
Abstract
Carbapenem-resistant Klebsiella pneumoniae (CRKP) infection has become a significant threat to global health. The application of chemical disinfectants is an effective infection control strategy to prevent the spread of CRKP in hospital environments. However, bacteria have shown reduced sensitivity to clinical disinfectants in recent years. Furthermore, bacteria can acquire antibiotic resistance due to the induction of disinfectants, posing a considerable challenge to hospital infection prevention and control. This study collected 68 CRKP strains from the Fifth Affiliated Hospital of Xinjiang Medical University in China from 2023 to 2024. These strains were isolated from the sputum, urine, and whole blood samples of patients diagnosed with CRKP infection. Antibiotic susceptibility tests were performed on CRKP strains. Concurrently, the minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) of disinfectants (benzalkonium bromide, 1% iodophor disinfectant, alcohol, and chlorine-containing disinfectant) against the test isolates were determined by the broth microdilution method. The efflux pump genes (cepA, qacE, qacEΔ1, qacEΔ1-SUL1, oqxA, and oqxB) were detected using polymerase chain reaction. The results showed that 21 out of the 68 CRKP strains exhibited extensive drug resistance, whereas 47 were nonextensively drug-resistant. The MIC value for benzalkonium bromide disinfectants displayed statistically significant differences (p < 0.05) between extensively drug-resistant (XDR) and non-XDR strains. Additionally, the MBC values for benzalkonium bromide disinfectants and 1% iodophor disinfectants displayed statistically significant differences (p < 0.05) between XDR and non-XDR strains. The detection rates for the efflux pump genes were as follows: cepA 52.9%, qacE 39.7%, qacEΔ1 35.2%, qacEΔ1-SUL1 52.9%, oqxA 30.8%, and oqxB 32.3%. The detection rate of the qacEΔ1-SUL1 gene in XDR CRKP strains was significantly higher than in non-XDR CRKP strains (p < 0.05). This indicates a potential link between CRKP bacterial disinfectant efflux pump genes and CRKP bacterial resistance patterns. Ongoing monitoring of the declining sensitivity of XDR strains against disinfectants is essential for the effective control and prevention of superbug.
Introduction
The global clinical use of carbapenem antibiotics has led to the identification and reporting of carbapenem-resistant Enterobacteriaceae worldwide.1,2 Klebsiella pneumoniae (KP), an opportunistic pathogen within the Gram-negative Enterobacteria group, frequently colonizes hospital environments, as well as the human gastrointestinal tract, skin, and nasopharynx, demonstrating a high transmission capability. 3 Research indicates that over 50% of patients treated for KP infections in certain regions show resistance to carbapenem antibiotics, largely due to the extensive and improper use of these drugs.4,5
Carbapenem-resistant KP (CRKP) can cause various nosocomial infections, particularly in immunocompromised individuals, including respiratory and urinary tract infections, bacteremias, and liver abscesses.6,7 Studies reveal that the fatality rate of CRKP infection ranges from 40% to 70%, which is two to three times higher than that of carbapenemase-sensitive KP infections.8,9 Furthermore, CRKP can develop resistance to numerous antibiotics, including carbapenems, potentially becoming extensively drug-resistant (XDR) bacteria, which is a leading cause of clinical treatment failure.10,11 According to the Centers for Disease Control and Prevention (CDC), XDR in Enterobacteriaceae is defined as nonsusceptibility to at least one agent in all but two or fewer antimicrobial categories. 12 The emergence of these bacteria limits antibiotic options for clinicians, resulting in poorer clinical outcomes, prolonged treatment cycles, and increased treatment costs.4,13 Zhen et al. reported that patients with XDR infections faced increased hospitalization costs of U.S. $4605–14252 and prolonged stays of 5.4–15.8 days, presenting significant challenges for clinical management. 14 Therefore, XDR-KP, derived from CRKP, requires increased attention and focus.
These bacteria, commonly found in hospital settings, make disinfection and sterilization essential for controlling their spread.15–17 Biocides, including antiseptics and disinfectants such as quaternary ammonium compounds (QACs), iodine preparations, chlorides, and ethanol, are widely used in hospitals to disinfect environments, medical equipment, and skin surfaces, playing a key role in preventing healthcare-associated infections.18–20
The frequent use of disinfectants has led to an increasing number of reports about drug-resistant bacteria developing resistance to commonly used clinical disinfectants, resulting in a rise in CRKP infection incidence overall. 21 This trend may be due to a gradual decrease in disinfectant sensitivity among CRKP strains, coupled with a growth in their resistance to these agents.22,23 The mechanisms behind antibiotic resistance and disinfectant resistance might be similar, with bacteria potentially developing antibiotic resistance through disinfectant induction. 24
Moreover, resistance to disinfectants can occur via inherent genetic transmission or the acquisition of exogenous mobile genetic elements. 25 Resistance genes on mobile genetic elements can spread the number and range of drug-resistant bacteria through horizontal transfer, which is a primary method by which bacteria develop resistance to disinfectants, such as qacE and cepA. 26 One study indicated that CRKP strains carrying the qacEΔ1-sul1 efflux gene show resistance to disinfectants containing benzalkonium bromide, suggesting that these genes can expel QACs. 27 The qacEΔ1 encoding system is mainly found in Gram-negative bacteria, where the genes can integrate into both plasmids and chromosomes. The detection rate of these genes is associated with resistance to quaternary ammonium disinfectants. 28 Additionally, other researchers have shown that qacEΔ1 and qacE affect bacterial sensitivity to iodophor disinfectants. 29 OqxA and oqxB, which belong to the resistance-nodulation cell division family, are also noteworthy. OqxAB, encoded by a plasmid, can efflux antimicrobial agents such as quinolones, tigecycline, and other antibacterial drugs, as well as QAC and biguanide disinfectants. 30
Furthermore, CRKP strains exhibit cross-resistance to disinfectants and antibiotics, indicating that increased bacterial resistance to antibiotics may reduce the efficacy of disinfectants. 31 This phenomenon of reduced bacterial susceptibility to disinfectants, and the potential connections between biocide and antibiotic resistance, is a relatively new and significant issue: it may lead to disinfection failures, complicating bacterial control. 32 Therefore, it is crucial to investigate whether XDR CRKP strains show higher resistance to commonly used chemical disinfectants. Disinfectant efflux pump genes also play a role in the widespread development of antibiotic resistance. 24 In some strains, integrons contain genes encoding antimicrobial resistance. 27 Gadea et al. found that Gram-negative Enterobacteriaceae resistant to disinfectants also showed decreased susceptibility to antibiotics such as ampicillin and cefotaxime, with the identified qac gene playing a key role in the development of strain resistance. 33 Some researchers also observed that Pseudomonas aeruginosa displayed significantly increased resistance to gentamicin and ciprofloxacin after exposure to sublethal concentrations of ciprofloxacin. 34 Talebi-Taher further confirmed that efflux pump expression in clinical Pseudomonas aeruginosa strains could affect their multidrug resistance. 35 However, the molecular basis of XDR CRKP strains remains poorly understood, especially due to the lack of scientific data from Xinjiang, China, posing a significant public health threat.
This study aimed to assess the disinfectant sensitivity of clinical CRKP strains, identify XDR CRKP strains through drug sensitivity testing, and explore the potential impact of antibiotic resistance on disinfectant resistance and its relationship with efflux pump genes. The goal was to reduce the risk of improper disinfectant use and the spread of drug-resistant bacteria in hospital settings.
Materials and Methods
Bacterial specimens
Sixty-eight CRKP strains were collected between February 2023 and June 2024 at the Fifth Affiliated Hospital of
Antibiotic susceptibility testing
The antimicrobial susceptibilities of the isolates to ertapenem, imipenem, piperacillin-tazobactam, amoxicillin-clavulanic acid, cefepime, ceftazidime, cefoxitin, ceftriaxone, amikacin, levofloxacin, colistin, and cotrimoxazole were tested using the Gram-negative susceptibility card on the Vitek system (BioMérieux, Marcy l’Etoile, France). The susceptibility to meropenem, aztreonam, gentamicin, ciprofloxacin, and tigecycline was tested using the Kirby–Bauer disk diffusion method. Antimicrobial susceptibility testing results were interpreted according to the criteria recommended by the CLSI. 36 Tigecycline testing criteria are in accordance with the standards set by the U.S. Food and Drug Administration. 37 XDR is defined as nonsusceptibility to at least one antibiotic in all categories but sensitive to ≤2 antimicrobial categories using criteria from the CDC. 12
Disinfectants
The study utilized four common clinical disinfectants: 0.1% benzalkonium bromide (Shanghai Macklin Biochemical Co., Ltd, Shanghai, China) as a low-efficiency disinfectant; 75% ethyl alcohol and 1% iodophor disinfectant (both from Beijing Xidebao Disinfection Products Co., Ltd, Beijing, China) as moderately effective disinfectants; and chlorine-containing disinfectants (Shandong Jiajie Water Purification Technology Co., Ltd, Shandong, China) as high-efficiency disinfectants.27,38
Detection of the MIC of disinfectants
The minimum inhibitory concentration (MIC) values of four disinfectants for 68 CRKP strains in this study were identified using the microbroth dilution method. A bacterial suspension with a standard concentration of 0.5 McFarland (108 CFU/mL) was utilized. Sterile distilled water was the negative control, and suspended broth served as the positive control. The MIC was recorded as the lowest disinfectant concentration where no bacterial growth was visibly detected. Each experiment was performed in triplicate.
Detection of the MBC of disinfectants
Samples from three successive wells starting at the MIC wells were transferred to Columbia blood culture plates and incubated at 35°C for 48 hours. The minimum bactericidal concentration (MBC) was defined as the minimum concentration of disinfectant that resulted in a sterile plate, indicating no bacterial growth. This experiment was repeated three times, yielding consistent results.
According to previous research criteria,27,28 strains with MIC and MBC values higher than those of standard strains were considered resistant to disinfectants, whereas lower values indicated sensitivity.
PCR detection of efflux pump genes
DNA templates from CRKP strains in this study were extracted using the boiling method. 29 Based on previous studies,27,39,40 the primer sequences for the efflux pump genes cepA, qacE, qacEΔ1, qacEΔ1-sul1, oqxA, and oqxB were listed in Supplementary Materials Supplementary Table S1and synthesized by Shanghai Sangon Bioengineering. The polymerase chain reaction (PCR) setup had a total volume of 25 μL. The PCR conditions were set with reference to published articles.27,39,40 The PCR amplification products were analyzed using 2% agarose gel electrophoresis and visualized under a UV imager. Positive controls were also included.
Statistical analysis
The data were analyzed using SPSS version 26. Frequencies and percentages were calculated for disinfectant efflux pump genes. The MIC and MBC data were analyzed using the Mann–Whitney test. The chi-square test was applied to determine the association between disinfectant efflux pump genes and increased antibiotic resistance. p-Values < 0.05 was considered statistically significant.
Results
Clinical data of CRKP strains
A total of 68 nonrepetitive CRKP strains were collected from clinical samples at the Fifth Affiliated Hospital of
Drug sensitivity test results
The 68 CRKP strains tested were insensitive to ertapenem, imipenem, and meropenem; this group included 21 XDR CRKP strains and 47 non-XDR strains. The resistance rates of the CRKP strains to piperacillin/tazobactam, ceftazidime, ceftriaxone, cefepime, levofloxacin, ciprofloxacin, and amoxicillin/clavulanic acid were 100% (68/68). The resistance rates to gentamicin and amikacin were 55.9% (38/68) and 50% (34/68), respectively, whereas the resistance rate to compound sulfamethoxazole was 35.3% (24/68). None of the 68 CRKP strains showed resistance to colistin. The susceptibility of five strains to tigecycline was categorized as intermediate, whereas six strains exhibited resistance to tigecycline, and the remaining strains were sensitive to tigecycline (Supplementary Table S2).
Sensitivity of clinical trial strains to disinfectants
The MIC ranges for 68 CRKP strains against alcohol, iodophor disinfectant, 0.1% benzalkonium bromide, and 2000 mg/L chlorine-containing disinfectant were 64–512, 128–1024, 128–1024, and 16–258 mg/L, respectively. The detailed MIC and MBC results for these strains against the four disinfectants are presented in Table 1.
Results of MIC and MBC of Disinfectant for Carbapenem-Resistant Klebsiella pneumoniae Strain (Unit of Measurement: mg/L)
MIC50 represents the MIC value required to inhibit the growth of 50% of the tested bacteria, and MIC90 represents the MIC value required to inhibit the growth of 90% of the tested bacteria. MBC50 represents the MBC value required to kill 50% of the tested bacteria, and MBC90 represents the MBC value required to kill 90% of the tested bacteria. MIC, minimum inhibitory concentration; MBC, minimum bactericidal concentration; CRKP, carbapenem-resistant Klebsiella pneumoniae; XDR, extensively drug-resistant.
*Indicates significant results (p < 0.05).
The MIC and MBC test results for the four clinical disinfectants were analyzed for two categories of CRKP strains: XDR and non-XDR. The results indicated that the MIC for 0.1% benzalkonium bromide differed significantly between extensively resistant and nonextensively resistant CRKP strains (p < 0.05). Significant differences were also observed in the MBC for benzalkonium bromide and the MBC for 1% iodophor disinfectant between the two groups (p < 0.05). The MIC and MBC for other disinfectants showed no statistically significant differences between the groups.
Disinfectant resistance genes
In this study, six disinfectant resistance genes were detected via PCR in 68 CRKP isolates. The prevalence rates for the genes cepA, qacE, qacEΔ1, qacEΔ1SUL1, oqxA, and oqxB were 52.9%, 39.7%, 35.2%, 52.9%, 30.8%, and 32.3%, respectively, with the cepA and qacEΔ1SUL1 genes being notably more common. Chi-square test analysis revealed that the detection rate of the qacEΔ1SUL1 gene in XDR CRKP strains was significantly higher than in non-XDR CRKP strains (p < 0.05), as detailed in Table 2 and Figure 1.
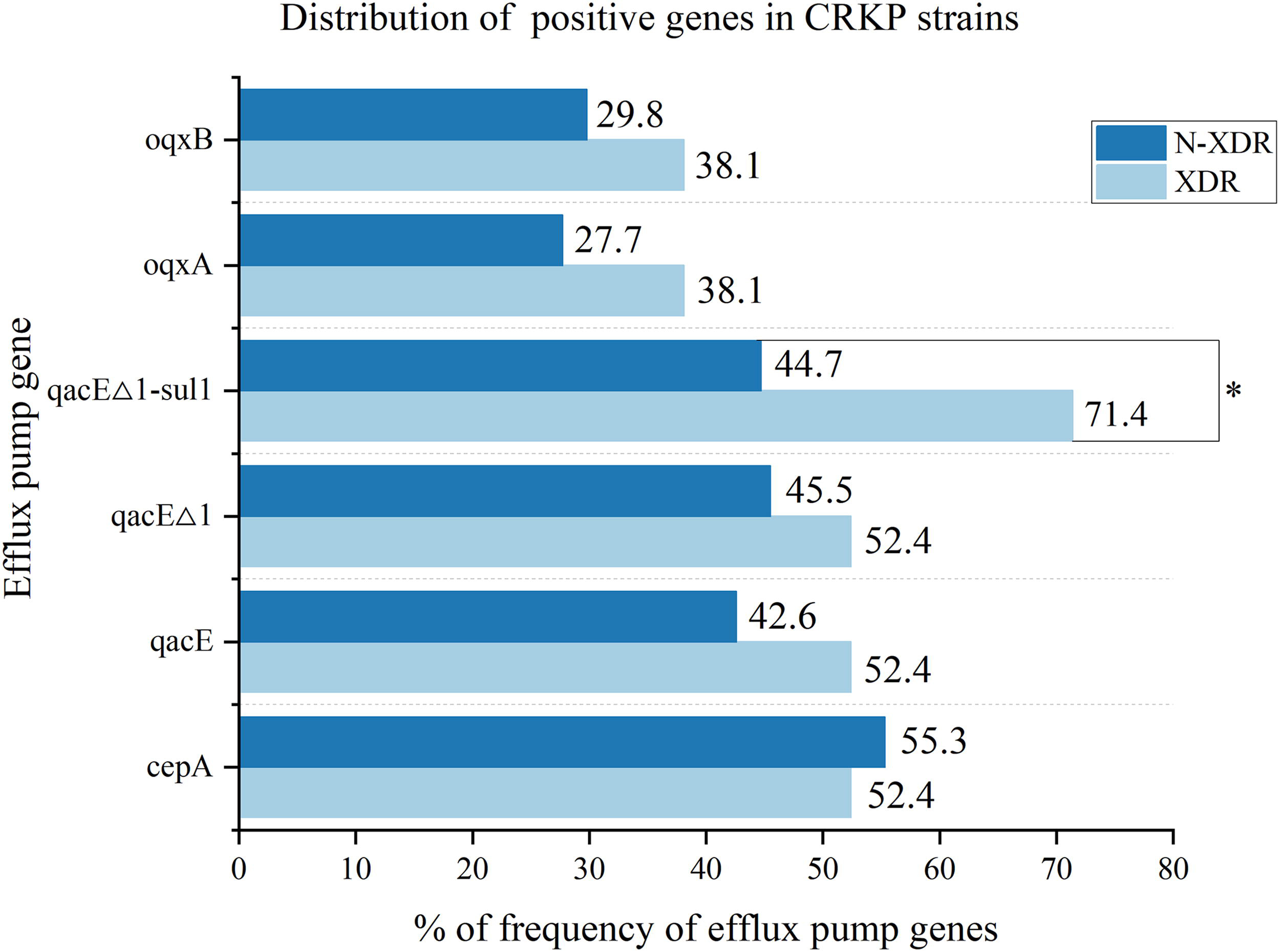
Distribution of positive genes in carbapenem-resistant Klebsiella pneumoniae strains.
Comparison of Distribution of Efflux Pump Genes
*Indicates significant results (p < 0.05).
Discussion
Resistance to CRKP is increasing annually, leading to higher medical costs and mortality rates, posing a significant public health threat. 41 According to the latest data from the China Antimicrobial Resistance Surveillance System, although the overall detection rate of CRKP in China slightly decreased in 2022, effective control has not been achieved in Xinjiang, where the detection rate increased from 5.7% in 2019 to 7.8% in 2022. 42
Among the 68 CRKP strains collected in this study, 58.8% were isolated from ICU wards, mainly from patients over 70 years old. This age distribution suggests that elderly patients in Xinjiang are at a higher risk of CRKP infection, which is consistent with findings from Chen et al.’s epidemiological study on Gram-negative Enterobacteriaceae. 43 The increased risk in elderly ICU patients may be due to their critical conditions and underlying comorbidities, which increase their susceptibility to colonization by drug-resistant bacteria and subsequent infections due to compromised immune function. 8 Sputum (61.8%) was the predominant sample type, indicating a likely prevalence of respiratory tract infections caused by CRKP in this region. In contrast, CRKP strains in the United States are primarily isolated from urine, 44 whereas studies in Africa report blood as the main source. 45 These differences highlight regional and population disparities in the sources of CRKP. 46
It is noteworthy that carbapenem resistance is often accompanied by resistance to several other key antimicrobial groups. 47 The study revealed that the 68 CRKP strains were nonsusceptible to ertapenem, imipenem, meropenem, piperacillin-tazobactam, amoxicillin-clavulanic acid, cefepime, ceftazidime, cefoxitin, ceftriaxone, levofloxacin, and ciprofloxacin, with most strains showing complete resistance. The resistance rates of XDR strains to amikacin, gentamicin, and cotrimoxazole were 66.7%, 76.2%, and 95.2%, respectively, compared with 42.6%, 46.8%, and 8.5% for non-XDR strains. El Badawy et al.’s study demonstrated that all clinically isolated CRKP strains were resistant to cephalosporins. 48 A study in Qingdao found the resistance rate of CRKP to amikacin to be the lowest, whereas it exceeded 90% for meropenem and cefepime, 49 similar to the findings of this study. However, a study from Portugal showed the greater effectiveness of cephalosporins against isolates, with resistance rates of only 40.2% and 68.6%, respectively. 47 Additionally, Zhu et al.’s results indicated a 11.9% resistance rate of CRKP strains to colistin, higher than in this report, likely due to different patient conditions and clinical treatments involving multiple types of antibiotics. 50 High resistance in CRKP strains is associated with combinations of drugs, antibiotic misuse, subjective medication practices, unsystematic medication planning, and delayed monitoring, especially in low- and middle-income countries. 11 This significantly limits the selection of effective antibiotics in clinical treatments, placing considerable pressure on managing CRKP infections. 51 Despite the introduction of new pharmaceuticals for treating CRKP infections, these measures are insufficient to counter the rising prevalence of drug-resistant bacteria. 52 Thus, disinfection and sterilization remain crucial in controlling hospital-acquired infections. 53
The results of this study indicated the highest resistance to chlorine-containing disinfectants, followed by iodophor, with the lowest resistance observed against benzalkonium bromide. The effectiveness of sterilization in controlling hospital infections seems to be decreasing, particularly due to the widespread and routine use of disinfectants. 54 Research as early as 1952 showed that bacteria could develop resistance to disinfectants in a manner similar to antibiotics, with subsequent observations of resistance to biguanides, phenols, alcohols, and iodine. 55 Extensive use of disinfectants has exposed CRKP strains to high concentrations over prolonged periods, potentially reducing their susceptibility to commonly used disinfectants and increasing their ability to spread within hospital settings. 56 Despite varying degrees of resistance among the CRKP strains in this study, the MICs of disinfectants were below the levels typically prescribed by hospitals. MICs provide a useful reference for disinfectants when used to prevent microbial multiplication and reduce viability to acceptable levels. 57 Therefore, the effectiveness of disinfectants can still be maintained in hospital environments by selecting appropriate types and adhering to recommended concentrations for sterilization.
In this study, the MIC values for non-XDR strains were primarily 256 and 512 mg/l, whereas those for XDR strains were mostly ≥512 mg/l. This difference may be due to bacterial cross-resistance to both antibiotics and disinfectants. XDR strains have developed elevated resistance levels to disinfectants, posing significant challenges in controlling the spread and transmission of resistant bacteria. 58 In addition, this study found that the sensitivity of benzalkonium bromide and 1% iodophor disinfectants differed between XDR and non-XDR CRKP strains. Increased disinfectant resistance in CRKP strains may induce the expression of efflux pump genes, leading to cross-resistance to antibiotics. 59 Monarrez et al. 60 reported that the qacE efflux pump gene in Escherichia coli from Nigeria was located on the 125 Kb autobiotic IncFII plasmid pMB2, which also carried the blaCTX-M-15 gene mediating resistance to cephalosporins.
However, the issue of cross-resistance caused by disinfectants and antibiotics remains controversial, with varied research outcomes.61,62 For instance, a study on cross-resistance mechanisms in Listeria monocytogenes in Germany 63 found no evidence of a link between bacterial resistance to disinfectants and the presence of disinfectant resistance genes and antibiotic resistance. In addition, Cottell et al. 64 reported that increased resistance to triclosan did not correlate with increased antibiotic resistance; instead, they found that E. coli with increased resistance to triclosan were more susceptible to aminoglycoside antibiotics. This highlights the importance of conducting detailed molecular-level studies to fully understand the interactions between these resistance mechanisms. Simultaneously, it is crucial for clinical staff to strictly adhere to specified disinfectant concentrations to prevent bacterial cross-resistance, which can result in incomplete sterilization and an increased risk of spreading drug-resistant bacteria within the hospital environment. 32
In this study, the detection rates of disinfectant efflux pump genes in XDR and non-XDR CRKP strains were compared. The detection rate of cepA reported by Abuzaid et al. 39 was higher than that of this study, which was 87.5%. In a Chinese study, 65 the detection rates for cepA and qacEΔ1 were 93.2% and 64.9%, respectively. Other studies have also reported significantly higher detection rates for oqxA, oqxB, and qacEΔ1-sul1 compared with those in this study. 27 Conversely, Jin et al. found lower detection rates for cepA and qacEΔ1 than our findings. 66 The variability in detection rates of efflux pump genes may be influenced by factors such as geographical region, strain diversity, type of disinfectant, and sample size. 67 Therefore, it is essential to improve the monitoring of disinfectant efflux pump genes locally and improve the supervision system for disinfection prevention and control, ensuring medical and health personnel use disinfectants appropriately.
This study suggests that qacEΔ1SUL1 may play a role in mediating bacterial cross-resistance. The qacEΔ1 gene is located at the 3′ conserved terminus of the Class I integron and typically encodes antibiotic resistance genes, which could explain its association with sulfonamide-resistant genes. 40 Furthermore, as a plasmid-mediated disinfectant efflux pump gene, qacEΔ1 has been shown to confer simultaneous resistance to disinfectants and various antibiotics such as gentamicin, penicillin, and sulfonamides. 68 Previous studies by Hu et al. 58 have shown that disinfectants can promote the development of cross-resistance to antibiotics by inducing qacEΔ1 and other disinfectant resistance genes, thereby increasing the spread of antimicrobial resistance, particularly during the COVID-19 pandemic, which aligns with the findings of our study. Another study indicated a close association between the disinfectant efflux pump gene cepA and antibiotic resistance in Enterobacteriaceae strains. 39 However, in our study, while isolates containing the cepA gene exhibited higher drug resistance compared with those without it, this difference was not statistically significant. This may be due to the limited sample size or geographical factors, but it could still hold clinical significance. Amsalu et al. 59 conducted a comparative analysis of cross-resistance between antibiotics and disinfectants in strains isolated from various ecological niches. Their findings suggest that bacteria can induce the overexpression of efflux pump genes through gene mutations, leading to concurrent resistance to multiple antibiotics and disinfectants.
Conclusion
The study revealed a significant correlation between the resistance of CRKP strains to both antibiotics and disinfectants, with extensively resistant CRKP strains showing increased resistance to commonly used disinfectants. The mechanism of cross-resistance is associated with disinfectant efflux pump genes, which are primarily found in extensively resistant CRKP strains. Therefore, regular monitoring of disinfectant and antibiotic resistance levels in hospital environments is crucial. However, due to the limited sample size, the study could not determine the involvement of other efflux pump genes in cross-resistance between disinfectants and antimicrobials. Controlling HAIs remains a significant and ongoing challenge, necessitating further research into cross-resistance mechanisms to provide empirical data for the strategic combined use of antibiotics and disinfectants, as well as for developing more effective prevention and control strategies against drug-resistant bacteria.
Footnotes
Acknowledgment
We thank the Fifth Affiliated Hospitals of Xinjiang Medical University for providing the data.
Authors’ Contributions
Conceptualization: K.Z., J.D., and P.T. Data curation: K.Z., Q.Z., and L.W. Formal analysis: K.Z., J.D., P.T., and L.W. Methodology: M.A., X.W., and Z.D. Writing original draft: K.Z., J.D., Q.Z., M.A., X.W., Z.D., and P.T. Writing-review and editing: K.Z., L.W., J.D., Q.Z., M.A., X.W., Z.D., and P.T. All authors reviewed the article.
Availability of Data and Materials
The datasets generated and/or analyzed during this study are confidential and not publicly available but may be obtained from the corresponding author upon reasonable request.
Consent for Publication
All authors have consented to publication.
Disclosure Statement
The authors declare no competing interests.
Funding Information
This work was supported by the Natural Science Foundation of the Xinjiang Uygur Autonomous Region (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.