
Abstract
Background:
Obesity, metabolic syndrome, and atherosclerosis are linked with an increased acute-phase response. Severe periodontal disease is associated with cardiovascular disease as sequelae of a systemic inflammatory response.
Objective:
The aim of this study was to assess changes in measures of systemic inflammation induced by periodontal therapy in periodontally diseased individuals with metabolic syndrome, compared to those induced in a systemically healthy group.
Methods:
A total of 31 subjects with chronic generalized periodontitis, including 16 subjects with metabolic syndrome (group A) and 15 systemically healthy subjects (group B), underwent nonsurgical periodontal therapy. Serum high-sensitivity C-reactive protein (hsCRP), total leukocyte count, and measures of lipid metabolism were measured at baseline and at 2 months after periodontal therapy. Baseline data for comparison was also obtained from 15 systemically and periodontally healthy individuals (group C).
Results:
Baseline periodontal parameters and serum CRP were significantly higher in group A than in group B. In group A, following periodontal therapy, a significant decrease was noted in mean serum CRP (3.28 ± 1.4 mg/L to 2.6 ± 1.5 mg/L), total leukocyte counts (8,322 ± 1,888 cells/mm3 to 6,361 ± 1,426 cells/mm3), serum triglycerides (153.3 ± 38 mg/dL to 121.0 ± 28.57mg/dL), along with a significant rise in serum high-density lipoprotein (HDL) (41.1 ± 5.2 mg/dL to 44.37 ± 6.7 mg/dL). In group B, changes in these parameters were not statistically significant. Mean serum low-density lipoprotein (LDL) and mean cholesterol levels did not change significantly in either group.
Conclusions:
Periodontal therapy produced significant modulation of serum hsCRP, total leukocytes, serum triglycerides, and HDL, and thus may benefit individuals affected with both metabolic syndrome and advanced periodontal disease.
Introduction
Methods
Study population
A total of 46 individuals participated in the study. The study protocol and data collection methods were approved by Institutional Ethics Committee, and informed consent was obtained from all subjects. Inclusion criteria were age within 40–60 years and presence of at least 20 teeth. Exclusion criteria included smoking, history of periodontal therapy within 3 years, statin intake or intake of medication likely to alter serum inflammatory markers, and any systemic disorder other than metabolic syndrome.
Oral examination
A full mouth periodontal examination was conducted and comprised of probing pocket depth (PPD), cinical attachment loss (CAL), and bleeding on probing (BOP) recorded at six sites at all teeth present. Subjects were grouped according to their periodontal status. Periodontal disease was quantified, taking into account both extent and severity 14 by recording data for extent of sites with attachment loss of 3 mm or more and probing depth of 5 mm or more, which was categorized as 0% (no disease), 0%–10% (moderate disease), and more than 10% (severe disease) of the sites.
Systemic examination
A questionnaire relating to systemic health status and medications was completed by the selected participants at baseline visit. Waist circumference and BMI were measured. Blood pressure was evaluated three times, at 5-min intervals. Serum triglycerides and plasma glucose were assayed. Serum high-density lipoprotein (HDL), low-density lipoprotein (LDL), total cholesterol, and trigycerides were measured by standard enzymatic methods. Diagnosis of metabolic syndrome was made in participants exceeding the threshold limits for at least three of these following components: Central obesity (waist circumference >102 cm for males and >88 cm for females); hypertriglyceridemia (triglycerides >150 mg/dL); low HDL-cholesterol (C) (<40 mg/dL for men and <50 for women); high blood pressure (systolic, >130 mmHg; or diastolic, >85 mmHg or on blood pressure medication); and high plasma glucose (>110 g/dL). 15
Subject stratification
Subjects were grouped as follows: Group A comprised 16 subjects with moderate to severe periodontal disease and metabolic syndrome. Group B comprised 15 individuals with moderate to severe periodontal disease, but no evidence of metabolic syndrome. Group C, the control group, comprised 15 systemically healthy subjects with no periodontal disease.
Blood analysis
Total leukocyte count was assessed by standard clinical laboratory methods. Serum CRP level was assessed by a high-sensitivity latex agglutination immunoassay, using a commercially available kit, Puretao S CRP Latex (SS type).
Periodontal treatment
Patients in Groups A and B received nonsurgical periodontal therapy. Supragingival scaling was followed by thorough subgingival debridement. Scaling and root planing under local anesthesia was carried out using ultrasonic scalers and hand instruments, over two to four visits. Oral hygiene instructions were provided. Subjects were reassessed 2 months after completion of treatment. Clinical periodontal parameters were recorded and blood analysis was repeated.
Data analysis
Baseline demographic data were compared using a t-test for normally distributed variables and chi-squared test for categorical variables. Clinical and hematological parameters at baseline and reassessment were compared between groups using analysis of variance (ANOVA). Paired t-tests were used to compare the parameters at baseline and reassessment within each group. To further analyze the relationship of clinical periodontal disease resolution with changes in outcome parameters, Spearman correlation coefficients between changes in extent of sites with PD ≥5 mm, CAL ≥3 mm versus change in CRP and total leukocyte count were calculated.
Results
There was no significant difference between groups (P > 0.05), at baseline in terms of age, gender distribution, and number of teeth present (Table 1).At baseline, the comparison of mean probing pocket depth (PPD), mean CAL, and percentage of sites having PPD ≥5 mm with concomitant CAL ≥3 mm showed a statistically significant difference (P < 0.0001) between all groups. The percentage of sites with BOP showed statistically a significant difference between group A and group B (Table 2).
Mean figures with standard deviation.
Student t-test.
Chi-squared test.
Mean figures with standard deviation. P < 0.05 is significant.
Analysis of variance (ANOVA).
Abbreviations: PPD, probing pocket depth; CAL, clinical attachment loss; BOP, bleeding on probing.
Mean serum CRP values were highest in group A (3.28 ± 1.4 mg/L), followed by group B (1.05 ± 0.2 mg/L) and group C (0.8 ± 0.3 mg/L). The difference in CRP levels was highly statistically significant between groups A and C (P <0.0001) and between groups A and B (P < 0.0001), but was not statistically significant between groups B and C. Mean serum triglycerides were significantly higher in group A as compared to group C, with no significant differences noted between groups with regards to other parameters of lipid metabolism. Mean total leukocyte counts were similarly highest in group A at 8,322 ± 1,888/mL 3 , followed by group B at 6,137 ± 712/mL 3 , and group C at 5,176.6 ± 641/mL 3 , with the differences between groups A and C and between groups A and B showing statistical significance (Table 3).
Mean figures with standard deviation. P < 0.05 is significant.
Analysis of variance (ANOVA).
Abbreviations: CRP, C-reactive protein; TLC, total leukocyte count; HDL, high-density lipoprotein; LDL, low-density lipoprotein; CHO, cholesterol; TG, triglyceride.
Comparisons of clinical periodontal parameters at baseline and at reassessment in groups A and B showed a highly statistically significant difference between baseline and reassessment values of PPD, CAL, percentage of sites having PPD ≥5 mm with concomitant CAL ≥3 mm in both groups A and B, and percentage of sites with BOP, thus validating the efficacy of periodontal treatment (Table 4).
Mean figures with standard deviation. P < 0.05 is significant.
Paired t-test.
Abbreviations: PPD, probing pocket depth; CAL, clinical attachment loss; BOP, bleeding on probing.
Mean serum CRP in group A decreased from 3.28 ± 1.4mg/L to 2.6 ± 1.5 mg/L, which was highly statistically significant. In group B, mean CRP values decreased from 1.05 ± 0.2 mg/L to 0.89 ± 0.2 mg/L, although this difference was not statistically significant. Mean total leukocyte counts in group A reduced from 8,322 ± 1,888 to 6,361 ± 1,426, which was statistically significant. A similar reduction occurred in group B, although it was not statistically significant (Table 5, Fig. 1).
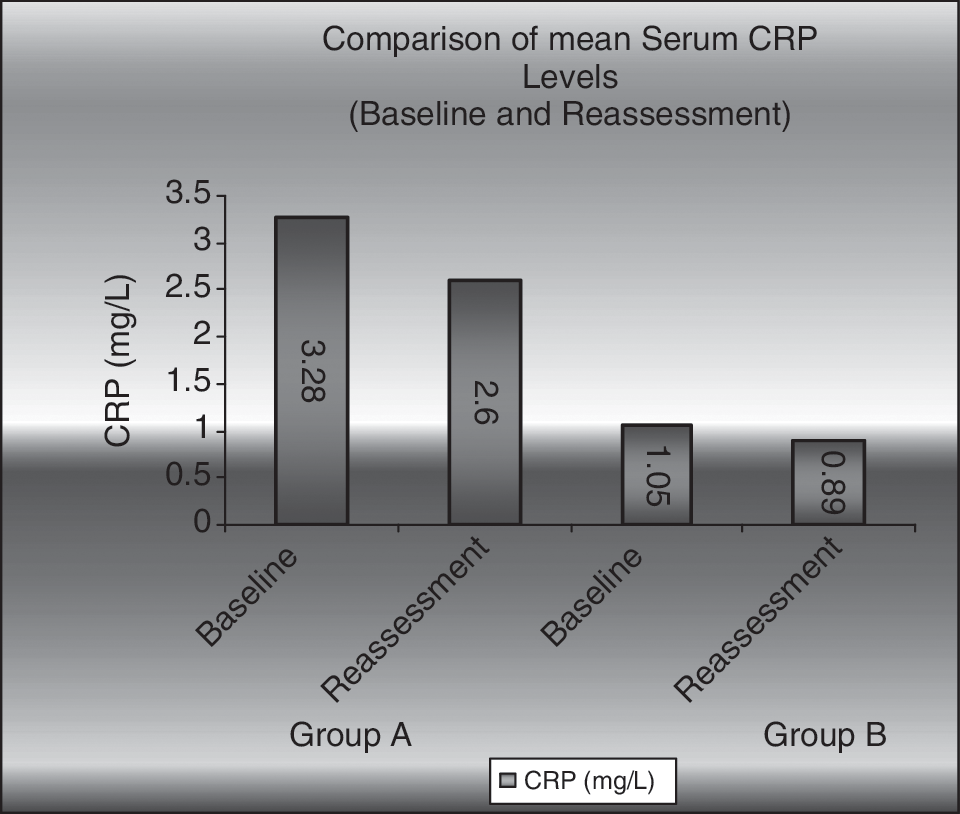
Comparison of mean serum C-reactive protein levels (baseline and reassessment). CRP, C-reactive protein.
Mean figures with standard deviation.
Wilcoxon ranked matched-pair test.
Paired t-test; P < 0.05 is significant.
Abbreviations: CRP, C-reactive protein; TLC, total leukocyte count; HDL, high-density lipoprotein; LDL, low-density lipoprotein; CHO, cholesterol; TG, triglyceride.
Mean serum trigycerides decreased in both groups, and this was statistically significant only in group A. Mean serum HDL was increased at reassessment in both groups, but this was statistically significant only in group A. Mean serum LDL showed lower values at reassessment in both groups, but the difference was not statistically significant. Mean cholesterol levels remained comparable and did not show a statistically significant change in either group (Table 5).
There was no significant correlation in changes in percentage of sites with PPD ≥5 mm, CAL ≥3 mm, and changes in serum CRP and total leukocyte count in group A. However, changes in serum CRP show a parital positive correlation with changes in this disease extent parameter (Table 6).
r is the Spearman correlation coefficient. P < 0.05 is significant.
Abbreviations: PPD, probing pocket depth; CAL, clinical attachment loss; TLC, total leukocyte count; CRP, C-reactive protein.
Discussion
Severe periodontitis has been associated with metabolic syndrome in middle-aged individuals, and it has been reported that subjects suffering from severe periodontal disease may be more than twice as likely to have metabolic syndrome than unaffected individuals. 16 Metabolic syndrome is an established predictor for both cardiovascular disease and diabetes. 17 Because both periodontitis and the metabolic syndrome are associated with systemic inflammation, these two diseases may be linked through a common pathophysiological pathway. 13,16 Thus, it follows that improvements in periodontal health may confer a reduction of systemic cardiometabolic risk factors.
In our study, subjects with metabolic syndrome had significantly higher mean measures of PPD, CAL, and percentage of BOP as compared to systemically healthy subjects. Although this finding may be incidental and attributed to the relatively broad case definition of periodontal disease adopted by us, it may also be indicative of the association of a poorer periodontal status with components of metabolic syndrome, as has been shown by various large-scale studies. 6,7,16,18
As expected, baseline mean serum CRP values were highest at 3.28 ± 1.4 mg/L in the periodontitis-affected individuals with metabolic syndrome (group A). Elevated serum CRP levels are associated with each metabolic syndrome component including obesity, hypertriglyceridemia, hypo-HDL-cholesterolemia, hyper-LDL-cholesterolemia, diabetes, hyperinsulinemia, hyperuricemia, and hypertension. 19 Higher CRP levels also independently associate with the presence of extensive periodontal disease. 2 20,21 Moreover, CRP values in this group are “elevated,” being greater than 3 mg/L, which is suggestive of an increased risk of both cardiovascular events 22,23 and metabolic disorders. 24,25 In addition to being a marker of innate immunity and systemic inflammation, CRP also has several direct effects at the level of the vessel wall, 26 causing multiple pathways of cardiovascular morbidity.
The observed mean total leukocyte count in periodontal disease with metabolic syndrome was highest at 8,322/ mm3. Leukocyte counts of 8,400/ mm3 have been reported as having a risk ratio of 1.4 for cardiovascular disease, as compared to 5,600/ mm3. 27 Chronic modest elevation of leukocytes increases blood viscosity and subsequent risk of cell adherence to endothelial lining and decrease in blood flow, which is associated with cardiovascular disease. 28 The moderate elevation of white blood cell (WBC) count, indicative of a low-grade systemic chronic inflammation, positively associates with features of metabolic syndrome, as shown by various studies and our findings are in agreement. 29,30
In the subjects with periodontitis only, we found a lower mean serum CRP level at 1.05 ± 0.2 mg/L. Whereas this was significantly lower than the metabolic syndrome group, it did not show a significant difference from that of the control group. As observed for serum CRP, we did not find a significantly elevated leukocyte count as compared to the control group. This may be attributed to the relatively lesser periodontal disease severity of this group. Only patients with advanced periodontal disease exhibit elevated CRP, 31 as opposed to those with less severe periodontal disease. The total pathogen burden is a significant predictor of levels of CRP, 32 and these results possibly validate the dose–response relationship of the systemic inflammatory response to the periodontal disease severity. The use of conventional case definitions of periodontal disease severity based on measures of clinical attachment loss is inadequate to quantify the systemic inflammatory burden imposed by periodontal disease and calls for the use of indices designed specifically for this purpose. 33
Periodontal therapy resulted in a significant decrease in serum CRP by 0.68 mg/L, at 8 weeks in the metabolic syndrome group, corresponding with the findings of a recent meta- analysis on studies assessing effect of periodontal treatment on serum CRP levels that reported that the range of effect in all studies was 0.3–0.7mg/L. 10 In subjects with metabolic syndrome, CRP level provides added prognostic information on subsequent risk for cardiovascular events, 34,35 in addition to being an independent risk predictor for cardiovascular events. 36 Hence, the moderate modulation of CRP levels noted as an outcome of periodontal improvement could possibly contribute to improved cardiovascular prognosis in metabolic syndrome subjects. The concomitant decrease in WBC counts consequent to reduction of periodontal bacterial load and inflammation of resolution corresponds with earlier reports, 37,38 is also indicative of a favorable modulation of cardiovascular risk. Although we did not assess the differential WBC count, it may have been of added value as neutrophil-to-lymphocyte ratio, and monocyte counts have been reported as stronger predictors of cardiovascular events as compared to total WBC count. 39,40 Periodontitis induced proinflammatory cytokines contribute to dysregulation of lipid metabolism. 12 Dyslipidemic status of the metabolic syndrome group also showed modulation with respect to a significant increase in HDL and decrease of triglycerides, corroborating with previous evidence that initial periodontal therapy alters serum lipid levels favorably in patients with both hyperlipidemia and periodontitis. 41
However, when considering the periodontitis-only group, we did not find periodontal therapy to significantly reduce CRP levels or WBC counts. Lipid levels remained largely unmodulated. The 0.16 mg/L mean drop in CRP, albeit nonsignificant, is similar to that observed by Ide et al. 9 Although this finding is most likely attributable to the baseline difference in disease severity, the magnitude of reduction of systemic inflammation resulting from periodontal therapy is reported as heterogeneous and inconsistent across subjects. 42 This could also account for the fact that only a partially positive correlation of CRP decrease with clinical resolution of periodontal disease was noted in the metabolic syndrome group. Both local and systemic inflammatory response are linked to the individuals genetic background, with specific cytokine polymorphisms of interleukin-1 (IL-1) and IL-6 genes being associated with serum CRP and other inflammatory marker levels. 43 Such genetic variations may produce a heightened individual local and systemic response to periodontal pathogens as well as to the treatment. Thus, these may predispose a subpopulation of periodontitis patients to metabolic disorders through common pathways, such as oxidative stress causing a bidirectional association. 44 Genetic influence on metabolic syndrome expression in various population groups is known, 45 but there are no data specifically regarding Indian subjects. Moreover, while in part shared lifestyle-related risk factors may account for the association of metabolic syndrome and periodontal disease, the possibility of underlying genetic traits and other pathophysiologic mechanisms common to both conditions must be explored in context of different ethnic populations.
Conclusions
Baseline periodontal status and serum CRP levels were worse in metabolic syndrome subjects of Indian ethnicity with periodontal disease, as compared to a group of systemically healthy periodontitis-affected individuals. Standard nonsurgical periodontal therapy caused a modest but significant decline in serum CRP levels, dyslipidemic status, and WBC counts in these subjects similar to that reported in other ethnic groups with periodontal disease only, 10,38,41 whereas only a nonsignificant systemic effect was noted in the systemically healthy group with periodontal disease. This therapeutic effect could indicate a potentially additional cardio-protective benefit of periodontal therapy in peridontally diseased individuals with metabolic syndrome.
Author Disclosure Statement
No competing financial interests exist.