
Abstract
The indoor environment of hospitals should be considered as an important reservoir of azole resistant Aspergillus species. In this study, we evaluated azole-containing agar plates (ACAPs) and antifungal susceptibility testing (AFST) for the detection of azole-resistant Aspergillus species in hospital environmental samples. Between September 2021 and January 2022, environmental samples (108 instruments and 12 air) were collected from different wards of 4 educational hospitals in Mazandaran province, Iran. All samples were cultured using ACAPs. Recovered Aspergillus isolates were molecularly identified at species level using partial DNA sequencing of beta-tubulin gene. AFST of Aspergillus species was performed using the Clinical and Laboratory Standards Institute M38-A3 guideline. Screening for cyp51A mutations was also done. Overall, 18 (15.0%) isolates of Aspergillus species were recovered from ACAPs, of which Aspergillus tubingensis (50%) and Aspergillus fumigatus (38.9%) were the commonest species. No isolate of Aspergillus species grew on posaconazole (PCZ)-containing agar plates. Among the 18 Aspergillus isolated species from ACAPs, 83.3% were related to samples from instruments. Of the nine isolates of A. tubingensis, 22.2% and 44.4% isolates showed minimum inhibitory concentration (MIC) = 2 μg/mL against voriconazole (VCZ) and itraconazole, respectively; and 44.4% isolates showed MIC = 1 μg/mL against PCZ. Of the seven isolates of A. fumigatus, one (14.3%) was resistant to VCZ. This isolate showed F46Y, G54E, G138C, M172V, M220I, D255E, T289F, G432C, and G448S mutation in cyp51A. Our finding showed the emergence of high MICs in cryptic and non-fumigatus species of Aspergillus such as A. tubingensis and VCZ resistance in A. fumigatus in indoor environment of hospitals.
Introduction
Invasive aspergillosis (IA) has been presented as one of the most life-threatening nosocomial infections in vulnerable patients, especially patients with hematological malignancies or immunodeficiency diseases in different countries. 1 In contrast, the indoor environment of hospitals is a potential reservoir of Aspergillus species, a phenomena that bring both the host and the infective agent together. 2 In addition, ubiquitous outdoor conidia of Aspergillus species enter into indoor environment of hospital wards as the main source of fungal contamination. 3 Hence, in the chain of the infectious disease (such as IA) process, reservoir plays an important role.
Currently, systemic triazole antifungal agents such as voriconazole (VCZ) and posaconazole (PCZ) are commonly used in prophylaxis and treatment of IA. However, different Aspergillus spp. may vary in their susceptibility to the triazole antifungals. Furthermore, the emergence of Aspergillus isolates resistant to one or multiple antifungal drugs is a major clinical concern globally. 4
Antifungal susceptibility testing (AFST) is a routine in vitro technique for evaluation of antifungal drug activity against different fungi, including Aspergillus spp., and as an important parameter to detection of antifungal resistance in different fungal species. However, several studies have shown that an easy-to-use susceptibility test, azole-containing agar plates (ACAPs), may be used for screening of resistance in Aspergillus fumigatus against triazole antifungals in various environmental and clinical samples.5–9
The first version of the E.Def 10.1 as the standard method for the screening of azole resistance in A. fumigatus isolates was released by European Committee on Antimicrobial Susceptibility Testing Subcommittee on AFST in September 2018 and subsequently published. 10 The second version E.Def 10.211 was defined as the standard method for the phenotypic detection of A. fumigatus isolates potentially resistant to itraconazole (ICZ), VCZ, or PCZ that includes a corresponding agar-based screening method used to detect echinocandin non-wild-type (WT) Aspergillus spp. isolates. The ACAP is available commercially from VIPcheck (Boven-Leeuwen, The Netherlands). However, in several studies in-house ACAPs were used for the detection of azole resistance in Aspergillus spp., especially A. fumigatus.6–9
Therefore, in the present study, we evaluated the ACAPs and AFST for detection of azole-resistant Aspergillus spp. in hospital environmental samples collected from different wards in four educational hospitals in Mazandaran province, Iran.
Materials and Methods
During September 2021–January 2022, a total of 120 samples were collected from medical equipment (n = 108) and air (n = 12) of 4 educational hospitals from Mazandaran province, a northern province of Iran. The samples were taken from the surfaces of medical equipment and appliances, for example, computer, ventilators, telemeters, pacemakers, anesthesia machines, endotracheal tubes, and sinks, floors, and walls in different wards, including intensive care unit (ICU), neonate ICU, operating room, surgery, neonatal, and oncology. According to the existence of different wards and their number in each hospital, at least four samples were collected from the devices in each ward. In each ward, indoor air was also evaluated for airborne fungal spores. This study was approved by the Ethics Committee of the Mazandaran University of Medical Sciences (Code: IR.MAZUMS.REC.1398.538).
Sampling and laboratory work
The tubes containing a cotton swab and Phosphate Buffered Saline (PBS) +0.1% Tween 20 (2–3 mL) (PBS: KCL: 0.2 g, KH2PO4: 0.2 g, NaCl: 8 g, Na2HPO4: 1.15 g with pH: 7.4) were prepared and sterilized. Surface samples were collected by pressing the cotton swab on each of different areas of equipment and appliances or surface of walls and returned into tube. And then, the tubes were quickly transferred to the laboratory. Each tube-containing swab was separately shaken by a shaker (Techne, UK) for 1 min and after that the swab was safely discarded, and tube centrifuged for 10 min at 3000 rpm. The supernatant was discarded, and the sediment was vortexed for 30 sec. Then 20 μL of each sediment was inoculated into in-house ACAPs containing sabouraud dextrose agar (SC, Condalab, Madrid, Spain) plates with VCZ (1 mg/L), ICZ (4 mg/L), and PCZ (0.5 mg/L), separately. The plates were incubated at 37°C for 7 days.
The airborne fungal spores were also collected using settle plates. Opened Petri dish plates containing the above mentioned media were placed at the level of breathing height from 1 to 1.5 m for each room for 15 min. The collected plates were incubated as described above.
Aspergillus species identification
Recovered Aspergillus isolates were subcultured onto SC and identified at species level using partial DNA sequencing of beta-tubulin gene. DNA was extracted from colonies grown for 5–7 days on SC (Difco Laboratories, Detroit, MI). Polymerase chain reaction (PCR) for partial amplification of the β-tubulin-encoding gene (benA) was performed using forward and reverse primers [forward primer (5′-GGTAACCAAATCGGTGCTGCTTTC-3′), reverse primer (5′-ACCCTCAGTGTAGTGACCCTTGGC-3′)]. The reactions were conducted in a GeneAmp PCR system 9700 thermocycler (Applied Biosystems, San Francisco, CA) in a total volume of 25 μL containing 12.5 μL of master mix (200 μmol/L deoxynucleoside triphosphates, 4.0 mmol/L MgCl2, and 2.5 U of Taq DNA polymerase), 2 μL of genomic DNA (∼10 ng), 25 pmol of each primer, and H2O. The following cycling conditions were used: initial denaturation for 5 min at 94°C, 35 cycles of denaturation at 94°C for 1 min, annealing at 68°C for 1 min, and extension at 68°C for 2 min.
PCR products were analyzed by electrophoresis in 1.5% agarose gels, and the amplified benA fragments were sequenced using the same primers with the ABI3730xL Genetic Analyzer platform (Applied Biosystems, Waltham, MA). All sequence data were subjected to nucleotide BLAST search of the NCBI database and the molecular database of the WI-KNAW Fungal Biodiversity Center (Utrecht, The Netherlands), and isolates were identified at species level. The sequences were deposited in GenBank.
In vitro antifungal susceptibility test
Azole in vitro susceptibility testing of A. fumigatus isolates was performed using the Clinical and Laboratory Standards Institute (CLSI) M38-A3 guideline. 12 The final concentration of antifungal drugs in the wells ranged from 0.016 to 16 μg/mL for VCZ (Pfizer, Sandwich, UK), ICZ (Janssen Pharmaceutica N.V., Beerse, Belgium), and PCZ (Merck, Sharp and Dohme BV, Haarlem, The Netherlands). All antifungal stock solutions were diluted in dimethyl sulfoxide. The Aspergillus strains were cultured on Potato dextrose agar (Difco Laboratories) supplemented with 0.02% chloramphenicol and incubated at 27–30°C for 5 to 7 days for sufficient sporulation. Conidial suspensions were prepared by scraping the surface of fungal colonies with a sterile cotton swab moistened with physiological saline containing 0.05% Tween 20. The optical densities were adjusted ranging from 80% to 82% transmission measured at 530 nm and were then diluted 1:50 in RPMI 1640 medium, and the final inoculum was between 0.4 × 104 to 5 × 104 CFU/mL. The microdilution plates were incubated at 35°C for 48 hr.
The minimum inhibitory concentration (MIC) was determined visually by comparison of the growth in the wells containing the drug with that of the drug-free control. For four drugs in our study MIC was read at 100% inhibition compared to the control well. Candida krusei (Pichia kudriavzevii) (ATCC 6258) and Candida parapsilosis (ATCC 22019) served as quality control (QC) strains.
Table 1 shows the epidemiological cutoff values (ECVs) of antifungal agents against A. fumigatus, Aspergillus flavus, and Aspergillus niger as defined by CLSI supplement M57S. 13 According to the CLSI M38M51S 14 MIC breakpoint for VCZ against A. fumigatus isolates was classified as susceptible (MIC ≤0.5 mg/L), intermediate (MIC = 1 mg/L), and resistant (MIC ≥2 mg/L). For cryptic species, the MIC distribution is presented without applying the ECV of each section.
Epidemiological Cutoff Values of Itraconazole, Voriconazole, and Posaconazole Against Aspergillus fumigatus, Aspergillus flavus, and Aspergillus niger
According to the CLSI M38M51S (10) MIC breakpoint for VCZ against A. fumigatus isolates was classified as susceptible (MIC ≤0.5 mg/L), intermediate (MIC = 1 mg/L), and resistant (MIC ≥2 mg/L).
CLSI, Clinical and Laboratory Standards Institute; ICZ, itraconazole; MIC, minimum inhibitory concentration; PCZ, posaconazole; VCZ, voriconazole.
Screening for lanosterol 14-α sterol demethylase gene (cyp51A) mutations
All isolates which showed the MIC values above the ECV to ICZ and/or identified as resistant against VCZ (MIC ≥2 μg/mL) in in vitro AFST were submitted to sequencing of cyp51A gene. Three primer pairs were used for amplifying the whole cyp51A gene. These primers included: CYP1-R (5′-AGCCTTGAAAGTTCGGTGAA-3′), CYP1-L (5′-CACCCTCCCTGTGTCTCCT-3′), CYP2-R (5′-CCTTGCGCATGATAGAGTGA-3′), CYP2-L (5′-CATGTGCCACTTATTGAGAAGG-3′), CYP3-R (5′-CCTTTGAAGTCCTCGATGGT-3′), and CYP3-L (5′-TTCCTCCGCTCCAGTACAAG-3′). The initiation of the PCR amplification was with an initial denaturation for 1 min at 95°C, and 35 denaturation cycles occurred at 94°C (60 sec), 60°C (30 sec), and 72°C (60 sec), followed by an end 10-min extension at 72°C. For detecting potential mutations in the PCR products, which were evaluated by DNA sequence analysis, a comparison was made between the sequence of the products and WT A. fumigatus cyp51A sequence using DNA Baser Assembler version 5.15.0.
Results
Screening for azole resistance in Aspergillus spp.
Out of the 120 collected samples, 18 (15.0%) isolates of Aspergillus spp. were recovered from ACAPs, of which Aspergillus tubingensis (50%, 9/18) and A. fumigatus (38.9%, 7/18) were the most prevalent species (Fig. 1). Of all collected samples, only Trichoderma (n = 3) and Rhizopus (n = 1), as non-Aspergillus species, were isolated from ITZ and PCZ and ITZ containing agar plates, respectively.
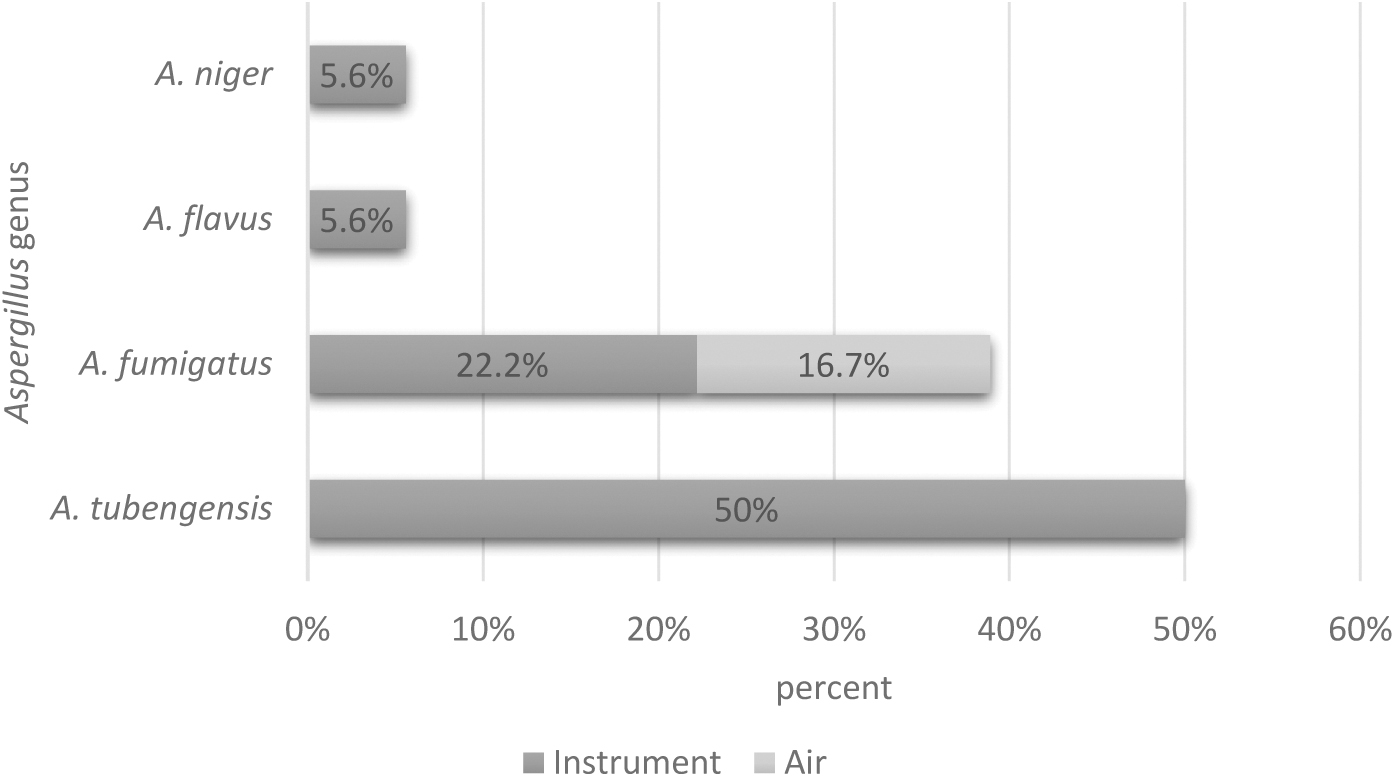
The distribution different species of Aspergillus from azole-containing agar plates based on type of collected samples.
The accession number of 18 isolates of Aspergillus species was available at gene bank OQ646673 to OQ646688; and OQ606233 and OQ606234.
In VCZ-containing agar plates, A. tubingensis (33.3%, 6/18) was the most prevalent isolate, followed by A. fumigatus (22.2%, 4/18) and A. flavus and A. niger (5.6%, 1/18 each). While in ICZ-containing agar plates, A. tubingensis and A. fumigatus had a similar isolation rate (16.7%, 3/18 each) (Fig. 2). No isolate of Aspergillus species grew on PCZ-containing agar plates. Among the 18 Aspergillus isolated species from ACAPs, 83.3% (15/18) were related to sample from instruments and 16.7% (3/18) to air samples. In air samples, A. fumigatus was the only isolated species (Fig. 1).
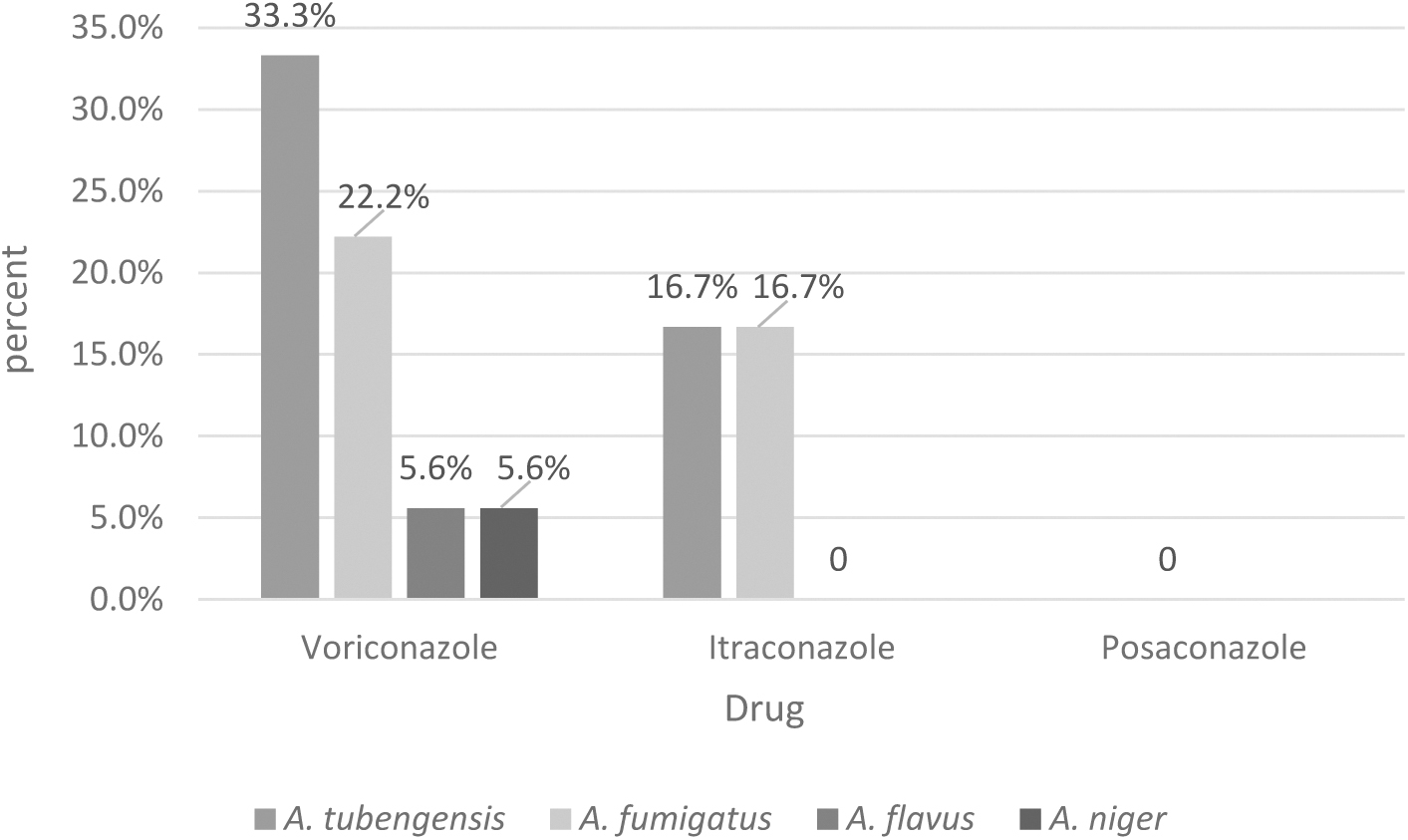
The distribution of Aspergillus species isolated from agar plates containing voriconazole, itraconazole, and posaconazole.
Azole in vitro susceptibility testing
VCZ had MIC ranging from 0.125 to 4 μg/mL against all Aspergillus isolates compared to 0.062 to 2 μg/mL for ICZ and 0.062 to 1 μg/mL for PCZ. PCZ (0.16 μg/mL) had the lowest geometric mean (GM) MIC values followed by ICZ (0.33 μg/mL) and VCZ (0.41 μg/mL), respectively. Among 18 isolates of Aspergillus spp., the most frequency of MIC to PCZ was 0.25 μg/mL, for VCZ was 0.125 and 0.25 μg/mL, and for ICZ was 0.063, 0.25, and 2 μg/mL. PCZ (MIC50/MIC90 0.25/1 μg/mL, GM MIC 0.23 μg/mL) and ICZ (MIC50/MIC90 1/2 μg/mL, GM MIC 0.5 μg/mL) exhibited the lowest and the highest in vitro activity against A. tubingensis isolates, respectively. PCZ (MIC50/MIC90 0.125/0.25 μg/mL, GM MIC 0.11 μg/mL) and VCZ (MIC50/MIC90 0.25/0.25 μg/mL, GM MIC 0.34 μg/mL) showed the lowest and highest in vitro activity to A. fumigatus isolates (Table 2).
In Vitro Antifungal Susceptibility Profile of Aspergillus Species Isolated from Azole-Containing Agar Plates (n = 18)
Among seven isolates of A. fumigatus identified from ACAPs, one (14.3%) was resistant to VCZ (≥4 μg/mL). Of the nine isolates of A. tubingensis, two (22.2%) isolates showed MIC = 2 μg/mL against VCZ, four (44.4%) isolates showed MIC = 2 μg/mL against ICZ, and two (44.4%) isolates showed MIC = 1 μg/mL against PCZ (Table 2). Two isolates of A. fumigatus and one isolate of A. tubingensis showed high MIC values in both VCZ and ITZ containing agar plates. Using the chi square test, no statistical correlation was seen between the result of in-house ACAPs to find ARAf and MIC values generated by susceptibility testing (pv = 0.52).
The A. fumigatus resistance to VCZ isolate (number 22) showed F46Y, G54E, G138C, M172V, M220I, D255E, T289F, G432C, and G448S mutations in cyp51A gene locus.
Discussion
A large number of studies worldwide have recently acknowledged the development of Aspergillus spp. especially A. fumigatus resistance to azole derivatives globally from environmental and clinical origins. In the present work, we screened the indoor environmental samples obtained from different hospitals using ACAPs and AFST for detection of azole-resistant Aspergillus spp.
In the present study, in the initial screening, we used ICZ/VCZ/POS-containing agar plates to identify resistant Aspergillus isolates. This approach revealed a rate of 15% (18/120) azole resistance among isolated Aspergillus species. The use of ACAPs has been implemented in different studies in different ways. In line with some previous reports,9,15,16 in this present study we used ACAPs as a screening method for isolation of resistant Aspergillus spp. directly in environmental samples. In some studies,7,8,17,18 Aspergillus spp. were first isolated using SC and then ACAPs used to screen for resistance in isolated species of Aspergillus. However, in most studies,7,8,15–18 AFST was used to confirm the resistance in isolated strains. In this present study, A. tubingensis (33.3%) and A. fumigatus (22.2%) were identified as the main isolates in VCZ-containing agar plates and both of them had a similar isolation rate (16.7%) in ICZ-containing agar plates. In Alvarez-Moreno et al. 19 study, among 34 isolated A. fumigatus from soil samples 18 (52.9%) grew on agar supplemented with ICZ or VCZ.
According to AFST results, in our study, among seven isolates of A. fumigatus, one strain (14.3%) was identified as resistant to VCZ. Although in the absence of a specific definition for ECV in CLSI protocol for cryptic species of Aspergillus which makes it impossible to classify resistant species but in the present study, A. tubingensis showed MIC = 2 μg/mL against VCZ and ICZ in 22.2% and 44.4%, respectively. In addition, 22.2% of isolates showed MIC = 1 μg/mL against PCZ. However, there was no statistical correlation between the MIC values produced by the susceptibility test and potential plate-based (ACAP) resistance.
In Godeau et al. study, 20.5% of A. fumigatus isolates from indoor environment of hospitals using EUCAST protocol were resistant to azoles. In a report from the Thailand, azole-resistant A. fumigatus was identified in 10/308 (3.2%) of the soil samples. 20 In Chowdhary et al. study from India of 105 soil samples from the agricultural fields, 6 (5.7%) and 8 (7.6%) A. fumigatus strains were found on VCZ and ICZ-containing agar plates, respectively. Prigitano et al. 21 identified A. fumigatus in 25.4% of the 173 soil samples on ICZ-containing agar plates, whereas no A. fumigatus grew on VCZ-containing agar plates. Among several environmental studies from Colombia, 18 China, 22 United Kingdom, 23 and Iran, 16 the rate of ACAPs for Aspergillus strains was reported as 9.3%, 2.2%, 6.2%, and 21%, respectively. These variations in results may reflect the geographical source of the samples, using commercially or in-house ACAPs for recovery of Aspergillus isolates and type of sample sources.
It is worth mentioning that in this study, C. krusei (P. kudriavzevii) and C. parapsilosis were used as QC strains based on the CLSI protocol for AFST of filamentous fungi. Since in this protocol, the MIC range and mode of QC strains are defined and recorded for each drug, and QC strains are considered as a measure of the quality of the response of each drug, the accuracy of AFST implementation is evaluated by how each drug responds to QC strains. Therefore, it seems that the use of yeast-like fungi as QC for AFST of filamentous fungi cannot be a limitation of the test.
In a recent review, Burks et al., 24 among the 28 published studies, a total of 570 azole-resistant isolates of A. fumigatus from the developed environments, including gardens, public parks, workplaces, hospitals, and homes, were identified, of which 58% (27.1% from the indoor and 31.9% from outdoor very near to hospital areas) were recovered from hospital settings.
In this present study, the amino substitutions at F46Y, G54E, G138C, M172V, M220I, D255E, T289F, G432C, and G448S in one isolate of A. fumigatus showed VCZ resistance. The point mutations in CYP51A were reported in azole-resistant environmental and clinical A. fumigatus isolates. Literature review showed that TR34/L98H substitution was considered as the most known mutation in A. fumigatus which recovered from Iranian clinical and environmental samples.25–28
In the present study, however, we couldn't find any mutation at TR34/L98H in our one isolate of A. fumigatus which showed resistance to VCZ. TR46/Y121F/T289A alternations were reported in clinical isolates of A. fumigatus. 29 Similarly, TR46/Y121F/T289A substitution was also reported from environmental samples of A. fumigatus isolated in Iran. 16 In line with present study in a study from Iran alternation at M172V amino acid was recorded. 29 The mutations at amino acid substitution at F46Y, M172V, M220I in this research were seen in other studies.30,31 To the best of our knowledge, in this present study some new mutations such as G54E, G138C, D255E, T289F, G432C, and G448S are reported for the first time from Iranian environmental isolates of A. fumigatus.
Most previous studies were focused on the detection of azole resistance in A. fumigatus; however, according to our previous experiences from Iran, A. flavus and A. tubingensis were mainly identified species of Aspergillus from clinical and environmental samples.23,24,32–36 Therefore, non-fumigatus species of Aspergillus need to consider seriously in aspect of epidemiological distribution and azole resistance, globally. In this current study focus on the hospital environmental samples as a reservoir of different opportunistic fungi, including those with resistance to azole agents, a phenomenon that brings the patients at risk of invasive fungal infections and a challenging infective agent together is a positive point.
Conclusion
Our finding showed the emergence of high MICs in cryptic and non-fumigatus species of Aspergillus such as A. tubingensis and VCZ resistance in A. fumigatus in indoor environment of hospitals which is a serious concern when managing patients vulnerable to aspergillosis. Our findings showed that ACAPs may be useful for the screening of A. fumigatus azole-resistant isolates. The sequencing result on only one environmental isolate of VCZ resistance A. fumigatus showed some new mutations, including G54E, G138C, D255E, T289F, G432C, and G448S in cyp51A gene locus.
Footnotes
Acknowledgments
The authors are grateful for the support and collaboration of all administrators of hospitals.
Authors' Contributions
M.G.: methodology, investigation, and original draft. M.T.H.: conceptualization, supervision, review, and editing. M.A., I.H., S.H., S.Y., B.N., and M.M.: methodology, investigation, and resources. F.B.: review and editing.
Authors' Confirmation Statement
Dr. M.G., Dr. M.A., Dr. I.H., Dr. M.M., Dr. S.H., Dr. S.Y., Dr. B.N.S., and Dr. M.T.H. are from Mazandaran University of Medical Sciences (Sari, Iran), where the primary functions are education and research.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a research fund (No. 5219) from Invasive Fungi Research Center of Mazandaran University of Medical Sciences, Sari, Iran.