the patient's stent and even crusted, we used the bronchoscope to suck up the sputum as much as possible, and used a freezer to remove the sputum scab.
Bronchoalveolar lavage fluid bacterial culture was positive for P. aeruginosa, which is susceptible to most antibiotics (Supplementary Material). To treat severe SARTI, we gave the patient meropenem 1 g q8h. However, the patient's condition rapidly deteriorated. The patient breathed so hard that a noninvasive ventilator is required to maintain. On month 16, her blood pressure decreased, heart rate increased, and inflammatory markers raised, so we decided to take the stent out (Fig. 3A–C). Bronchoalveolar lavage fluid bacterial culture was positive for K. pneumoniae, which is almost resistant to all the antibiotics, except for polymyxin, tigecycline, and ceftazidime–avibactam.

Four weeks after stent placement, a large amount of yellow thick sputum was attached to the patient's stent again, we took the stent out, the left and right main bronchi were still very smooth.
Owing to the financial reasons of her family, we gave the patient cefoperazone sulbactam sodium combined with tigecycline. Two weeks after the stent removal, chest CT (Fig. 4) showed that the tumor was similar in size to that before stent removal, but there was a cavity-type infection in the right upper lung. To prevent superinfection caused by broad-spectrum antibiotics, we also gave the patient micafungin to inhibit fungi. On month 17, sputum bacterial cultures were repeatedly positive for the same carbapenem-resistant K. pneumoniae (CRKP).
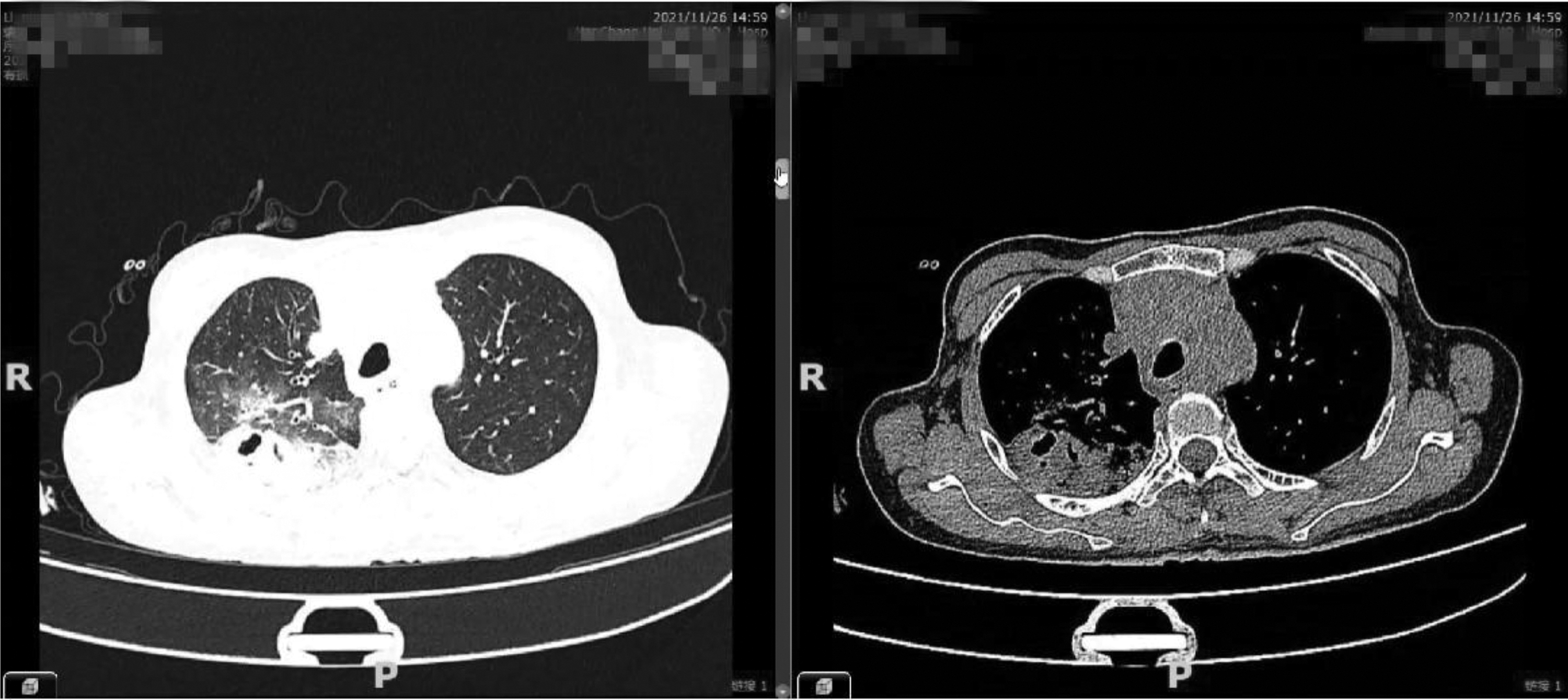
Pneumonia related to SARTI. Two weeks after the stent removal, chest CT showed that the tumor was similar in size to that before, but there was a cavity-type infection in the right upper lung. CT, computed tomography; SARTI, stent-associated respiratory tract infection.
Chest CT (Fig. 5) showed that the tumor was still similar in size to that before, whereas infectious lesions in the right upper lung markedly enlarged to form abscesses. The patient eventually died due to SARTI caused by CRKP, as shown in Fig. 6.
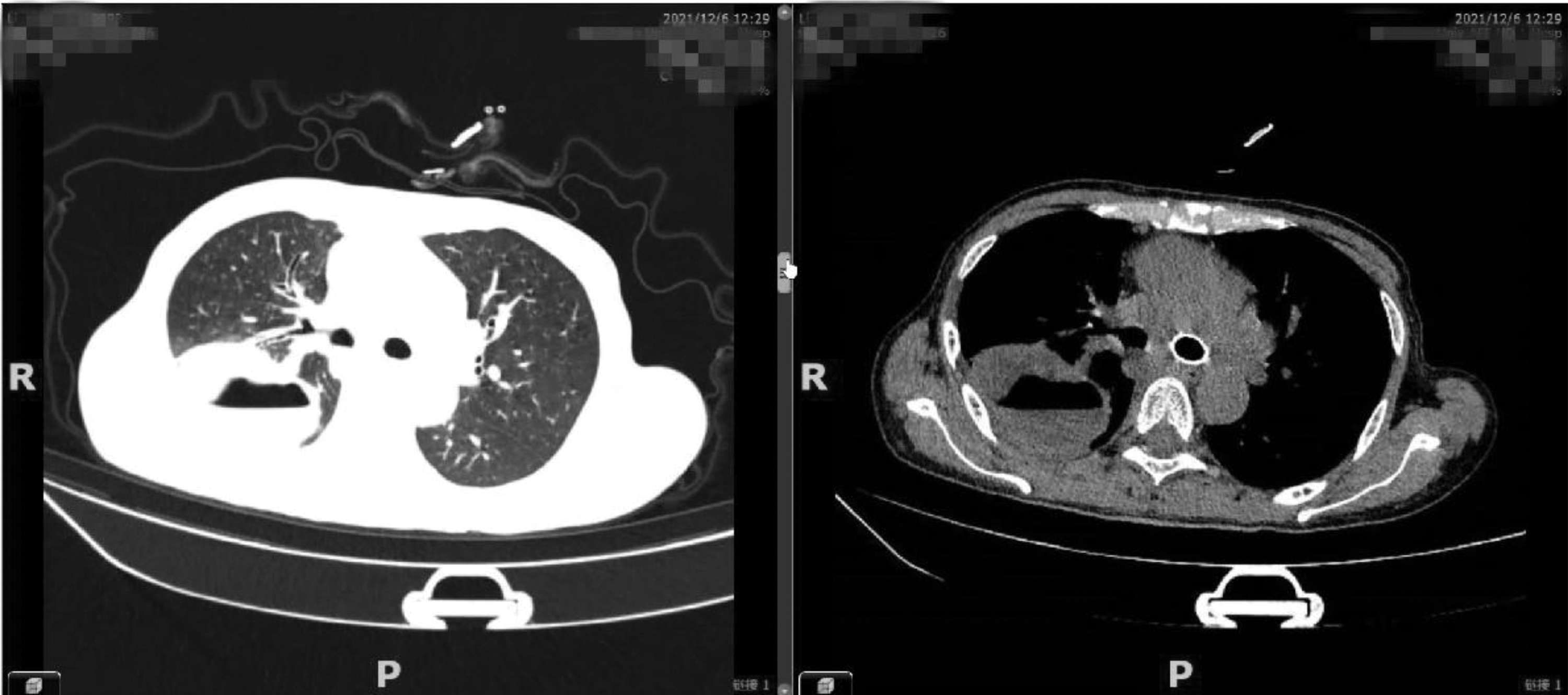
Lung abscess related to SARTI. Four weeks after stent removal, chest CT showed that the tumor was still similar in size to that before, whereas infectious lesions in the right upper lung markedly enlarged to form abscesses.

Treatment process from the admission to the death of the patient.
Bacterial Strains and Antimicrobial Susceptibilities
One month after the Y-shaped stent graft placement, multiple respiratory specimens were collected, and all the bacterial cultures were positive for K. pneumoniae by the VITEK-2 system. All isolates showed that the hypermucoviscosity phenotype was determined by the string test. 9 The antimicrobial susceptibility testing was performed using the VITEK-2 system (bioMérieux, Balmes-Les-Grottes, France) and confirmed by the microdilution method. Results were interpreted following the Clinical and Laboratory Standards Institute guidelines.
All isolates were characterized as resistant to imipenem or meropenem and were determined with phenotypic screening for carbapenemase production. The breakpoint of ceftazidime–avibactam was based on the interpretative criteria according to the U.S. Food and Drug Administration. Results of tigecycline and colistin were interpreted according to the breakpoint approved by the EUCAST. The reference strains—K. pneumoniae ATCC 700603 and Escherichia coli ATCC 25922—were used for quality control of antimicrobial susceptibility testing, as described previously. 10 The results showed that these K. pneumoniae were extensively drug-resistant (XDR) isolates, 11 remaining susceptible only to tigecycline, colistin, and ceftazidime–avibactam.
Whole Genome Sequence
Genome sequences were obtained using a combination of Illumina Miseq (150 bp paired-end) and they were assembled with SPAdes version 3.9.1. An average sequencing depth of 64 × was achieved for the genomes. Genomics analysis was performed as described in a previous study. 12 The CRKP genome was a single chromosome of 5,476,867 bp and five plasmids (Supplementary Material). Multilocus sequence typing revealed that the two CR-hvKP strains were ST11 (gapA-infB-mdh-pgi-phoE-rpoB-tonB, Allele No. 3-3-1-1-1-1-4), and the K64 serotype was confirmed through capsular typing using the wzi allele.
Resistance genes and plasmid replicons were determined using the ResFinder and PlasmidFinder web services. Genome analysis showed that resistance genes for β-lactam (carbapenemase gene blaKPC-2, blaSHV-12, blaCTX-M-14, blaSHV-182, blaLAP-2, blaTEM-1B), sulfonamide (sul2), fosfomycin (fosA), and trimethoprim (dfrA14) were detected. Also, plasmid-mediated [qnrS1, aac(6′)-Ib-cr] for quinolone resistance and plasmid-mediated [aac(6′)-Ib3] for aminoglycoside resistance were detected.
The following plasmid replicons were observed: IncR and ColRNAI, IncFII, IncHI1B, repB. In addition, the search for virulence factors detected genes related to the phenolate siderophore yersiniabactin (ybtA, ybtE, ybtP, ybtQ, ybtT, ybtU, and ybtX), aerobactin (iucABCD-iutA), and capsule-regulated genes (rmpA and rmpA2), and irp1, irp2, and fyuA. These virulence-related determinants including yersiniabactin, aerobactin, and capsule-regulated genes are considered to be from the pLVPK-like virulence plasmid of hvKP. 13
The irp2 gene is considered an important virulence factor for extraintestinal infection establishment. 14 Furthermore, mannose-specific adhesin subunit of type 3 fimbriae mrkABCDF and mrkHIJ loci, able to mediate bacterial adhesion and biofilm formation for several surface structures, was also detected. 15
Mouse Lethality Assay
Determination of the virulence of K. pneumoniae in mouse lethality assay and the medium lethal dose (LD50, expressed as colony-forming units) was performed as previously described. 16 The mouse lethality assay proved that all these CRKP isolates were hypervirulent, having the 50% lethal dose (LD50) of <103 CFU (colony-forming unit), and were a little lower virulent than the hvKP strain NTUH-K2044 having the LD50 of <102 CFU.
Ethics Statement
The study was evaluated by the ethics committee of our hospital. The spouse of the patient has provided informed consent for publication of the case.
Discussion
A review concluded that probably one in five patients with airway stents were affected by SARTI. 2 Whereas there was a higher incidence (27.2%) of SARTI described in China Meitan General Hospital, which is one hospital with the most interventional treatments under bronchoscopy in China. 4 A plausible explanation for the higher incidence of SARTI in China could be that metal stents are used more than nonmetal stents in China because of lower operating difficulty. In general, the incidence of SARTI in metal stents was higher than that of nonmetallic stents. 17
A bare-metal stent in the left main bronchus and a Y-shaped stent graft in the tracheal bronchus were placed successively in our patient. Though the most common pathogen of SARTI P. aeruginosa also infected our patient, we soon eradicated the antibiotic-sensitive pathogen by using the carbapenem antibiotic meropenem.
K. pneumoniae is Gram-negative bacilli associated with opportunistic and nosocomial infections such as pneumonia, meningitis, and bacteremia. 18 Typically, classical K. pneumoniae strains cause serious infection in immunocompromised individuals, including people suffering from diabetes or malignancies. 19 Our patient had undergone multiple chemotherapy treatments because of lung cancer, moreover, stent placement destroyed the local immunity and expectoration ability of bronchial mucosa. Since the 1990s, the increasing number of CRKP infections bring great challenges to global public health associated with significant morbidity and mortality, whereas ST11 is predominant in China.20–22
Even more concerningly, in 2018, a fatal outbreak of ST11 CR-hvKP in a Chinese hospital was first reported by Chen and colleagues. 6 Owing to the acquisition of pLVPK-like virulence plasmids by ST11 CRKP strains, ST11 CR-hvKP strains simultaneously exhibit the features of hyper-resistance and hypervirulence. 6 Carbapenem resistance and hypervirulence were exhibited by different well-separated K. pneumoniae lineages in the past, but their convergence clones CR-hvKP—both highly pathogenic and resistant to most available antibiotics—have increasingly been reported in China.12,13,23
However, to the best of our knowledge, this is the first reported clinical case of severe SARTI caused by ST11 CR-hvKP. Resistance genes for beta-lactam (blaKPC-2, blaSHV-12, blaCTX-M-14, blaSHV-182, blaLAP-2, and blaTEM-1B), sulfonamide (sul2), fosfomycin (fosA), and trimethoprim (dfrA14), plasmid-mediated [qnrS1 and aac(6′)-Ib-cr] for quinolone resistance, and plasmid-mediated [aac(6′)-Ib3] for aminoglycoside resistance detected in our isolate made it XDR. Similarly, the virulence genes such as yersiniabactin (ybtA, ybtE, ybtP, ybtQ, ybtT, ybtU, and ybtX), aerobactin (iucABCD-iutA), capsule-regulated genes (rmpA and rmpA2), irp1, irp2, and fyuA made it hypervirulent, as proved in the mouse lethality assay. The ST11 CR-hvKP caused a lung abscess in our patient for a short time and eventually led to the death of the patient, despite our aggressive clearing of phlegm and potent antibiotics.
Conclusion
In summary, we described a rare and fatal case of SARTI caused by K64-ST11 KPC-2-producing CR-hvKP that occurred in China. Therefore, clinicians should recognize this rare clinical entity and collect specimens under bronchoscopy early and repeatedly in patients with potentially severe SARTI. In addition, our case highlights the clinical importance of keeping in mind CR-hvKP infections as a possible cause of SARTI in immunocompromised individuals, and of NGS to identify CR-hvKP strains for appropriate treatment.
Footnotes
Authors' Contributions
T.T.Z. and F.Y.Y. made substantial contributions to clinic data collection. Z.Z.Z. and X.P. made contributions to the literature review. J.C. and W.Z. revised the article critically for important intellectual content. W.J.L. drafted the article. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
Financial support was provided by the National Natural Science Foundation of China (81860368), Natural Science Foundation of Jiangxi province (20202BAB206048, 20224BAB216084) and The first affiliated hospital of Nanchang University Young Talents Scientific Research Breeding Fund (YFYPY202114).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.