
Abstract
Background:
Leptin is a hormone expressed by the leptin gene, primarily in adipocytes, controlling food intake and energy expenditure. The effects of leptin are mediated by its receptor (LEPR) located in the central nervous system and other tissues, including adipocytes and endothelial cells. The aim of this study was to characterize two polymorphisms of LEPR, Lys109Arg (rs1137100) and Gln223Arg (rs1137101), as risk factors for early atherosclerosis. This connection has not been studied before.
Methods:
This study was performed in the randomly selected, middle-aged control subjects (n = 526) from our well-defined OPERA (Oulu Project Elucidating Risk of Atherosclerosis) study. Analysis of covariance (ANCOVA) was performed to study the associations between genotypes, intima media thickness (IMT) measurements, and risk factors for atherosclerosis.
Results:
Subjects with the genotype Lys109Arg had the lowest body mass index (BMI) (P = 0.035), whereas Arg109Arg homozygotes had the highest total cholesterol (P = 0.021) when adjusted for sex and age. Gln223Arg associated independently with systolic blood pressure (P = 0.036). There were no differences in leptin concentrations between the genotypes. The adjusted (sex, age, BMI, smoking status, low-density lipoprotein cholesterol, systolic blood pressure, and fasting blood glucose) means for the IMT measurements were lowest in the Arg109 and Arg223 homozygotes (P = 0.042 and P = 0.041, ANCOVA, respectively).
Conclusions:
The variations in the LEPR gene are independently associated with early atherosclerosis and some of its risk factors. These variations could possibly affect leptin signaling and thereby modify the effects of leptin on the atherosclerotic process.
Introduction
Atherosclerosis is a complex disease with contributions from both environmental and genetic factors. The heritability varies between 40% and 60% in most populations. Atherosclerosis is a leading cause of mortality in the developed countries, and its incidence is on the increase in the developing countries. 5 The major risk factors for atherosclerosis are cigarette smoking, elevated blood pressure, and serum total and low-density lipoprotein cholesterol (LDL-C), low high-density lipoprotein cholesterol (HDL-C), diabetes mellitus, and advanced age, as well as, obesity, which is one of the recognized risk factors. 6 Plasma leptin levels, which reflect the amount of adipose tissue, have been associated positively with the risk of coronary heart disease, 7,8 although conflicting results also exist. 9 Leptin may be involved in atherogenesis through its effects on endothelial function, 10 accumulation of cholesterol esters into foam cells, 11 hemostatic factors, and modifying the classic risk factors of atherosclerosis. 12 Two single nucleotide polymorphisms (SNPs) of LEPR, Lys109Arg and Gln223Arg, have been studied previously and shown to associate with systolic blood pressure in men. 13 Lys109Arg was associated with leptin levels in overweight and obese postmenopausal women and Gln223Arg with body composition in overweight and obese women 14 and with body weight and body mass index (BMI) in Pacific Islanders. 15 In addition, the Gln223Arg polymorphism has been associated with total cholesterol and serum HDL-C and LDL-C levels in Japanese men 16 and in glucose-tolerant Caucasians. 17 Gln223Arg was also associated with the insulin sensitivity index and glucose clearance in glucose-tolerant Caucasians. 17 Lys109Arg and Gln223Arg polymorphisms have also been shown to associate with the conversion to type 2 diabetes in high-risk individuals with impaired glucose tolerance. 18 It seems that these polymorphisms are associated with various risk factors of atherosclerosis, but they have not been previously studied directly in association with atherosclerosis.
The aim of our study was to characterize Lys109Arg and Gln223Arg polymorphisms as risk indicators for early atherosclerosis. The degree of atherosclerosis was defined by intima media thickness (IMT) measurements, 19 and the association of polymorphisms to IMT and traditional risk factors of atherosclerosis was studied.
Materials and Methods
Subjects
OPERA (Oulu Project Elucidating Risk of Atherosclerosis) is a population-based, epidemiological study designed to address the risk factors and disease end points of atherosclerotic cardiovascular diseases. This study population and selection criteria have been previously described in detail. 20
In this study, we examined the control cohort of the OPERA project consisting of 526 subjects. The participants were interviewed, examined, and tested in our research laboratory. The study was conducted according to the principles of the Declaration of Helsinki, and approved by the Ethical Committee of the Faculty of Medicine, University of Oulu. Informed consent was obtained from each participant.
Carotid ultrasonography
The IMT was measured by one single trained radiologist without knowledge of the clinical data. IMT, defined as the distance between the media–adventitia interface and the lumen–intima interface, was measured using a duplex ultrasound system with a 7.5-MHz scanning frequency in B-mode, pulsed Doppler mode, and color mode (Toshiba SSA-270A, Toshiba Corp., Tokyo, Japan). The far-wall IMT was measured on both sides at three different locations: One measurement from the internal carotid artery (ICA), one measurement from the bifurcation enlargement (BIF), and three measurements from the common carotid artery (CCA) (proximal, middle, and distal from the bifurcation). The mean IMT (IBC) was defined as the mean of ICA, BIF, and the three highest CCA measurements.
Clinical measurements
The blood pressure measurements were conducted according to the recommendations of the American Society of Hypertension. All of the blood pressure measurements were recorded with an automatic oscillometric blood pressure recorder (Dinamap, Critikon Ltd., Ascot, UK). The resting blood pressure was measured three times at 1-min intervals on the right arm after the patient had been seated at least 5 min and after that two times at 1-min intervals with the patient standing. The mean value of the second and the third blood pressure measurement from the sitting patient was used in the analysis. Smoking history was obtained by a questionnaire. The lifetime smoking burden was calculated as pack-years (1 pack-year = 20 cigarettes smoked/day in 1 year). Height was measured to the nearest centimeter without shoes. Weight was measured to the nearest 0.1 kg on a lever balance with the subject wearing only light underwear without shoes. BMI was calculated as weight (kg) divided by height squared (m2). All of the measurements were performed by the same specially trained nurses.
Laboratory analyses
The very-low-density lipoprotein (VLDL) fraction was separated from plasma by ultracentrifugation at 10,500 × g for 18 h. The plasma HDL-C concentration was measured by mixing 0.5 mL of the VLDL-free fraction with 25 μL of 2.8% (wt/vol) heparin and 25 μL of 2 M manganese chloride and measuring the cholesterol concentration in the supernatant after centrifugation at 1,000 × g and 4°C for 30 min. The LDL-C concentration was calculated by subtracting the cholesterol concentration in HDL from that in the VLDL-free fraction. The concentrations of total cholesterol and triglycerides in the plasma were determined by enzymatic colorimetric methods (Boehringer Diagnostica, Mannheim, Germany). C-reactive protein was analyzed by using commercially available enzyme-linked immunosorbent assay (ELISA) kits (Diagnostic Systems Laboratories, TX). The glucose concentrations were measured with the glucose dehydrogenase method (Diagnostica, Merck, Darmstadt, Germany).
Genotyping
Genotypes were determined by restriction fragment length polymorphism (RFLP) method. The polymerase chain reaction (PCR) was performed in a 10-μL volume containing using 50 ng of genomic DNA, 450–nmoles of each primer for Lys109Arg, and 300 nmoles of each primer for Gln223Arg, 200 μM dNTP, 2 U DNA polymerase (DynaZyme DNA polymerase, Finnzymes, Espoo, Finland), and 1 × Optimized DyNAzyme™ Buffer (10 mM Tris-HCl, 1.5 mM MgCl2, 50 mM KCl, 0.1% Triton X-100). PCR cycles consisted of 40 cycles at 95°C for 30 s, annealing at 55°C for 30 s, and extension at 72°C for 30 s. PCR products were digested over night at 37°C with, respectively, 5 U of HaeIII and MspI restriction enzymes for the Lys109Arg and Gln223Arg polymorphisms. The digested samples for Lys109Arg were separated on a 3% agarose gel and for Gln223Arg on a 2.5% agarose gel. The following primers were used to amplify regions of the leptin receptor. There was a mismatch (italic) in the Lys109Arg reverse primer to create an artificial restriction site. Lys109Arg F, 5′-CTGTTGAACCTAAGTTTAATTC AAG-3′; Lys109Arg R, 5′-G
Statistical methods
Allele and haplotype frequencies and linkage disequilibrium were calculated with CubeX. 21 The chi-squared test was carried out to determine if the observed frequencies were in Hardy–Weinberg equilibrium. The data were analyzed with SPSS (version 16.0, SPSS Inc.). Analysis of covariance (ANCOVA) was used to compare the means of the variables measured. In the multivariate analysis, sex, age, BMI, smoked pack-years, LDL concentration, and systolic blood pressure (SBP) were added as explanatory factors. To normalize the skewed distributions, log-transformed values of IMT measurements, BMI, SBP, leptin, total cholesterol, triglyceride, LDL, HDL, and C-reactive protein (CRP) concentrations were used. The Bonferroni test of SPSS was used to distinguish the significance of differences in the traits between each genotype. Results with a P value less than 0.05 were considered statistically significant.
Results
Among the subjects studied, 4.2% had a diagnosis of type 2 diabetes. Additionally, 4.0% were suffering from hypertension (HTA) and 10.5% were treated with blood pressure–lowering medication. The drugs used by the subjects were thiazide diuretics (1.9%), loop diuretics (0.4%), beta blockers (5.7%), calcium channel blockers (3.2%), angiotensin-converting enzyme inhibitors (2.1%), lipid-lowering medication (1.9%), acetylsalicylic acid (3.4%), metformin (0.2%), and sulfonylurea (0.8%).
The allele frequency of Arg109 was 35.8% and that of Gln223 was 39.5%. The genotype frequencies were in Hardy–Weinberg distribution. The polymorphisms were in linkage disequilibrium, with standardized linkage disequilibrium (D′) of 1.0 and r 2 of 0.3647 (P < 0.001). The haplotype frequencies were 0.395 for Lys109/Gln223, 0.2466 for Lys109/Arg223, and 0.3584 for Arg109/Arg223. No subjects with haplotype Arg109/Gln223 were detected.
The main characteristics of the study subjects by LEPR Lys109Arg and Gln223Arg genotypes are shown in Table 1. Lys109Arg was significantly associated with BMI in our study after adjustment for sex and age (P = 0.035) and total cholesterol adjusted for sex, age, and BMI (P = 0.021). Subjects with the genotype Lys109Arg displayed the lowest BMI whereas Arg109 homozygotes exhibited the highest total cholesterol. Gln223Arg associated with SBP after adjustment for sex, age, and BMI (P = 0.036). SBP was highest among Gln223Arg heterozygotes. There were no differences in the leptin concentration between genotypes when adjusted for sex, age, and BMI.
Values are means and 95% confidence intervals. P = probability for a difference between genotypes in analysis of covariance (ANCOVA) adjusted for sex, age, and body mass index (BMI).
Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; N.S., not significant.
The polymorphisms were associated with IMT measurements (Table 2). Lys109Arg was significantly associated with BIF (P = 0.005), ICA (P = 0.034), and the mean value of ICA, BIF, and CCA (IBC) (P = 0.012) when adjusted with sex. After adjustment for sex, age, BMI, smoked pack-years, LDL-C, SBP, and fasting blood glucose, the association between Lys109Arg and BIF (P = 0.018) and IBC (P = 0.042) remained significant. When adjustment of lipid and blood pressure–lowering medication was included into the analysis, association of Lys109Arg with BIF (P = 0.017) and IBC (P = 0.038) remained. Arg109Arg homozygotes showed the lowest IMT.
Values are means and 95% confidence intervals.
p = probability for a difference between genotypes in analysis of covariance (ANCOVA) adjusted for sex, age, body mass index (BMI), smoked pack–years, low-density lipoprotein cholesterol, systolic blood pressure, and fasting blood glucose.
Abbreviations: IMT, intima media thickness; CCA, common carotid artery; BIF, bifurcation enlargement; ICA, internal carotid artery; IBC, the mean value of CCA, BIF, and ICA; N.S., not significant.
Gln223Arg was also associated with IMT measured by carotid ultrasound. When adjusted with sex, CCA (P = 0.005), BIF (P = 0.050), ICA (P = 0.001), and IBC (P = 0.004) were associated with Gln223Arg genotypes. IMT values were significantly lower among Arg223Arg homozygotes. After adjustment for sex, age, BMI, smoked pack-years, LDL-C, SBP, and fasting blood glucose, differences in the IMT of ICA (P = 0.006) and IBC (P = 0.041) between Gln223Arg genotypes remained significant. When adjusted with lipid and blood pressure–lowering medication, association of Gln223Arg with ICA (P = 0.006) and IBC (P = 0.039) remained. Mean IMT measurements in relation to the polymorphisms are shown in Fig. 1.
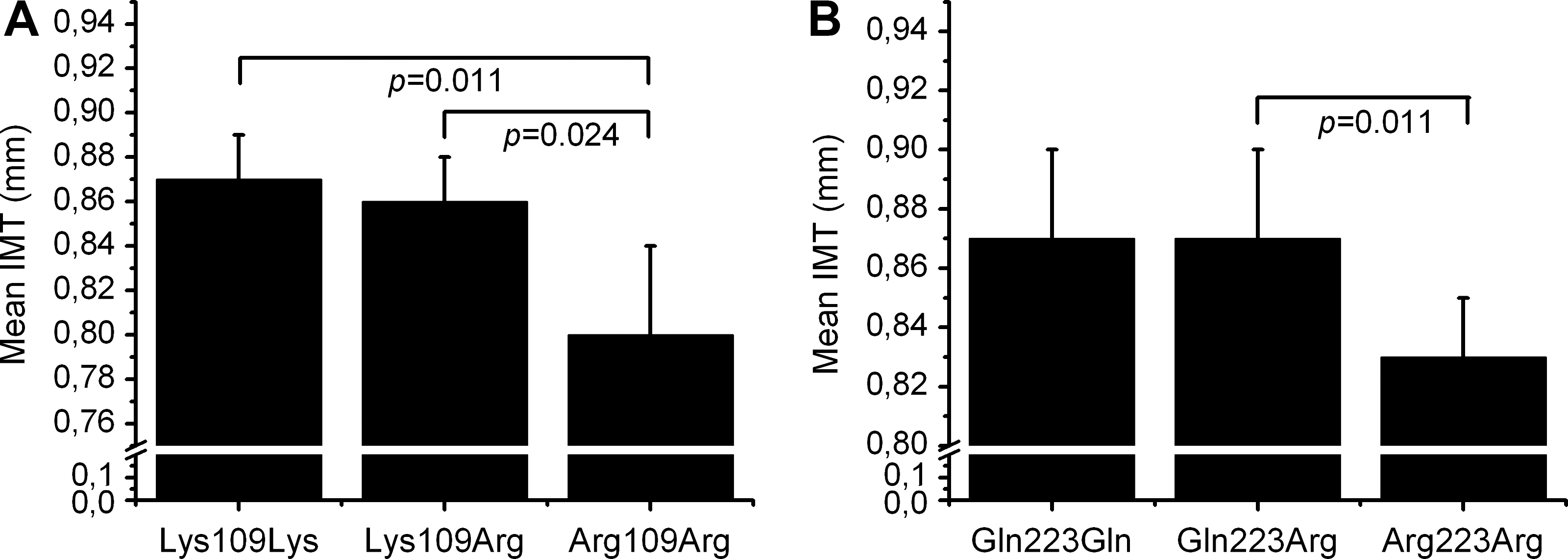
Mean intima media thickness (IMT) values in relation to Lys109Arg (P = 0.012) (
Discussion
The aim of our study was to explore the possible association between polymorphisms in LEPR, cardiovascular risk factors, and IMT measurements. As far as we are aware, the findings reported here are the first to have evaluated these single-nucleotide polymorphisms (SNPs) in the LEPR in relation to IMT measurements in humans. IMT measured by carotid ultrasound is a reliable indicator of early atherosclerosis. The most significant finding was the lowest IMT values in the subjects carrying Arg109 and Arg223 in the LEPR gene.
In our study, Lys109Arg displayed a significant association with BMI, but interestingly heterozygotes had the lowest BMI of the group. Previously an association was shown between Lys109Arg and BMI, with Arg109 homozygotes appearing to have the lowest BMI in comparison to other genotypes. 13 In contrast, another study identified an association between BMI and Gln223Arg, but no association was found between BMI and Lys109Arg. 15 We also found an important association between Lys109Arg and total cholesterol levels. Interestingly, Arg109 homozygotes possessed the highest total cholesterol levels. To our knowledge, this kind of association between Lys109Arg and total cholesterol has not been reported previously. The fact that the association observed between the LEPR gene Lys109Arg polymorphism and IMT measurements remained significant after adjustment for total cholesterol, among other conventional cardiovascular risk factors, is consistent with the concept that the variation in IMT among LEPR Lys109Arg genotypes is not mediated through lipid abnormalities. It must also be pointed out that HDL-C tended to be higher among Arg109 carriers and the association of LDL-C with LEPR Lys109Arg variation was nonsignificant.
Therefore, the total cholesterol-to-HDL-C ratio, a ratio that has been used in predicting an individual's risk of developing atherosclerosis, did not differ between the three genotype groups (4.2 for Lys109Lys, 3.9 for Lys109Arg, and 4.1 for Arg109Arg). Another polymorphism, Gln223Arg, displayed an association with SBP, although it seemed to be highest among Gln223Arg heterozygotes in our study. In previous reports, however, SBP was lowest among Arg223 homozygotes. 13,22 Arg109 and Arg223 alleles have also been shown to protect from the conversion to type 2 diabetes in high-risk individuals with impaired glucose tolerance. 18 These results suggest that leptin receptor polymorphisms may have some impact on atherosclerosis risk factors. In particular, the association observed here between variations in the LEPR gene and IMT measurements remained significant after adjustment for conventional cardiovascular risk factors, which is consistent with the concept that some additional mechanisms related to the LEPR genotype must be considered.
Lys109Arg and Gln223Arg polymorphisms are located in the cytokine receptor homologous 1 (CRH1) domain in LEPR. The function of this region has still not been clarified and will need to be studied more carefully. However, some functional studies have been performed, and it has been claimed that the CRH1 domain is probably not involved in leptin binding. 23 The CRH domain contains a conserved WSXWS motif that is believed to be essential for proper folding of the domain. 24,25
The Gln269Pro mutation in this same domain also causes the obese phenotype of the fa/fa rat 26 and results in defective LEPR signaling. 27 Because Lys109Arg, Gln223Arg, and Gln269Pro are all located in the same domain, it is possible that Lys109Arg and Gln223Arg could also affect the function of LEPR. In a previous study, a deletion of CHR1 resulted in a lower leptin response, and it seems that CRH1 contributes to optimal LEPR activation. 28 The study by Stefan et al. suggests that Arg223 allele carriers of the Gln223Arg polymorphism had also lower leptin binding to the soluble form of the leptin receptor. 29
These results suggest that these two polymorphisms, Lys109Arg and Gln223Arg, could affect the function of LEPR by influencing the stability or correct folding of this domain or the LEPR complex formation. This might affect the leptin-mediated signaling and impair the effects of leptin. Leptin resistance has been observed in obesity, 30 and this may promote the development of atherogenesis.
In conclusion, we have shown here that Lys109Arg and Gln223Arg associate with BMI, SBP, and IMT measurements. This result suggests that the variations in LEPR gene are associated with early atherosclerosis and this is independent of the traditional risk factors for atherosclerosis.
Footnotes
Acknowledgments
We would like to thank Heidi Häikiö, Saija Kortetjärvi, Liisa Mannermaa, and Leena Ukkola for expert technical assistance and Dr. Markku Päivänsalo, M.D., Ph.D., for carrying out the carotid IMT measurements and analyses. This study was supported by the Medical Council of the Academy of Finland and the Finnish Foundation for Cardiovascular Research.
Author Disclosure Statement
The authors have no conflicts of interest to declare. No competing financial interests exist.