
Abstract
Objective:
It has been shown that patients with insulin resistance (IR) have a higher prevalence of thyroid nodules and bigger thyroid glands. We evaluated the ability of metformin (M) alone or combined with levothyroxine (L-T4) to reduce the nodular size in benign thyroid hyperplastic nodules (<2 cm in diameter).
Methods:
A total of 66 women with IR and nodular hyperplasia, diagnosed by fine needle aspiration biopsy (FNAB), who completed this prospective 6-month duration protocol, were assigned to one of four groups: Group I (GI) (n = 14), patients treated with M; GII (n = 18), patients treated with M plus L-T4; GIII (n = 19), patients treated with L-T4; and GIV (n = 15), patients without any treatment.
Results:
All groups of included patients had no statistically significant different mean baseline characteristics. Patients from GII and GIII showed drops in thyroid-stimulating hormone (TSH) levels and GI and GII normalized the homeostasis model assessment (HOMA) index after treatment, as expected. The median baseline size of all included nodules was 298 mm3 ≈0.84 cm in diameter (range, 32–3,616 mm3). After treatment, patients of Group I and II showed significant reductions in their nodule size [median reduction, 108.50 mm3 (30%) and 184.5 mm3 (55%), P < 0.008 and P < 0.0001, respectively]. Patients in GIII and GIV did not have a significant reduction of their nodules [P = not significant (N.S.)].
Conclusions:
We conclude that M produced a significant decrease in the nodular size in patients with IR and small thyroid nodules, whereas the combination of M with L-T4 was the best treatment in these women.
Introduction
IR has been increasing epidemically in the last years together with the spread of the obesity epidemic. 4 When insulin-resistant individuals cannot maintain the degree of hyperinsulinemia, type 2 diabetes generally develops. 4 We have shown that those individuals with hyperisulinemia have larger thyroid glands and a higher prevalence of thyroid nodules. 5 These original findings were recently corroborated by Ayturk et al. 6 in a Turkish area with mild to moderate iodine deficiency. Moreover, we have also reported the higher incidence of IR in patients with differentiated thyroid cancers (DTC), and it has been postulated that it would be an important risk factor for developing DTC, as is well known with some other nonthyroid carcinomas. 7,8 Furthermore, we have also shown that patients with achrocordons (skin tags) have an elevated prevalence of thyroid nodules associated with a high frequency of IR. 9 In the present study we evaluated prospectively the capability of metformin (M), levothyroxine (L-T4), or a combination of both for reducing the size of thyroid nodules smaller than 2 cm in diameter in patients with IR.
Subjects and Methods
Subjects
A total of 80 women with IR and thyroid nodular hyperplasia, diagnosed by ultrasonography (US) and fine needle aspiration biopsy (FNAB), were initially included (20 to each group); however, only 66 completed the 6-month follow-up period that this study demanded. In these subjects, 75 thyroid nodules were studied.
Fourteen subjects dropped out of the study. The subjects excluded were 6 in Group I (GI) (5 failed to take the medication, and 1 did not come to the controls); 2 subjects in GII (who stopped taking M); 1 subject stopped taking L-T4 in GIII and 5 subjects decided not to continue with the controls in GIV. Any of the patients were excluded because they had an increase in thyroid volume or nodule volumes.
The estimate of IR by homeostasis model assessment (HOMA) score was calculated with the following formula: Fasting serum insulin (μU/mL) × fasting plasma glucose (mmol/L)/22.5. A HOMA index ≥2.5 denoted IR. All patients were euthyroid with negative titers of antithyroperoxidase antibodies (TPO-Ab) and were living in an iodine-sufficient area. The mean value of urinary iodine observed in subjects living in this area was 140 μg/24 h. 10 All subjects gave written voluntary consent to participate in the study. Procedures were applied in agreement with the ethical guidelines of our institutions.
Methods
Anthropometric measurements
Body weights (kg) and heights (m) were measured without shoes and/or cap. Body mass index (BMI) was expressed as weight per squared height (kg/m2).
Biochemical evaluations
All blood samples were taken between 8:00 and 9:00 a.m., after 12 h of fasting. After collection, serum samples were stored at −20°C and assayed in not more than a week.
Insulin determination techniques
Insulin was determined by a two-site chemiluminescent immunometric assay with solid-phase anti-insulin murine monoclonal antibodies and sheep polyclonal anti-insulin antibodies, and mouse monoclonal anti-insulin antibodies conjugated with calf intestine alkaline phosphatase in buffer solution (IMMULITE® INSULIN, Diagnostic Products Corporations, Los Angeles, CA), with 2 IU/mL sensitivity. Intraassay precision of the equipment used was 6.4% and 5.3% for 7.39 and 300 IU/mL values, respectively. Interassay coefficient of variation (CV) was 8% and 7% for 7.39 and 300 IU/mL values, respectively.
Glycemic determination techniques
Glycemia was determined using the glucose oxidase (GOD/PAP) automated method (SEA-PAK® Plus, Bayer Corporation, manufactured in Sées, Industrial Area, France). Spectrophotometer sensitivity at 505 nm was 0.70 mg/dL.
Thyrotropin, or thyroid stimulating hormone (TSH), and TPO-Ab were measured by electrochemiluminescent technology with an automatic analyzer (Roche Diagnostics Elecsys 2010 Immunoassay System, Mannheim, Germany). Values were expressed as IU/mL.
Evaluation of the thyroid gland morphology
Thyroid USscannings were performed in all subjects by the same operator, using the same 7.5-MHz linear transducer. Thyroid volume was calculated by the elliptical shape volume formula (0.479 × length × width × height) for each lobe; thyroid volumes were expressed as cm3. Thyroid nodules had to be solid to be included in the analysis. Although we usually consider as thyroid nodules all the US nodular lesions >3 mm diameter, in this study, due to the FNAB accessibility, the smallest thyroid nodule considered for inclusion was 4 × 4 × 4 mm; nodule volumes were expressed as mm3.
Cytology
All samples of FNAB were performed and analyzed by the same thyroid expert pathologist. The cytology was diagnostic and consistent with nodular hyperplasia in all cases. There was no diagnosis of follicular neoplasm or thyroid cancer.
Interventions
After diagnosis of the presence of IR, and signed informed consent, patients were randomly assigned to one of four groups to receive a specific treatment. Women who completed the 6-month follow-up period were in: GI, 14 patients (19 thyroid nodules) who receive only M; GII, 18 patients (21 thyroid nodules) who received M and L-T4; GIII: 19 subjects (20 thyroid nodules) who received only L-T4 treatment; GIV, 15 patients (15 thyroid nodules) without any treatment.
Metformin was indicated with the following schedule: 1 g b.i.d, in two 500-mg doses, administered with lunch and dinner, respectively. L-T4 was administered 30 min before breakfast every day. The dose was adjusted to keep a serum TSH level between 0.11 and 0.99 μU/mL. TSH levels were measured every 2 months. Both treatments were kept for 6 months, at which point all patients were reevaluated with US by the same operator and the same equipment.
Statistical analysis
Statistical analysis began with estimating the significance of the Shapiro–Wilk test in all of variables to decide whether or not to use the parametric test. The Kruskall–Wallis test was used to evaluate the significance of differences of median among therapeutic groups. The Wilcoxon test was used for the comparison of each group before and after treatment; and the Fisher or chi-squared test, when corresponding, was used to compare percentages of different groups. The observed differences were assumed to be statistically significant if the probability of chance occurrence was less than 5% (P < 0.05).
Results
The baseline characteristics of patients included in the four different groups are shown in Table 1. All groups of included patients had a nonstatistically significant different median baseline age, weight, BMI, HOMA index, TSH levels, thyroid gland volume, and nodule diameter [P = not significant (N.S.)]. The mean HOMA index for all subjects was 3.4 ± 0.4.
Group I (GI), patients with insulin resistance (IR) who received metformin (M); GII, patients with IR who received M and levothyroxine (L-T4); GIII, patients with IR who received L-T4 treatment; GIV, patients with IR who did not receive any treatment.
The numbers in parentheses in last row are the number of nodules included in respective groups.
P = significance of Kruskall–Wallis test.
SEM, standard error mean; N.S., not significant; HOMA, homeostasis model assessment; BMI, body mass index; TSH, thyroid-stimulating hormone.
Patients from GII and GIII, showed significant drops on TSH levels after 6 months of treatment (Table 2), as expected. In these patients, mean serum TSH levels lowered from 2.81 μU/mL to 0.59 μU/mL (P < 0.0001). At the end of treatment, patients who received L-T4 (GII and GIII) showed significantly lower TSH levels with respect to those subjects who did not (GI and GIV) (P < 0.0001 of the Kruskall–Wallis test). Patients of GI and GII also showed significant changes in the HOMA scores. (GI, from a baseline index of 3.8 ± 0.4 to 1.87 ± 0.34; P < 0.001; and GII from 3.3 ± 0.4 to 1.9 ± 0.86; P < 0.001).
Group I (GI), patients with insulin resistance (IR) who received metformin (M); GII, patients with IR who received M and levothyroxine (L-T4); GIII, patients with IR who received L-T4 treatment; GIV, patients with IR who did not receive any treatment.
TSH, thyroid-stimulating hormone; SEM, standard error mean.
Those patients who received any of the treatments, whether M or L-T4, showed statistically significant reductions in their thyroid gland volume (Table 3). At the end of treatment, there were no significant differences in the posttreatment thyroid volume between GI, GII, and GIII (P = N.S. of the Kruskall–Wallis test).
Group I (GI), Patients with insulin resistance (IR) who received metformin (M); GII, patients with IR who received M and levothyroxine (L-T4); GIII, patients with IR who received L-T4 treatment; GIV, patients with IR who did not receive any treatment.
P = significance of Wilcoxon test.
SEM, standard error mean; N.S., not significant.
The median baseline size of all included nodules was 298 mm3 ≈0.84 cm in diameter] (range, 32–3,616 mm3). After treatment, patients with IR who received only M (GI) and those treated with M and L-T4 (GII) showed extremely significant reductions in their nodule size (Table 4). The percentages of nodules that reduced their size (independently of the magnitude of such reduction) in the different groups in each group are shown in Fig. 1.
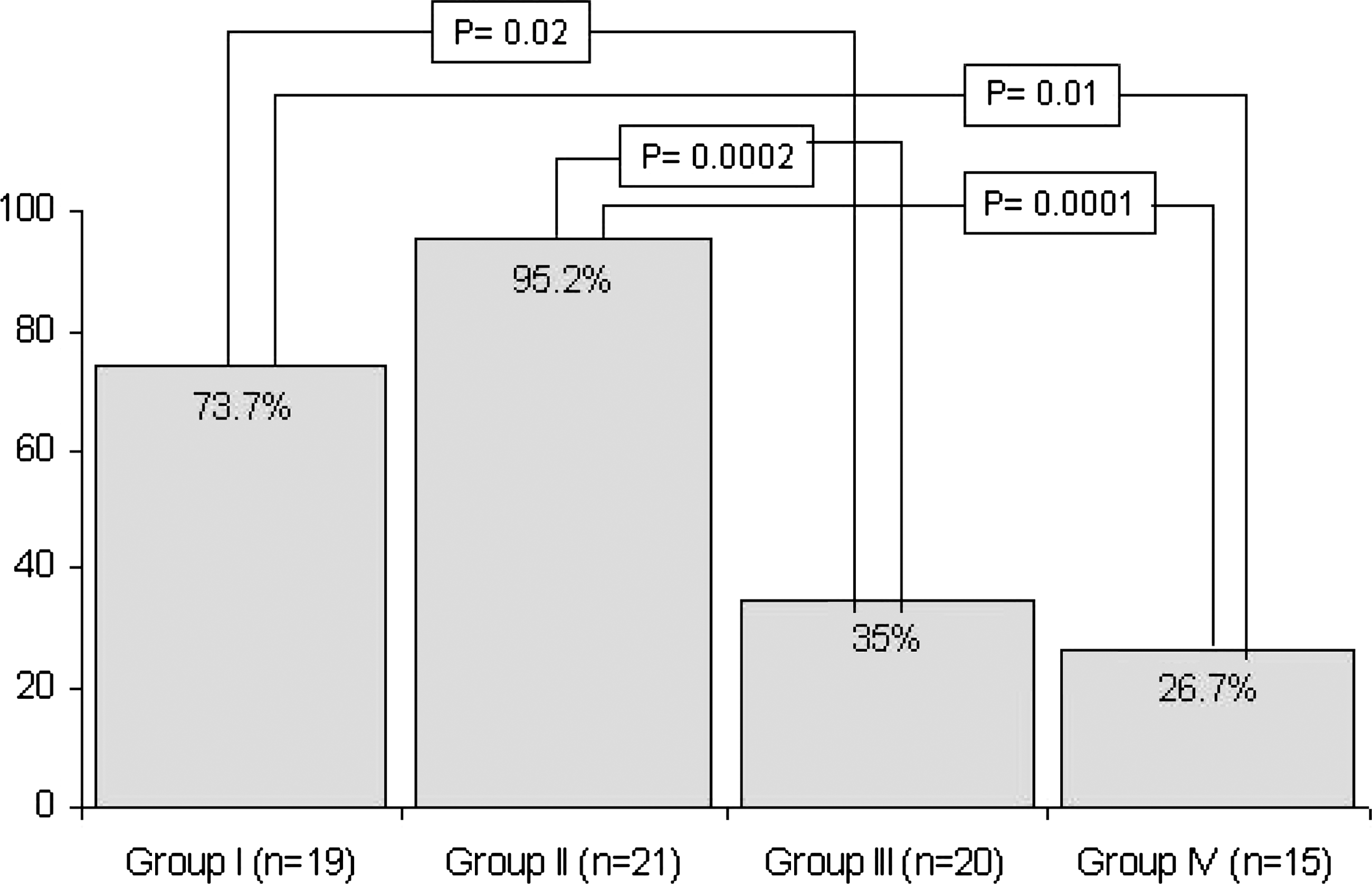
Percentage of nodules that reduced their size (independently of the magnitude of such reduction) in the different groups. Group I (GI), Patients with insulin resistence (IR) who received metformin (M); GII, patients with IR who received M and levothyroxine (L-T4); GIII, patients with IR who received L-T4 treatment; GIV, patients with IR who did not receive any treatment. P = significance of chi-squared test.
Group I (GI), Patients with insulin resistance (IR) who received metformin (M); GII, patients with IR who received M and levothyroxine (L-T4); GIII, patients with IR who received L-T4 treatment; GIV, patients with IR who did not receive any treatment.
P = significance of Wilcoxon test.
N.S., not significant.
Patients with IR treated only with M (GI) significantly reduced their thyroid nodule size with respect to those patients only treated with L-T4 (GIII) (P = 0.02), or those without treatment. (GIV) (P = 0.01). Patients treated with M and L-T4 (GII) showed statistically significant reductions in thyroid nodules (P = 0.0002 compared with GIII and P = 0.0001 compared with GIV, respectively).
When baseline thyroid nodules were arbitrarily divided into larger or smaller than 1 cm in diameter, it was shown that the proportions of reduction were similar between both sizes, in all of groups (P = N.S.) (Table 5).
Group I (GI), Patients with insulin resistence (IR) who received metformin (M); GII, patients with IR who received M and levothyroxine (L-T4); GIII, patients with IR who received L-T4 treatment; GIV, patients with IR who did not receive any treatment.
P = significance of Fisher test.
N.S., not significant.
Discussion
Thyroid nodules, due to multinodular goiter, are enlargements of the thyroid gland characterized by excessive growth and structural transformation of one or several areas within the normal thyroid tissue. Their etiology seems to involve complex interactions between environmental, genetic, and endogenous factors. The exogenous predisposing factors might be the iodine intake, smoking, certain drugs, and natural goitrogens. All of these factors are supposed to interact with gender and with genetic aspects. 11
Because we chose patients with small nodules (no greater than 2 cm in diameter), and the cytology was nodular hyperplasia in all patients, we did not observe those cystic and complicated (hemorrhagic, with fibrosis, necrosis, calcifications, etc.) and heterogeneous features observed in larger nodules of patients with a long evolution of a multinodular goiter. It is supposed that these kinds of “noncomplicated” thyroid nodules might have a better response when the trophic stimulus is blunt.
At first glance, it seems clear that TSH is the major growth factor of the thyroid gland. However, this straightforward interpretation neglects some findings that point to an intricate complexity of TSH-dependent and -independent mechanisms within a network of interacting positive and negative signals. 12 TSH is not only involved in the control of differentiated functions, it also regulates the expression of growth factors and their receptors. 12,13 This has been demonstrated, for example, for the expression of epidermal growth factor (EGF) receptors, 14 and for insulin-like growth factor I (IGF-I)-dependent signaling. 15 Indeed, TSH promotes the insulin IGF-I signaling. 16 –19 Moreover, exposure to TSH- or cyclic adenosine monophosphate (cAMP)-elevating agents increased the responsiveness of thyroid cells to stimulation with insulin, IGF-I, and IGF-II. 17 Accumulated evidence indicates that IGF-I-dependent, TSH-independent signaling may be of major importance for growth regulation of the human thyroid gland. This assumption is supported by findings in conditions not accompanied by increased TSH secretion, such as in acromegaly, in which high intrathyroidal IGF-I levels may contribute to goiter development. 20 Thus, on one hand, TSH induces the expression of growth factors and their receptors and may contribute to an increased responsiveness to growth factor–stimulated tyrosine kinase signaling with consequent proliferation via pathways other than the cAMP cascade, like the elevated insulin levels observed in the insulin-resistant state.
However, although subjects were selected in part on the basis of baseline IR, it is unknown whether this variable was a relevant factor in the outcome of the study. The justification for L-T4 administration with the aim of suppressing TSH long enough so as to decrease the size or arrest the growth of thyroid nodules has been a highly controversial issue. 21 Most of the current evidence seems to suggest that thyroid hormone therapy is not effective in shrinking the majority of thyroid nodules. 21 A beneficial effect of thyroid hormones on diffuse goiters has been demonstrated in several controlled trials. 22 –29 This has not always been possible to prove with nodular goiters. 25 There are only three controlled studies in which ultrasonography has been used for objective size monitoring. 30 –32 A 50% decrease in nodular size has been shown in only 30% of patients. 31
On the other hand, the impact of IR on the thyroid gland has recently been assessed by our group and another group of investigators. 5,6 We have shown that patients with IR have larger thyroid volume and a higher prevalence of thyroid nodules. 5 We have also introduced, for the first time, the thyroid gland morphology as another “victim” of the IR syndrome. Following these findings, we designed this prospective study in which we hypothesized that correction of IR with M would decrease thyroid nodule size. Following this rationale, not surprisingly, we observed that when our patients with IR were treated only with L-T4 (GIII), there was no decrease in thyroid nodule volume. However, in patients with IR who received only M, 74% of their nodules decreased, which was also enhanced when the combination treatment with M and L-T4 was administered (95.2%). Additionally, when GII was compared with GIII and GIV, the significances were very important, and no statistically significant differences were found between GIII and GIV.
Although it has been reported that M can decrease endogenous TSH levels due to an unknown mechanism, 33 –35 we did not observe significant changes on TSH levels in GI (patients who received M alone) when the comparison was performed pre- and post-M treatment. Serum TSH concentrations at the end of treatment were not significantly different between GI and GIV (2.17 vs. 2.57). Published papers showed this effect with M doses of 1,700 mg/day. Perhaps this could explain the different findings.
We concluded that in patients with IR and small hyperplastic thyroid nodules, M produced a significant decrease in the nodular size. The combination of M with L-T4 showed the best result in thyroid nodule volume decrease in these women. L-T4 alone only prevented the nodular growth, but it was not effective in reducing the nodular volume in the subjects with IR. Because TSH and insulin are thyroid growth factors, the combined treatment, which decreased the serum levels of both hormones, appears to be a very good therapeutic tool in these patients. More studies will be necessary to reproduce these results.
Footnotes
Author Disclosure Statement
The authors have nothing to declare. This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.