
Abstract
Background:
Metabolic syndrome has the highest prevalence among Mexican-American women. Little information is available for Caribbean Hispanics, the largest and fastest growing ethnic minority in the United States. We sought to evaluate the frequency of metabolic syndrome and its relationship with race/ethnicity, socioeconomic position, and education in women of largely Caribbean Hispanic origin.
Methods:
There were 204 women enrolled in a cross-sectional study who had demographics, fasting glucose, lipid profile, waist circumference, and blood pressure determined. Metabolic syndrome (defined by the National Cholesterol Education Program/Adult Treatment Panel III [NCEP/ATP III]) was analyzed using univariate and multivariate logistic regression to test age, race/ethnicity, education, health insurance, and residence on the risk of metabolic syndrome. A P value <0.05 was considered significant.
Results:
Mean age was 58 ± 11 years, Hispanic 44.1% (93% Caribbean), non-Hispanic white (NHW) 38.7%, and non-Hispanic black 9.8%. Education was some high school (<HS) 33.7%, HS graduate 11.2%, some college 12.9%, college graduate 10.1%, and postgraduate 32%. Health insurance was Medicaid 47.8% and commercial 52.2%. Area of residence was urban 77.1% and suburban 22.9%. The frequency of metabolic syndrome was 42.4%, and was increased in Hispanic women (63.3%) versus NHW (29.6%), women with <HS (72.6%) versus postgraduate education (32.1%), women with Medicaid (57.9% vs. 27.4%) and urban residence (47.5% vs. 27.2%). For all comparisons, P < 0.05. Education <HS was linked to increased risk of metabolic syndrome (odds ratio [OR] = 3.5 [1.2–10.0], P = 0.02). Hispanic women had the lowest level of education (P < 0.001) and the highest frequency of individual metabolic syndrome components (P < 0.01).
Conclusions:
Metabolic syndrome showed an alarming rate in less educated Caribbean Hispanic women and was independently associated with lower education level.
Introduction
CVD is the leading cause of death among women and Hispanics. 9 Hispanics have surpassed other racial and ethnic groups to become the largest and fastest growing U.S. minority, numbering an estimated 42.7 million people in 2007 10 and projected to increase to 96.5 million (24% of the population) by 2050. 9
Cardiovascular risk factors such as metabolic syndrome, obesity, and diabetes have an alarming prevalence among Hispanics. 10 Using the Adult Treatment Panel III (ATP III) definition of metabolic syndrome, the age-adjusted prevalence of the metabolic syndrome in U.S adults is 24% in men and 23.4% in women, with >40% of the elderly affected. 11 –13 It is highest among Mexican Americans (31.9%) and lowest among whites (23.8%), African Americans (21.6%), and people reporting “other” as race or ethnicity (20.3%), with Mexican-American women having a higher prevalence than men. Little information is available for other Hispanic subgroups. 14 While Mexican Americans currently represent the majority of Hispanics in the United States, Caribbean Hispanics are a major subgroup of relatively recent immigrants from the Caribbean Islands, including the Dominican Republic, Cuba, and Puerto Rico. They are the fastest growing ethnic group in the northeastern United States. 9,10,15 The majority of the northern Manhattan Hispanic community is of Caribbean origin, thus providing a unique opportunity for the study of cardiovascular risk in Caribbean Hispanic women.
The objectives of the study were to: (1) characterize the frequency of metabolic syndrome and its individual components in Hispanic women of Caribbean origin, and (2) evaluate the potential relationships between education, socioeconomic position, race/ethnicity, and components of metabolic syndrome in women from a representative sample of this minority.
Methods
Sample
Women from Washington Heights–Inwood, northern Manhattan, and the tristate area of New York, New Jersey, and Connecticut were enrolled in a cross-sectional study approved by the Columbia University Institutional Review Board. Subjects were referred by their primary care physicians and signed consent forms. Medical histories and physical exams, which included assessment of waist circumference and blood pressure, as well as standardized questionnaires adapted from the Behavior Risk Surveillance Study were obtained. 16 Additionally fasting plasma glucose levels and lipid profiles (total cholesterol, low-density lipoprotein cholesterol [LDL-C], high-density lipoprotein cholesterol [HDL-C], triglycerides) were obtained at the time of enrollment.
Measures
Metabolic syndrome
Metabolic syndrome was defined using ATP III 17 criteria which requires at least three of the following criteria: waist circumference >88 cm (>35 in), fasting plasma glucose ≥100 mg/dL, triglyceride level of ≥150 mg/dL, HDL-C <50 mg/dL, and blood pressure reading of systolic ≥130 or diastolic ≥85 mmHg.
Race/ethnicity
Race and ethnicity were defined by self-identification based on a series of interview questions modeled after the U.S. census. 18 Data from racial and ethnic groups other than non-Hispanic whites, non-Hispanic blacks, and Hispanics were collected but excluded from analysis involving race/ethnicity because the sample size was small.
Education
Education was categorized as: Never attended school, attended only kindergarten, attended grades 1 through 8 (elementary), grades 9 through 11 (some high school), grade 12 or General Education Development test (GED) (high school graduate), college 1 year to 3 years (some college, vocational, or technical school), college graduate, or postgraduate (>4 years college).
Geographic area of residency
Suburban or urban geographic area of residency was determined.
Health insurance status
Health insurance status was categorized as Medicaid or state, Medicare, health maintenance organization (HMO), commercial, private, none, or other.
Perceptions related to heart disease and stroke
Participants were provided with a standardized interviewer-assisted questionnaire about demographic information and asked open-ended questions regarding the leading cause of death among women, warning signs of heart attack and stroke, and the action to take if experiencing a heart attack or stroke. These questions evaluate the goals established by Healthy People 2010 (Chapter 12, Heart Disease and Stroke, 12.2 & 12.8) to improve cardiovascular health and quality of life through the prevention, detection, and treatment of risk factors; early identification and treatment of heart attacks and strokes; and prevention of recurrent cardiovascular events. 19
Framingham Risk Score
Low-, moderate-, and high-risk status were defined as <10%, 10–20%, and >20% probability of coronary heart disease in 10 years, based on the Framingham risk algorithm. 20 Those with diabetes were assigned to high-risk status.
Statistical analyses
The results are reported as means and standard deviations for continuous variables and as frequencies for categorical variables. The significance of differences in mean values between those with and without metabolic syndrome was assessed by t-test. The Fisher exact test or chi-squared tests were used to determine the significance of the association of metabolic syndrome with categorical variables. Univariate and multivariable logistic regression analysis was used to test the effect of age, race/ethnicity, education, insurance, and location of residence on the OR for metabolic syndrome. A P value <0.05 was considered significant for all analyses.
Results
There were 204 females enrolled (Table 1). The presence of metabolic syndrome could be determined in 184 (90%) subjects and could not be defined in 20 of the 204 subjects due to one or more missing components of metabolic syndrome. Among the remaining 184 subjects, 75 subjects (42.4%) had three or more components of metabolic syndrome. Of the remaining 109 subejcts (57.6%), 23.4% had two components, 20.1% had one component, and 14.1% had no components of metabolic syndrome.
The presence of metabolic syndrome could not be determined for 20 of the 204 subjects due to one or more missing components.
Abbreviations: MS, metabolic syndrome; SD, standard deviation.
Age and metabolic syndrome
The mean age was 58 ± 11 years. There were no significant differences in the frequency of metabolic syndrome among age groups.
Race-ethnicity and metabolic syndrome
The race-ethnicity breakdown was predominantly Hispanic, followed by non-Hispanic white (NHW), non-Hispanic black (NHB), and other. Among Hispanics, 92.9% were of Caribbean origin. Compared to NHW, the frequency of metabolic syndrome was greater in Hispanics but not in NHB (Table 1).
Educational level and metabolic syndrome
Education was <HS 33.7%, high school graduate 11.2%, some college 12.9%, college graduate 10.1%, and postgraduate 32.0%. Educational level was related to metabolic syndrome with greater frequency in subjects whose level of education was <HS compared to those with postgraduate education (Table 1).
Health insurance, area of residence, and metabolic syndrome
All subjects had health insurance including Medicaid and HMO or other commercial. The area of residence was predominantly urban. The frequency of metabolic syndrome was significantly increased in women with Medicaid and in those living in urban areas (Table 1).
Multivariable logistic regression was used to assess the relationship between metabolic syndrome and age, race-ethnicity, educational level, health insurance, and area of residence. In this analysis only educational level lower than high school was independently related to metabolic syndrome (OR = 3.5, 95% confidence interval [CI] 1.2–10.0, P = 0.02).
Among Hispanics, <HS education was related to metabolic syndrome (P = 0.04). There were too few women with low educational levels in NHW and NHB to analyze the educational effect separately in these race/ethnic groups.
Metabolic syndrome components
The most frequent abnormal criteria were waist circumference >88 cm (>35 in) (68.6%) and elevated blood pressure (54.8%) with 52.5% having a systolic blood pressure of ≥130 mmHg and 31.8% having a diastolic blood pressure of ≥85 mmHg.
Among all races/ethnicities, the frequencies of abnormal waist circumference, HDL-C, triglycerides, and fasting plasma glucose among Hispanics were greater than for NHW (all P < 0.01) (Table 2A). NHB women showed lower frequencies of elevated blood pressure, high triglyceride, and high glucose levels compared to NHW, but these were not statistically significant. Among women with metabolic syndrome, only elevated fasting glucose differed by race/ethnicity, with a significantly higher rate among Hispanics than NHW (83.7% vs. 50.0%, P = 0.006).
Abbreviations: CI, confidence interval; NHW, non-Hispanic white; NHB, non-Hispanic black; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; SPB, systolic blood pressure; DBP, diastolic blood pressure.
Among subjects with the lowest level of education, the frequencies of low HDL-C, high triglycerides, fasting plasma glucose, and increased waist circumference were significantly greater than those with the highest level of education. (Table 2B).
Abbreviations: CI, confidence interval; <HS, some high school or less; HSG, high school graduate; SC, some college; CG, college graduate; PG, postgraduate; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; SPB, systolic blood pressure; DBP, diastolic blood pressure.
Framingham Risk Score and metabolic syndrome
Among those with metabolic syndrome, 23.1% had a calculated 10-year risk for coronary heart disease of <10% (low), 3.9% had a risk of 10–20% (intermediate), and 73.1% had a risk of >20% (high). This is in contrast to those without metabolic syndrome, where a significantly higher proportion was at low risk (61.5%) or intermediate risk (5.8%) and a lower proportion was at high risk (32.7%), (P < 0.0001) (Fig. 1). Hispanic women with metabolic syndrome were more likely than their NHW and NHB counterparts to have a higher Framingham Risk Score (FRS) (Table 3).
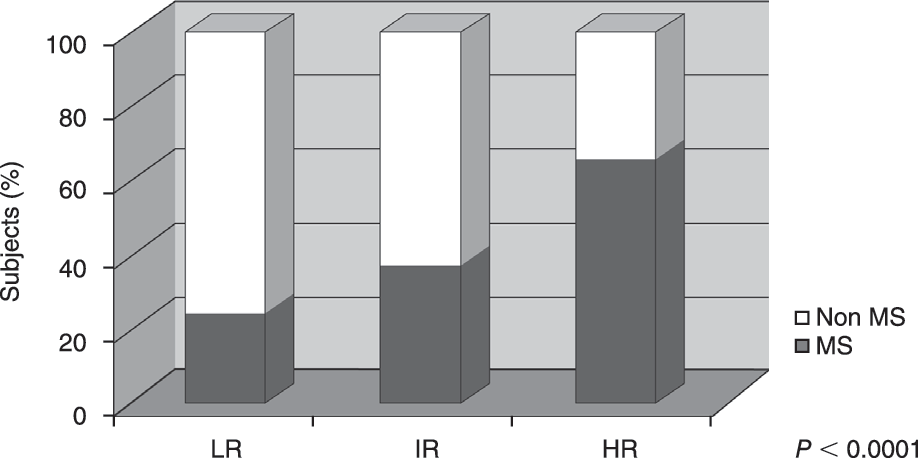
Framingham Risk Score and metabolic syndrome. Among subjects with metabolic syndrome, 23.1% had a calculated 10-year risk for coronary heart disease of <10% (low), 3.9% had 10-year coronary heart disease risk of 10–20% (intermediate), and 73.1% had 10-year coronary heart disease risk of >20% (high). This contrasts with those without metabolic syndrome where a significantly higher proportion was at low risk (61.5%) or intermediate risk (5.8%) and a lower proportion was at high risk (32.7%). Abbreviations: LR, low-risk; IR, intermediate risk; HR, high-risk; Non MS, non-metabolic syndrome; MS, metabolic syndrome.
Abbreviations: CI, confidence interval; NHW, non-Hispanic white; NHB, non-Hispanic black; FRS, Framingham Risk Score.
Perceptions related to heart disease and stroke
Responses to the questions related to knowledge about heart disease and stroke were obtained in 122 women. Awareness that heart disease is the leading cause of death among women was lower among Hispanics compared with NHW (41.3% vs. 93.8%, P < 0.0001) (Fig. 2). Awareness among NHB (81.8%) was not significantly different from NHW (P = not significant [N.S.]). Educational level <HS was also associated with lower frequency of awareness (37.0%) compared with those with a college education or greater (86.7%), P < 0.0001. Similar disparities related to race/ethnicity and education were found for warning signs of heart attack and stroke. However, >90% of all race/ethnic and educational groupings were aware of the action to take if experiencing a heart attack or stroke (P = N.S. for all comparisons).

Awareness related to heart disease and stroke and race/ethnicity. Awareness that heart disease is the leading cause of death among women was lower among Hispanics compared with NHW. Awareness among NHB was not significantly different from NHW. Similar disparities were found for warning signs of heart attack and stroke. Abbreviations: NHW, non-Hispanic white; NHB, non-Hispanic black; H, Hispanic. Question 1, Cardiovascular disease is the leading cause of death among women; Question 2, Warning symptoms and signs of heart attack and stroke.
Discussion
Findings in this report demonstrate a strong association between metabolic syndrome and low education independent of age, race/ethnicity, insurance, and location of residence and, moreover, add new information, specifically relevant to Caribbean-Hispanic women.
Frequency and components of metabolic syndrome by race/ethnicity
The age-adjusted prevalence of metabolic syndrome was recently found to be 23.7% among 8814 U.S. adults participating in the National Health and Nutrition Examination Survey III (NHANES III). 21 The prevalence of this syndrome varies among different race/ethnic groups. 11,22 –25 Hispanics had the highest age-adjusted prevalence (31.9%), probably linked to a higher prevalence of obesity. 26 In our study, metabolic syndrome in women varies among race/ethnic groups, ranging from 21% in NHB to 63% in Hispanics.
The frequency of metabolic syndrome was not related to age and was higher than previously reported for other populations. 12,22 –24,27 However, some of these differences might arise from variations in the definition of metabolic syndrome used in each study. Our patients were recruited from a single tertiary institution, and the high frequency observed may not truly represent the metabolic syndrome community in general.
The most frequent abnormal criteria for metabolic syndrome were waist circumference >88 cm (>35 inch) and elevated blood pressure. Waist circumference >88 cm was present in 69% of subjects in this study; this measure is well correlated with visceral adipose tissue and is a better anthropometric predictor of metabolic risk factors than body mass index. 12 Given the known relationship between metabolic syndrome and abdominal obesity, 28 this was a key difference that likely influenced the risk for the other four factors.
The frequency of elevated blood pressure was 55%, with a majority of subjects exhibiting abnormal systolic blood pressure and approximately one third exhibiting elevated diastolic blood pressure. It has been reported that about half of the patients with hypertension have insulin resistance and hyperinsulinemia. Studies suggest that hypertension is an important factor in the overall development of the phenotype “metabolic syndrome,” with underlying “insulin resistance” as an etiology. 29
The frequency of subjects reporting a history of diabetes mellitus and current diabetes medication use was 50%, possibly due to most people with diabetes having type 2 diabetes and metabolic syndrome.
When individual components of metabolic syndrome were analyzed, differences were found among ethnic groups. Lower prevalence of metabolic syndrome in NHB women was accompanied by lower frequencies of elevated triglyceride levels and blood glucose levels, similar to other reports. 30 Noteworthy, among Hispanics the frequencies of abnormal waist circumference, low HDL-C, high triglycerides, and elevated fasting plasma glucose were all greater than for NHW. Our findings are consistent with studies that demonstrate that compared with NHW; Hispanics are more prone to develop hyperinsulinemia, insulin resistance, and an unfavorable distribution of body fat, which are the central features of metabolic syndrome. 31
Metabolic syndrome, Framingham Risk Score, and race/ethnicity
A wide spectrum of estimated risk of coronary heart disease exists in U.S. adults with metabolic syndrome. About one third of metabolic syndrome subjects are at high risk of coronary heart disease and approximately one half are at 10% or greater risk. 32 These findings coincide with our study. Interestingly Hispanic women with metabolic syndrome were more likely than their NHW and NHB counterparts to have higher FRS (P < 0.0001). The highest elevated fasting plasma glucose among Hispanic women could be responsible for the difference in FRS among metabolic syndrome women of different race/ethnicity. However, among Hispanics with metabolic syndrome, 34 of 47 (72%) had <HS education and all 34 had high FRS. Unfortunately, there were too few women with metabolic syndrome and <HS education among NHW and NHB to allow for a multivariate analysis of race/ethnicity and educational level.
Metabolic syndrome, socioeconomic position, and race/ethnicity
Adult socioeconomic position is typically measured as educational attainment, income, or occupation. Educational level is one of the most commonly used proxies for socioeconomic position 33 because it is simple to collect, associated with a high response rate, minimally affected by later health status, and remains relatively constant. Low socioeconomic position measured by education links CVD with major individual risk factors 34 –36 and metabolic syndrome. 37 Therefore, we investigated whether metabolic syndrome was significantly linked to race-ethnicity and variables related to socioeconomic position including education, the subject's health-care provider, and area of residency.
The frequency of metabolic syndrome was greater in Hispanics, those with a level of education <HS compared to those with postgraduate education, subjects with Medicaid and those living in an urban area of residence (Table 1). Using multivariable logistic regression, only <HS education was an independent predictor of increased frequency of metabolics syndrome (OR = 3.5, 95% CI 1.2–10.0, P = 0.02). This finding suggests that the higher frequency of metabolic syndrome in Hispanics may reflect a diminished socioeconomic position and lower educational attainment. Furthermore, a low level of education was significantly related to four of the individual metabolic syndrome components. As previously shown, 38 we found that low HDL-C, high triglycerides, high fasting glucose, and increased waist circumference were strongly associated with lower educational level.
Consistent with our data, others 38,39 found that metabolic syndrome is significantly related to low levels of education in women. However, little is known concerning education and metabolic syndrome in Caribbean Hispanics women.
Washington Heights–Inwood in northern Manhattan encompasses approximately 270,000 individuals, composed of 71% Hispanic (primarily Caribbean Hispanic), 14% African American, 11% white, and 2% other. Women represent 65% of the population and African-American and Hispanic women account for 80% of that group. This population has a lower average household income ($30,726), greater numbers of people with less than a high school education (40.4%), more poverty (31.4%), and fewer managerial and professional workers (13.9%) than New York City overall. 40
Several associations between education and metabolic syndrome in Caribbean Hispanic women of this community may account for our findings. First, low levels of education in women may be a marker for characteristics associated with increased risk for metabolic syndrome, such as access to and retrieval of health information. Second, neighborhood characteristics are a potential mechanism linking education to metabolic syndrome. 41,42 Persons living in neighborhoods with fewer recreational activities, more fast food restaurants, and billboard advertisements for fast food are influenced by the environment. 43 These structural differences may predispose residents to participate in metabolic syndrome-inducing behaviors. A third mechanism is related to findings that women with low education level have additional psychosocial risks (income under the poverty threshold, unemployment, and single parenting), which may be associated with poorer metabolic outcomes. 44 A fourth potential explanation is that minority women may not perceive the value of obtaining early preventive health care. In our study, the lack of awareness of heart disease as the leading cause of death among women and the warning signs of heart attack and stroke were associated with lower level of education, which was lower among Hispanic women compared with NHW. Lack of knowledge and awareness of CVD may contribute to disproportionately low use of health-care resources and therefore contribute to the higher risk observed in Hispanic women. 45 It is alarming that while the majority of Hispanic women recognized chest pain as a heart attack symptom, more than half of the respondents failed to recognize less typical symptoms of a heart attack and stroke. Because women are more likely to present with atypical symptoms, failing to recognize these as heart attack symptoms may be an important contributor to delays in treatment for Hispanic women. Our observations are unique because few have examined heart attack and stroke symptom awareness among adult Caribbean Hispanic women, a group at high risk for delays in treatment. 46
In summary, Caribbean-Hispanic women in this population have: (1) the highest frequency of metabolic syndrome, (2) the highest risk of coronary heart disease as assessed by the Framingham Risk Score and, (3) the lowest level of education.
The association between metabolic syndrome, risk of coronary heart disease risk, and education raises a “red flag” to alert the health-care community of the limitations in our knowledge of this community. Despite the strength of our observations, it is not clear if addressing the observed educational gap or if reducing metabolic syndrome will be effective in reducing risk in terms of cardiovascular health outcomes. However, the findings here are evidence that raising alertness, while exploring the even greater issue of health outcomes, is important.
Study limitations
This study has limitations that should be taken into consideration. First, this was a cross-sectional design and cause and effect cannot be determined. Second, self-reported information was analyzed and is subject to recall bias. Third, there may be racial/ethnic and cultural barriers to health-care services that could have affected the likelihood of screening and diagnosis for high cholesterol, diabetes, or high blood pressure leading to underestimates in the NHB and Hispanic subjects. Fourth, the study did not take into account other factors such as income levels or having a primary care provider that might influence knowledge and treatment-seeking behavior. Fifth, dietary habits, exercise, and family history of diabetes or heart disease could not be precisely documented, which may might predispose subjects to participate in metabolic syndrome-inducing behaviors. Last, a limited geographic region of northern Manhattan and its surrounding suburbs was evaluated; hence, a larger geographic area and increased sample size is desirable to make recommendations for interventions in other populations.
Conclusion
In summary, a troubling rate of metabolic syndrome within Hispanic women living in northern Manhattan and a clustering of the clinical features of metabolic syndrome proved to be independently associated with lower education level.
Footnotes
Acknowledgments
This study was supported by the Office of Women's Health, Department of Health and Human Services (HHCWH050003), the New York Presbyterian Hospital Auxiliary of the Columbia University Medical Center, the Arlene and Joseph Taub Foundation, the Norman and Rosita Winston Foundation, and the Avon Foundation.
Author Disclosure Statement
No competing financial interests exist.