
Abstract
Little is known about the characteristics of uropathogenic Escherichia coli (UPEC) associated with recurrent urinary tract infections (RUTIs). The present study aimed to analyze the phenotypic antimicrobial resistance of recurrent UPEC isolates attributable to either relapse or reinfection. A total of 140 E. coli strains were isolated from 70 outpatients with RUTIs. All isolates were analyzed by random amplified polymorphic DNA-polymerase chain reaction to evaluate genetic similarity between the first and second isolates. We found that 64.2% (45/70) of outpatients had a relapse with the primary infecting E. coli strain and 35.7% (25/70) had reinfection with a new E. coli strain. Compared with reinfecting strains, relapse UPEC isolates exhibited much higher antimicrobial resistance; 89% of these isolates were multidrug-resistant and 46.6% were extended-spectrum β-lactamase producers. Our study provides evidence that RUTIs are mainly driven by the persistence of the original strain in the host (relapses) despite appropriate antibiotic treatments, and only RUTIs attributed to relapses seem to favor multidrug resistance in UPEC isolates.
Introduction
Urinary tract infections (UTIs) are characterized by a high frequency of recurrence, even after appropriate antibiotic therapy, 1 and they are mostly caused by uropathogenic Escherichia coli (UPEC). 2 Recurrent urinary tract infections (RUTIs) are defined as “relapse” when they are caused by the resurgence of the same strain that caused the original UTI, or as “reinfection” when they are caused by the reintroduction of a new strain into the urinary tract.3,4 The ability of UPEC to persist at subclinical levels as intracellular reservoirs that are not susceptible to most antibiotic treatments likely contributes to the recurrence of UTIs after cessation of antibiotic administration.5–7
The emergence of antimicrobial resistance is a major medical concern (particularly in low- and middle-income countries) 8 that limits therapeutic alternatives and increases morbidity and mortality. 9 Of particular concern is the increase in extended-spectrum β-lactamase (ESBL)-producing E. coli, causing UTIs in recent years.10,11 Moreover, UPEC is becoming increasingly resistant to many of the antimicrobials used to treat UTIs. In many areas of the world (e.g., Mexico City), resistance to ciprofloxacin and TMP/SMX has a prevalence of over 55%.12–14 The impact of multiple antimicrobial treatments on the increase in antimicrobial resistance in patients with RUTIs is still unclear. We believe that recurrent infections, especially those attributable to failure of the initial treatment (i.e., relapse), may lead to antibiotic resistance since persisting bacteria are exposed to multiple antibiotics. Here, we analyze phenotypic antimicrobial resistance of recurrent UPEC isolates attributable to either relapse or reinfection RUTIs and compare them with resistance profiles of isolates from nonrecurrent UTIs.
Materials and Methods
Source of bacterial strains and selection criteria
Urinary samples of outpatients aged 1–70, suffering from RUTI, were collected between 2016 and 2019 from General Hospital “Dr. Manuel Gea González” (SSA, Ministry of Health). Informed consent was obtained from patients who donated urine samples. Sample collection, quantification, and identification were performed as previously described. 14 Isolates that were biochemically confirmed as E. coli were maintained in Luria Bertani (LB) broth with 20% glycerol at –20°C. Seemingly healthy individuals with uncomplicated acute cystitis were selected as urine donors. Samples were collected during the diagnosis of UTIs. Patients were excluded if they met one of the following criteria: if they were pregnant; had diabetes, obstruction, or functional abnormalities of the urinary tract; had been treated with antibiotics for UTI within the last 30 days; were immunocompromised; or if other sources of infection were present. A total of 140 E. coli clinical isolates were obtained from urine samples from 70 outpatients with symptoms of lower UTI: 2 isolates per patient from repeated UTI episodes occurring within an interval between 2 weeks and 6 months. The first E. coli sample was isolated before antimicrobial treatment and the second sample was isolated when the patient returned to the hospital with clinical symptoms of UTI despite conducting the appropriate antimicrobial treatment (after an antibiotic sensitivity test, the patients were treated with an appropriate antimicrobial drug following the clinical practice guidelines established by The Secretary of Health of Mexico). Additionally, 85 strains were isolated from patients with uncomplicated and sporadic UTI (nonrecurrent), without a history of RUTIs; urine samples were collected in the same year and with the same selection criteria as the RUTIs.
Definitions
A case of acute E. coli UTI was defined according to the presence of the following symptoms: significant bacteriuria with an E. coli count of ≥104 CFU/mL of midstream urine, pyuria with ≥5 leukocytes/mm3, and clinical signs or symptoms of UTI (urgency for urination, dysuria, suprapubic pain, or low lumbar/flank pain). RUTI refers to at least two episodes of repeatedly occurring UTIs, documented by urine culture within more than 2 weeks. We classified recurrence as a relapse when a strain from the second episode had an identical random amplified polymorphic DNA-polymerase chain reaction (RAPD-PCR) pattern to that of the initial episode. Recurrence was considered a reinfection when the RAPD-PCR pattern was different between the initial and subsequent episodes.
DNA extraction
We prepared templates for RAPD-PCR by boiling; 15 single colonies were inoculated in 1 mL of LB in a 1.5-mL microcentrifuge tube and were incubated as standing cultures at 37°C for 16 hours. The cells were centrifuged (in a bench centrifuge) at maximum speed for 2 minutes. The pellet was washed twice in sterile distilled water; cells were then suspended in 300 µL of distilled water and boiled for 10 minutes. The supernatant was used immediately as a template source for PCR. The DNA concentration and purity in the supernatant were determined using a Nanodrop One spectrophotometer (Thermo Scientific).
RAPD-PCR analysis
To determine whether two isolates from each patient (70 patients) had identical E. coli clones, a RAPD-PCR typing assay was developed for this study. A PCR was applied to each sample, containing one primer; 1254 (5′-CCGCAGCCAA-3′).16,17 RAPD analysis of E. coli isolates was performed according to procedures described previously by Bart et al. 18 with a few modifications. Briefly, the mixture used for PCR of RAPD contained: 100 ng of template DNA, 5 pmol/µL (primer 1254), each nucleotide (dATP, dCTP, dGTP, dTTP) at 0.2 mM, 3.0 mM MgCl2, 1× of buffer 10×, and 1U (1254 primers) of Taq polymerase (Vivantis) in a final volume of 25 µL. The following cycling conditions were used: 94°C for 1 minute, 4 cycles of 94°C for 4 minutes, 36°C for 4 minutes, and 72°C for 4 minutes, and 35 cycles of 94°C for 1 minute, 36°C for 1 minute, and 72°C for 2 minutes with a final 10 minutes elongation step at 72°C. The PCR reaction products were separated on 1.5% (wt/vol) agarose gels in 0.5× TBE buffer or polyacrylamide gels and stained with ethidium bromide (BIO-RAD) for 45 minutes. The BIONUMERICS software (Applied Maths NV), was used for analyzing DNA fingerprint gel images. 19 The Jaccard coefficient was used to determine the percentage of similarity between the samples. The dendrograms were prepared applying the algorithm UPGMA (unweighted pair-group method with arithmetical averages) for the formation of clusters for graphical representation.
Antimicrobial susceptibility testing and detection of ESBL phenotype
The antimicrobials drugs were amikacin (AMK, 30 μg), amoxicillin/clavulanic acid (AMC, 20/10 µg), ampicillin (AMP, 10 μg), cephazolin (KZ, 30 μg), cefepime (FEP, 30 μg), ceftriaxone (CRO, 30 μg), ciprofloxacin (CIP, 5 μg), fosfomycin (FOS, 200 μg), gentamicin (CN, 10 μg), meropenem (MEM, 10 μg), nitrofurantoin (F, 300 μg), and trimethoprim-sulfamethoxazole (SXT, 25 μg). Antibiotic disks were obtained from Oxoid Ltd. UK. The United States National Committee for Clinical and Laboratory Standards (CLSI) guidelines were used to produce the antibiograms (disc diffusion on Mueller-Hinton agar, Oxoid; with incubation for 24 hours at 37°C) and to interpret the inhibition halos. 20 The inhibition zones were measured and then classified as sensitive or resistant; reduced susceptibility was also classified as resistance. E. coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as reference strains for antibiotic disk controls. Multidrug-resistant (MDR) was defined as resistance to three or more different classes of antibiotics. ESBL production was determined by the double-disk synergy test according to Jarlier et al. 21 This test was performed by placing disks of ceftazidime, cefotaxime, and ceftriaxone (30 μg each) at a distance of 20 mm (from center to center) from a disk containing amoxicillin with clavulanic acid (20 and 10 μg, respectively). The strains that showed synergy between oxyimino-β-lactams and clavulanic acid were classified as ESBL-producing strains. Klebsiella pneumoniae ATCC 700603 was used as the positive control and E. coli ATCC 25922 as the negative control.
Statistical analyses
For statistical analysis, a χ2 test was used to assess the significance of differences between groups. For the tests, a p value of <0.05 was considered statistically significant.
Results
Inclusion of the study participants
A total of 140 E. coli strains were isolated from 70 outpatients with RUTIs (two isolates per patient; men, women, or children) with a variety of ages (1–70) from 2016 to 2019. Strains consisted of one isolate before the beginning of antimicrobial treatment and one isolate at the first bacteriological recurrence, after treatment of patients with significant E. coli bacteriuria. All patients had recurrences within 5 months of the first UTI episode. For comparative purposes, the data of patients from nonrecurrent cases are included in Table 1. Patients were 70% female and 30% male; 48.6% of them were 30–59 years old (79.4% females and 20.5% males) (Table 1). Notably, Table 1 shows that 14.2% of the recurrence cases occurred in girls under 14 years of age, while in nonrecurrent UTI cases, the percentage was 4.7; this difference was statistically significant. RUTI cases increased by 4.4% in men older than 60 years compared with nonrecurrent UTI cases.
Age, Gender, and Number of Patients with Recurrent Urinary Tract Infections and Patients with Nonrecurrent Urinary Tract Infections
A p value <0.05 (bold) was considered statistically significant.
RUTI, recurrent urinary tract infection; UTI, urinary tract infection.
Genetic relatedness by RAPD-PCR
All isolates were analyzed by RAPD-PCR (using primer 1254) to evaluate genetic similarity between the first and second isolates and to discriminate between relapses (i.e., the same strain) or reinfections (a new strain), and based on this RAPD analysis, a dendrogram was constructed (Fig. 1), (Fig. 2). Identical electrophoretic profiles in the first and second isolates evidenced relapses in 45 patients (64.2%), while differences between the first and second isolates evidenced reinfections in 35.7% of them.
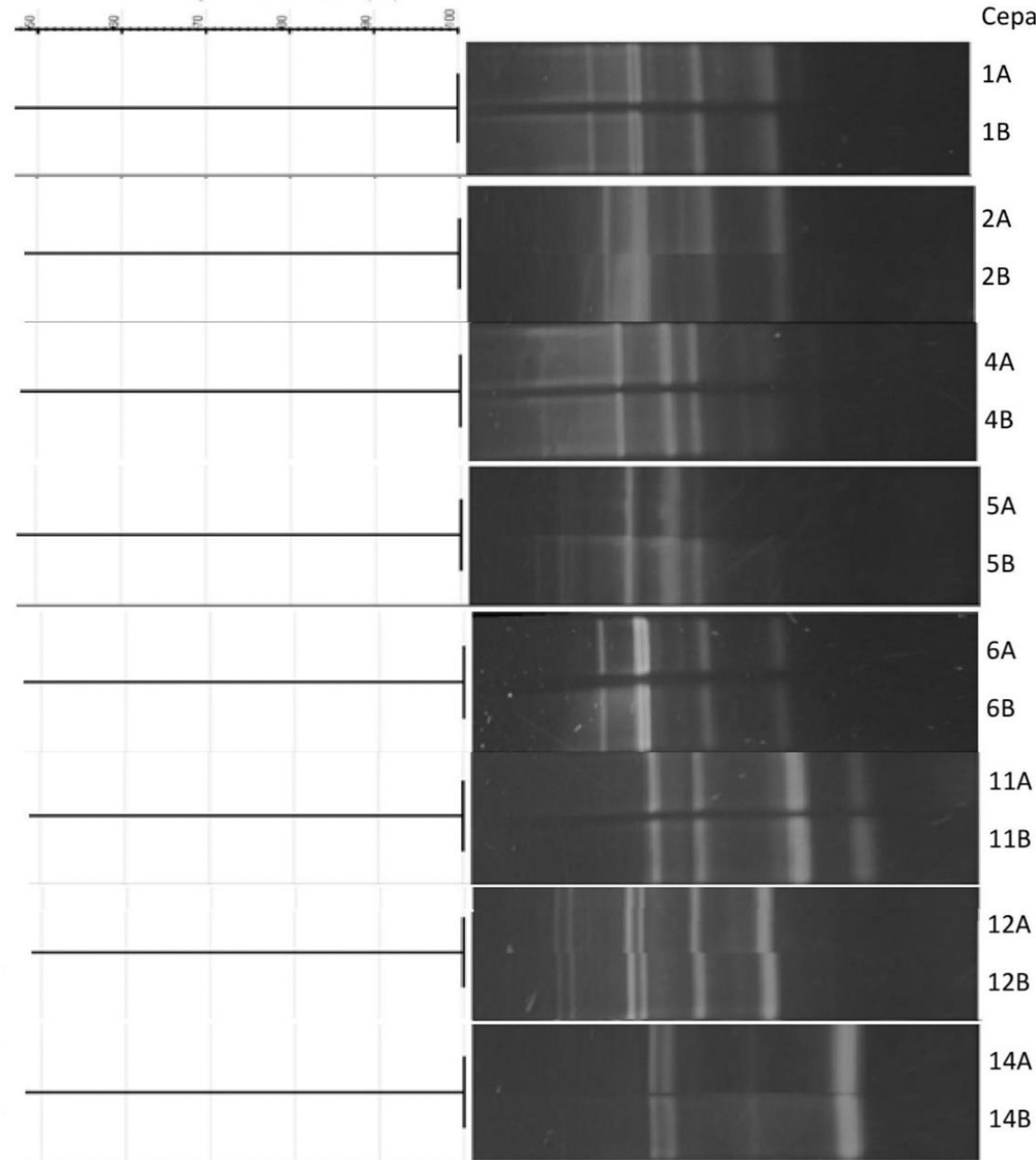
Dendrogram derived from UPGMA cluster analysis using Jaccard’s similarity indices based on RAPD profiles for 16 strains: 2 strains isolated from the same patient in 2 episodes of infections. Primer 1254 was used in the PCR.

Dendrogram derived from UPGMA cluster analysis using Jaccard’s similarity indices based on RAPD profiles for 74 strains: two strains isolated from the same patient in two episodes of infections. Primer 1254 was used in the PCR.
Antimicrobial susceptibility and ESBL phenotypes
The antibiotics tested were those commonly prescribed to treat UTIs. The antimicrobial resistance profiles of E. coli isolates from relapse or reinfection RUTIs cases are compared in Table 2. Antibiotic resistance rates were higher in relapse isolates; there was a statistically significant difference in resistance to 6 out of 12 antibiotics (ampicillin, amoxicillin-clavulanic acid, cefazolin, ciprofloxacin, trimethoprim-sulfamethoxazole, and gentamicin) (Table 2). Interestingly, the resistance profiles of isolates from reinfections and nonrecurrent UTIs were very similar. However, the prevalence of MDR isolates was 89% (40/45) in relapse cases, 52% (26/50) in reinfection cases, and 45.8% (39/85) in nonrecurrent UTI cases.
Percentage of Resistance to Different Antimicrobial Agents in Escherichia coli Isolated from Recurrent Urinary Tract Infections (Relapse or Reinfection) or Nonrecurrent Urinary Tract Infections
A p value of <0.05 (bold) was considered statistically significant.
The first and second isolates of 40 relapse cases presented identical antimicrobial resistance profile. Only in five relapse cases some differences in resistance were found between the first and second isolates (Table 3). These changes occurred in the isolates; key 12, where the 1st isolate was resistant to SXT and CN and in the 2nd isolate, they changed to susceptible; isolate key 45, the 1st isolate was susceptible to SXT and in the 2nd isolate changed to resistant; isolate key 47, the 1st was resistant to CRO and in the 2nd, changed to susceptible; isolate key 51, the 1st was resistant to CRO and FEP and in the 2nd, changed to susceptible; finally, isolate key 52, the 1st was susceptible to AMK and CN and in the 2nd, changed to resistant (Table 3).
Antimicrobial Resistance to Antimicrobial Agents in 90 Escherichia coli Causing Urinary Tract Infection Relapses, First and Second Isolates from Two Infectious Episodes per Patient
Two isolates per patient (1st and 2nd) from two different infectious episodes of 45 patients, in total 90 isolates.
R, resistant;
AMP, ampicillin; AMC, amoxicillin-clavulanic acid; KZ, cefazolin; CRO, ceftriaxone; FEP, cefepime; MEM, meropenem; CIP, ciprofloxacin; SXT, trimethoprim-sulfamethoxazole; AMK, amikacin; CN, gentamicin; FOS, fosfomycin; F, nitrofurantoin.
In 95 isolates from RUTIs, ESBL-producing E. coli were phenotypically detected in 46.6% (21/45) of relapses and 26% (13/50) of reinfections. All ESBL-producing E. coli were MDR in relapses and 11/13 were MDR in reinfections.
Discussion
We sought to determine whether recurrent infections, especially those attributable to the failure of the initial treatment (i.e., relapse), may lead to antibiotic resistance. Here, we analyzed the antimicrobial resistance of E. coli strains from relapse or reinfection RUTIs and compared them with resistance profiles of isolates from nonrecurrent urinary infections; we show that RUTIs are mainly relapses despite appropriate antibiotic treatment, which could lead to the emergence of antimicrobial resistant strains.
We found that 64.2% of the RUTIs were owing to relapses caused by the same UPEC strain, which is consistent with previous studies also using molecular typing methods; relapse rates up to 68% have been reported.4,22,23 Although our study involves a few cases from a single area of Mexico City, it is worth noting that RUTIs in girls under 14 years of age and in men over 60 years of age were more common than previously known. In our study, relapses occurred even after appropriate antimicrobial treatment indicating that the bacteria were not eliminated from the urinary tract, thus, possibly re-emerging from quiescent intracellular reservoirs that can persist in the bladder, 24 or from reinfection with the same bacterial strain from the gut or the vagina. 25
We found a significant difference in antimicrobial resistance between isolates from relapses and reinfections (Table 2): a much higher percentage of relapse isolates (18–32% higher than in reinfection isolates) were resistant to antibiotics (e.g., gentamicin, trimethoprim/sulfamethoxazole, ciprofloxacin, cefazolin, amoxicillin/clavulanic ac., and ampicillin). Moreover, 89% of relapse isolates were MDR, while only 52% of reinfection isolates were MDR. Additionally, the number of relapse isolates containing ESBL producers was nearly twice that of reinfection isolates. This big difference in antimicrobial resistance is particularly striking since previous studies reported no significant differences in antimicrobial susceptibility between relapse or reinfection isolates.26,27
In a similar study, Ahn et al. 28 showed that among patients who experienced UTI recurrence caused by ESBL-producing E. coli, 71% had recurrences with ESBL-producing E. coli. In another study conducted in Mexico, recurrent symptomatic UTIs were significantly associated with development of ESBL-producing E. coli causing UTIs. 29
We believe that the observed increase in bacterial resistance is owing, in part, to constant exposure of bacteria to antibiotics after numerous treatments selecting resistant bacteria, as resistance patterns are strongly associated with previous antibiotic exposure. 30 It is well known that continuous ingestion of antibiotics promotes the emergence and selection for bacterial resistance. 31 It is noteworthy that the most empirically prescribed antibiotics in Mexico are trimethoprim/sulfamethoxazole, ciprofloxacin, and cephalosporins (cefepime and ceftriaxone), 32 which were among the antibiotics with the highest levels of resistance (particularly in relapse isolates).
Bacterial cells called “persisters” are a subpopulation of slow-growing or growth-arrested bacterial cells with decreased susceptibility to antibiotics that coexist with a susceptible clonal bacterial population. 33 We still do not know whether some of our isolates are of the “persister” type; however, accumulating evidence indicates that “persisters” have a significant role in the relapse and recalcitrance of infections. 33
Conclusions
Our study provides evidence that UPEC isolates from RUTIs, especially those that cause relapses (strains that persist in the host for long periods), tend to be MDR. We find that isolates from relapses were more resistant to the antimicrobials tested than isolates from reinfections. However, the biological basis of MDR in these isolates remains to be explored.
Footnotes
Acknowledgment
We thank the Faculty of Medicine, UNAM, for the facilities and donations of reagents.
Authors’ Contributions
S.G.-P.: Conceptualization, methodology, validation, investigation, project administration, writing original draft. P.C.-G.: Methodology, formal analysis, investigation. S.V.-R.: Resourses, validation. R.H.-C.: Investigation, Resourses, writing—review and editing. A.M.-H.: Conceptualization, formal analysis, resourses, visualization, supervision, funding acquisition, writing—review and editing.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This work has not been supported by any funding agency.