
Abstract
Background:
The epidemiological evidence supporting a causal link between Mediterranean diets and body weight is contrasting. We evaluated the effect of Mediterranean diets on body weight in randomized controlled trials (RCTs) using a meta-analysis.
Methods:
We searched English and non-English publications in PubMed, Embase, Scopus, and the Cochrane Central Register of Controlled Trials from inception to January, 2010. Two evaluators independently selected and reviewed eligible studies. Sixteen randomized controlled trials, with 19 arms and 3,436 participants (1,848 assigned to a Mediterranean diet and 1,588 assigned to a control diet) were included.
Results:
In a random-effects meta-analysis of all 19 arms, the Mediterranean diet group had a significant effect on weight [mean difference between Mediterranean diet and control diet, −1.75 kg; 95% confidence interval (CI), −2.86 to −0.64 kg] and body mass index (mean difference, −0.57 kg/m2, −0.93 to −0.21 kg/m2). The effect of Mediterranean diet on body weight was greater in association with energy restriction (mean difference, −3.88 kg, −6.54 to −1.21 kg), increased physical activity (−4.01 kg, −5.79 to −2.23 kg), and follow up longer than 6 months (−2.69 kg, −3.99 to −1.38 kg). No study reported significant weight gain with a Mediterranean diet.
Conclusions:
Mediterranean diet may be a useful tool to reduce body weight, especially when the Mediterranean diet is energy-restricted, associated with physical activity, and more than 6 months in length. Mediterranean diet does not cause weight gain, which removes the objection to its relatively high fat content. These results may be useful for helping people to lose weight.
Introduction
Materials and Methods
Data sources
We followed the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) checklist for reporting systematic reviews and meta-analyses. 8 We searched PubMed, Embase, Scopus, and the Cochrane Central Register of Controlled Trials databases from inception to January, 2010, using a search strategy that included both truncated free text and exploded MeSH terms. MeSH headings included “Mediterranean,” “diet,” “dietary pattern,” “obesity,” “overweight,” “body weight,” “body mass index,” “weight loss,” “randomized trial,” and “controlled clinical trial.” The search strategy had no language restrictions. We also consulted references from the extracted articles and reviews to complete the data bank. We assessed the relevance of studies by using a hierarchical approach based on title, abstract, and the full manuscript.
Study selection
We included RCTs that reported the effects of a Mediterranean diet on body weight, which could be either the primary or a secondary outcome. We also included RCTs with a crossover design. Trials were excluded in the case of lack of randomization, lack of a control diet group, samples with less than 15 patients, or a follow up less than 4 weeks. We excluded reviews, editorials, comments, letters, abstracts, and studies that performed a post hoc analysis of previous published trials, already selected for this review. The principal outcome measures included change in body weight and body mass index (BMI); we used two overlapping outcome measures as some studies reported only one measure.
Figure 1 shows a flow diagram of how we selected relevant trials. A total of 290 articles were identified after searching the databases and hand searching relevant bibliographies. After excluding 266 articles that did not satisfy the selection criteria described in the articles' “Methods” section, we reviewed the full texts of 24 articles. Of these, 8 were excluded for the following reasons: Lacking a control group (n = 4); the study population consisted of less than 15 subjects (n = 3); and the study was a post hoc analysis (n = 1). We included 16 RCTs 11 –26 in the final analysis.
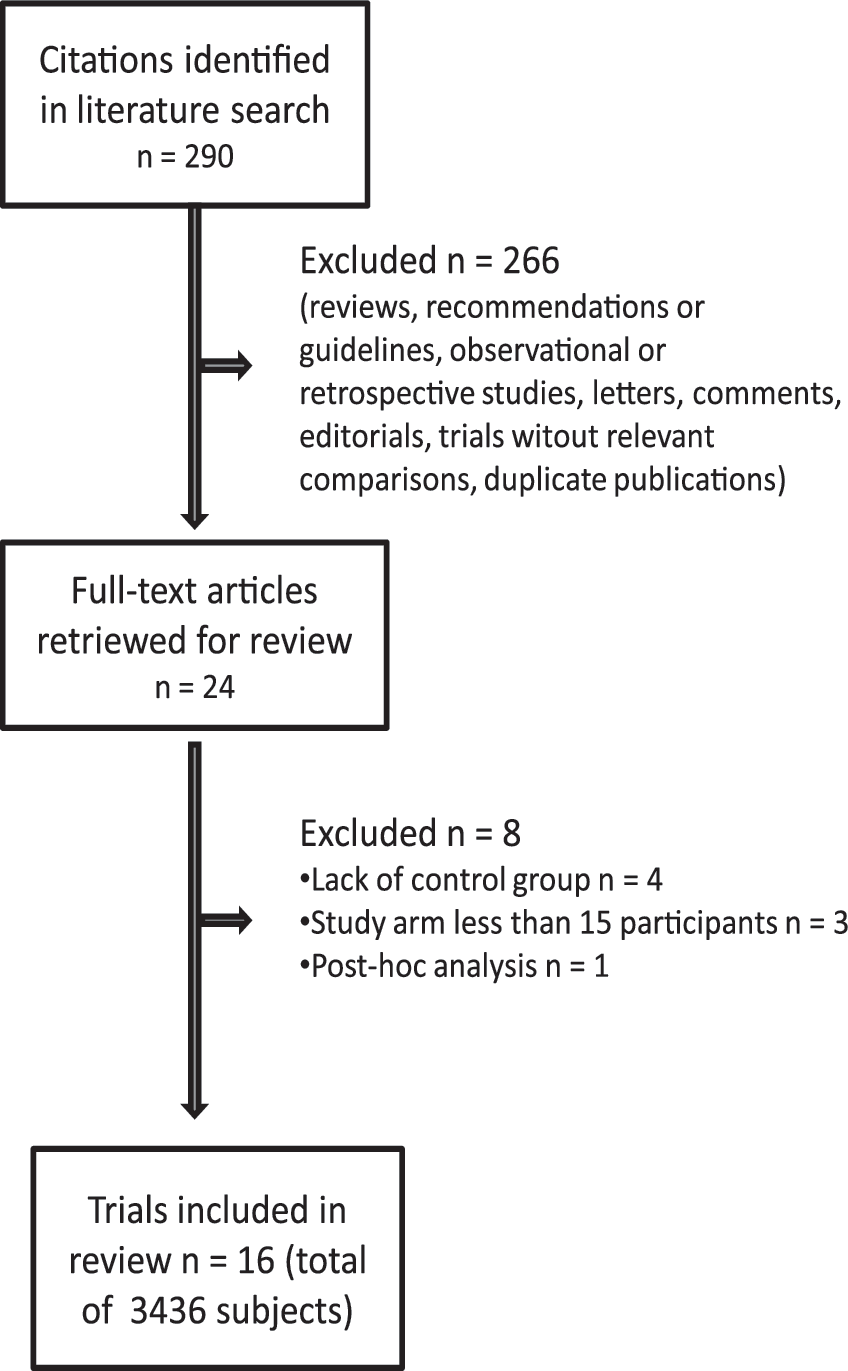
Flowchart of identification of relevant randomized controlled trials (RCTs).
Data extraction
Two investigators (D.G., K.E.) independently assessed the eligibility of all studies retrieved from the databases. Disagreements were solved by consensus and by the opinion of a third author (C-M.K.), if necessary. From the trials included in the final analysis, we extracted the following data: Study name (along with name of the first author and year of publication), country of origin, follow-up period, number of participants, content of intervention and control conditions, outcome measures (kilograms and body mass index), and percentage of lost to follow up in both intervention and control groups.
We assessed the methodological quality of the trials based on a validated scale for RCTs developed by Jadad et al. 9 This 5-point quality scale includes points for randomization (described as randomized, 1 point; table of random numbers or computer-generated randomization, additional 1 point), double-blind (described as double-blind, 1 point; use of masking such as identical placebo, additional 1 point), and follow-up (the numbers and reasons for withdrawal in each group are stated; 1 point) in the report of an RCT. We gave an additional point if the analysis was by intention-to-treat. We considered scores of 2 or less as low quality, and a score of 3 or more as high quality, because none of the studies were double-blinded, which is difficult with this type of intervention.
Statistical analysis
Random effects meta-analysis of the selected trials was applied based on within-trial comparisons, thereby avoiding any biases being caused by methodological differences between trials. Each trial was represented by a dummy variable and the use of a random-effects model was possible, because standard errors of the point estimates within studies were given in the text. Each data point consisted of the BMI or weight loss (end point) and the corresponding relative risk. The validity of the models was examined using the influence of each separate data point (i.e., trial) on the estimated regression coefficients. The later was assessed with the use of the Cook distance to detect possible outliers; a cut-off of Cook distance greater than 0.3 was used to detect studies that caused nonnormality of the residuals. The standard error of the log-risk-ratio or log-odds ratio in each trial was estimated from the number of standard errors by which the reported relationship differed from zero. Confidence intervals (CI) were obtained by normal approximations to the log-relative risk or log-odds, with 95% CI used for the overall results. Heterogeneity of the effect across studies was assessed by the Q 2 statistics, which is distributed as a χ2 statistics. An I2 value greater than 50% was considered substantial heterogeneity. A P value <0.10 was used to indicate lack of homogeneity among effects.
Subgroup analyses were performed to explore heterogeneity. We evaluated the effects of Mediterranean diet according to energy restriction of the diet (yes vs. no), recommended increased physical activity (yes vs. no), initial BMI (≥30 vs. <30 kg/m2), gender (males <50% vs. females ≥50%), and follow-up period (≥6 months vs. <6 months). To investigate the influence of each individual trial on the overall summary estimate, we conducted an influence analysis. In this analysis, the meta-analysis estimates were computed, omitting one trial in each turn. Publication bias was evaluated using the Begg funnel plot and Egger test. 10 If publication bias exists, the funnel plot is asymmetrical or the P value is found to be less than 0.05 by Egger test. We used Stata SE software (version 10.0; StataCorp, College Station, TX) for statistical analysis.
Results
Characteristics of RCTs
Figure 1 shows a flow diagram of how we selected relevant trials. A total of 290 articles were identified after searching the databases and hand searching relevant bibliographies. After excluding 266 articles that did not satisfy the selection criteria described in the articles' “Methods” section, we reviewed the full texts of 24 articles. Of these, 8 were excluded for the following reasons: Lacking a control group (n = 4); the study population consisted of less than 15 subjects (n = 3); and the study was a post hoc analysis (n = 1). We included 16 RCTs 11 –26 in the final analysis.
The 16 RCTs included a total of 3,436 participants: 1,848 assigned to a Mediterranean diet and 1,588 to a control diet. The characteristics of the 16 RCTs and the dietary regimens are shown in Table 1. There were 19 arms, as two trials 20,25 evaluated the effect of two types of Mediterranean diet and one trial 22 compared a Mediterranean-type diet versus two other diets. The selected trials were reported from 1994 through 2010, spanning 16 years. The countries in which the trials were conducted were as follows: The United States, 12,14,21 Italy, 13,17,24 Spain, 15,16,20 France, 11,18 Israel, 22,25 Greece, 23 Germany, 19 and The Netherlands. 26 The range of follow-up periods was 4 weeks to 24 months. Scores of methodological quality was generally high (median score = 3.5, range 1–4). In most trials, the control diet was a low-fat diet, 11,12,18,20 –22,24 a high-carbohydrate diet, 15,16 a prudent diet, 13,17 the usual patient treatment, 14 the American Diabetes Association diet, 25 a high-saturated fat diet, 26 a general healthy dietary information, 19 or less counseling on a Mediterranean diet prescription. 23 Reports of the trials showed variable outcomes. In particular, one trial 25 did not report data on BMI, and four trials 14,18,19,21 did not report data on weight change in kilograms. Moreover, four RTCs with five arms involved energy-restricted diets 12,13,22,24 and eight trials recommended to increase physical activity. 12 –14,17,19,21,24,25 The two small trials 15,16 with a crossover design did not include a washout period, which could lead to an underestimation due to a carryover effect.
Data are mean [standard deviation (SD)]. The numbers in the second column represent the total numbers of participants in the study, and the numbers of participants in each arm. N.S., Not-significant at P < 0.05.
Numbers refer to Mediterranean diet versus control diet.
M/F, male/female; Med, Mediterranean; BMI, body mass index; MUFA, monounsaturated fatty acids; CI, confidence interval; CHO, carbohydrates; SFA, saturated fatty acids; PUFA, polyunsaturated fatty acids; Pro, proteins; CAD, coronary artery disease; CV, cardiovascular; ADA, American Diabetes Association.
Main outcomes
In the Mediterranean diet group, BMI loss was significantly greater compared with the control diet group (mean difference between Mediterranean diet and control diet, −0.57 kg/m2; 95% CI, −0.93 to −0.21 kg/m2) with significant heterogeneity [Cohran Q = 197.42, degrees of freedom (df ) = 15, I2 = 91.45, P < 0.001] (Fig. 2). There was no evidence for publication bias in the selected trials (the Begg funnel plot was symmetrical; for the Egger test, P for bias = 0.14). Figure 3 shows the analysis considering all trials that reported weight change as an outcome. In the Mediterranean diet group, weight loss was greater compared with the control diet group (mean difference, −1.75 kg; 95% CI, −2.86 to −0.64 kg), with significant heterogeneity (Cohran Q = 275.64, df = 13, I2 = 94.93, P < 0.001). There was no evidence for publication bias (P for bias = 0.24). No trial reported weight gain with a Mediterranean diet respect to the control diet.
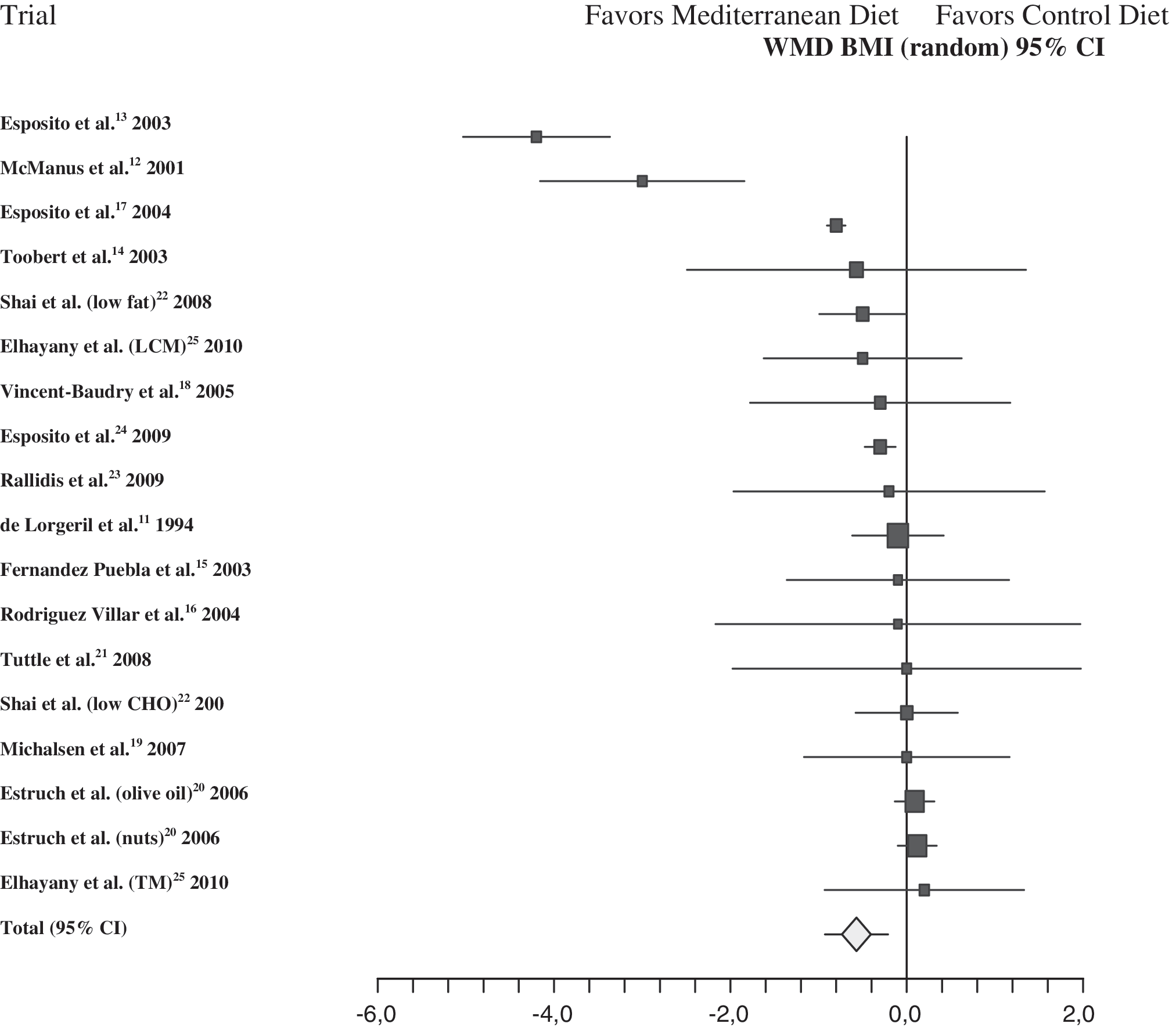
Forest plot of randomized controlled trials (RCTs) assessing the effect of the Mediterranean diet on body mass index (BMI) (kg/m2). Squares represent effect size (weighted mean difference between Mediterranean diet and control diet); extended lines show 95% confidence intervals; diamond represents total effect size. There are 18 arms coming from 15 RCTs. One trial 26 did not report BMI. The two arms of the study of Shai et al. 22 compared the effect of a Mediterranean diet versus a low-fat diet or a low-carbohydrate diet (low CHO); Elhayany et al. 25 compared a low-carbohydrate Mediterranean diet (LCM) or a traditional Mediterranean diet (TM) versus the American Diabetes Association (ADA) diet. Estruch et al. 10 evaluated the effect of two Mediterranean diets (olive oil or nuts) versus a low-fat diet.
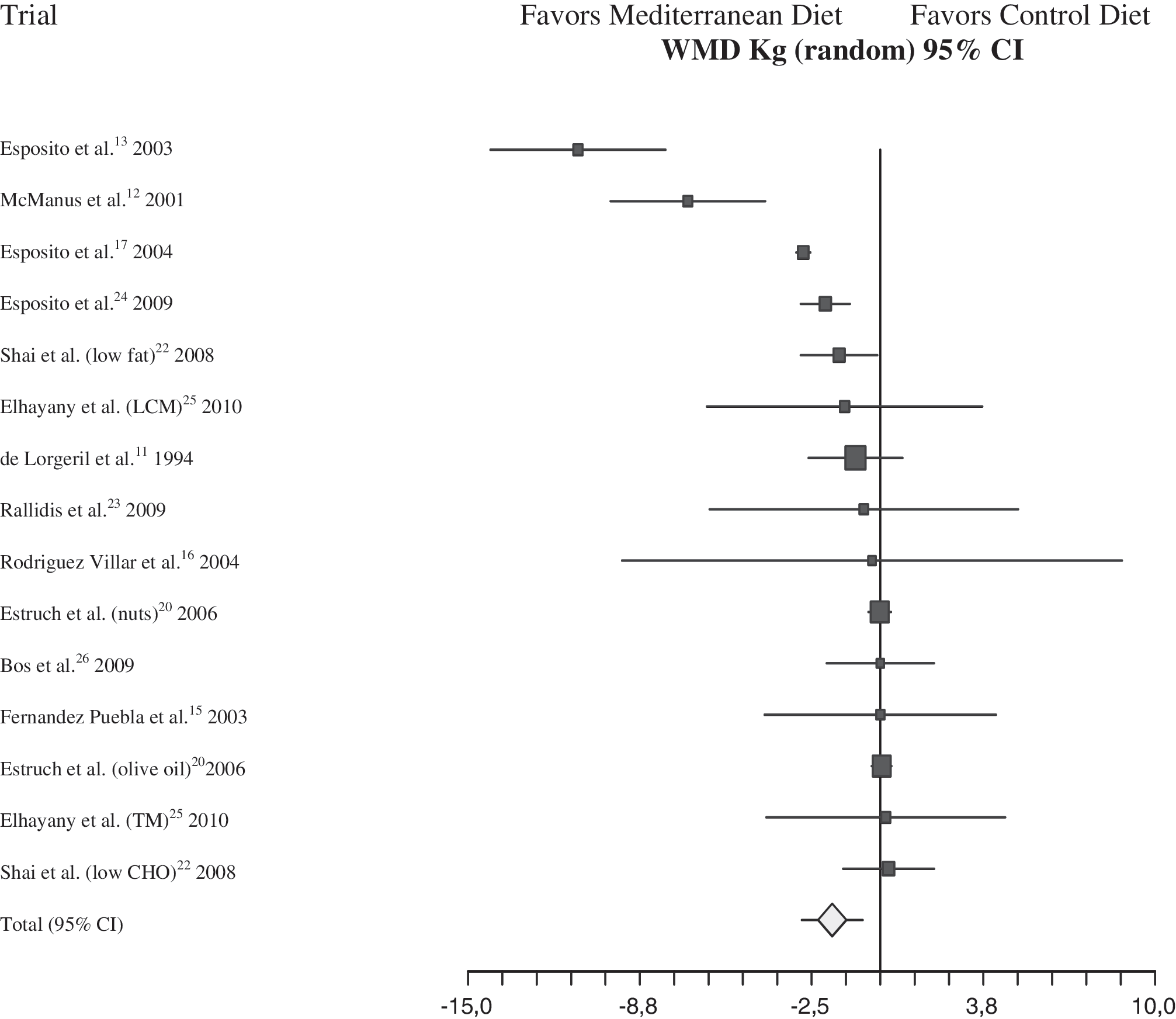
Forest plot of RCTs assessing the effect of the Mediterranean diet on weight (kg). Squares represent effect size (weighted mean difference between Mediterranean diet and control diet); extended lines show 95% confidence intervals; diamond represents total effect size. There are 15 arms coming from 12 RCTs. Four trials 14,18,19,21 did not report data on weight in kilograms.
Sensitivity analyses
Table 2 shows the effect of a Mediterranean diet on body weight (kg) and BMI (kg/m2) in subgroup analyses by energy restriction, physical activity, initial BMI, gender, and follow-up period. The effect of a Mediterranean diet was no longer statistically significant when diet was not associated with energy restriction or increased physical activity, and in trials with a shorter follow-up (≤6 months). Regarding BMI at baseline, there was a trend for a greater BMI loss with a Mediterranean diet in obese subjects, probably owing to the greater number of subjects evaluated. However, large I2 values, indicating heterogeneity, were observed in these analyses (P < 0.01). An influence analysis showed that omission of any individual study made no difference in outcomes (weight or BMI) when its graph was visually interpreted. Moreover, the exclusion of the two small studies with a crossover design reinforced the outcomes (mean difference, −1.80 kg; 95% CI, −2.91 to −0.72 kg).
Significant heterogeneity (P < 0.01).
Discussion
This meta-analysis of 16 RCTs shows that consumption of a Mediterranean diet causes greater weight loss as compared with a control diet. In the overall analysis, the mean weight loss was 1.75 kg; however, the effect of the Mediterranean diet on body weight was greater in association with energy restriction (−3.88 kg) or increased physical activity (−4.01 kg). Moreover, in none of the 16 RCTs did a Mediterranean diet cause significant weight gain compared with the control diet. To our knowledge, this is the first quantitative meta-analysis that has evaluated the effect of a Mediterranean diet on body weight in subjects with a wide range of co-morbidities.
Diet and overweight
The relatively high content of fat (up to 40%) of the Mediterranean diet might be a topic of concern, partly due to the possible effect on weight gain. However, there is evidence that high-fat diets are not the major cause of obesity, because no significant relation between diets with greater fat content and obesity has been found. 27,28 This view has recently been confirmed by the data of six cohorts of the EPIC study, including 89,432 men and women. 29 No significant association was found between the amount or type of dietary fat and subsequent weight change in this large prospective study. Moreover, no clinical trial included in our analysis reported increased weight gain with a Mediterranean diet as compared with a control diet, despite the intake of monounsaturated fatty acids (MUFA) may be so high to cover about one-quarter of the daily caloric intake. 23 One important challenge is to prevent weight gain and weight regain after weight loss. Due et al. 30 compared the effects of three ad libitum diets (high fat diet with >20% of MUFA, low-fat diet with 20–30% of energy from fat, and a control diet) on the maintenance of an initial weight loss in 131 overweight subjects followed for 6 months. Although all groups regained weight, body fat regain was lower in both low-fat and MUFA diet groups, as compared with the control group.
Practical implications
Increased energy intake appears to be more than sufficient to explain weight gain, at least in the U.S. population. 31 Interventional studies assessing the role of diet on weight loss may be polluted by different macronutrient composition, but there is no agreement. Howard et al. 32 reported that weight loss was greatest among women who decreased their percentage of energy from fat; Shai et al. 22 showed that a low-carbohydrate diet was superior to a low-fat diet for weight loss; and Sacks et al. 33 showed that reduced calorie diets caused weight loss independent of macronutrient composition. Our analysis indicate a greater effect of Mediterranean diet on weight independent of energy intake; on the other hand, energy restriction amplified the weight loss induced by a Mediterranean diet, pointing to a synergistic interaction between the specific nutritional value of the Mediterranean diet and cutting of daily calories. Of the five arms of the four RCTs that assessed Mediterranean diets with energy restriction, 12,13,22,24 all but one 12 reported more weight loss with a Mediterranean diet, as compared with the control diet, at the same level of energy intake and physical activity. Many components of Mediterranean diets may, in theory, favor weight loss, including abundance of plant-based foods that provide a large quantity of dietary fiber, low energy density, low glycemic load, and high water content. 5 Regardless of the mechanisms involved, and given the few current options for the pharmacological treatment of obesity, any successful dietary strategy for fighting overweight could be important and of public utility.
Limitations
Our study has several possible limitations. The interventional Mediterranean diet varied between the clinical trials, also in terms of level of detail of the recommendations and amount of time spent explaining the Mediterranean diet in one study. 23 Moreover, the control diet also varied between trials. The degree of heterogeneity was high, which may introduce a bias about the generalization of the results. However, in most cases results were qualitatively similar across studies in terms of directions of effect, even in the presence of large I2 values. Although sensitivity analysis could identify some source of heterogeneity, residual significant heterogeneity was present. However, the role of heterogeneity in medicine is being actively discussed. 34
Conclusions
This meta-analysis shows that the Mediterranean diet may be a useful tool to reduce body weight, especially when the Mediterranean diet is energy-restricted, associated with physical activity, and with a follow-up of more than 6 months. Moreover, the evidence is univocal, indicating that Mediterranean diet does not cause weight gain, which removes the objection to its relatively high fat content. Considering the beneficial effects of the Mediterranean diet on cardiovascular outlook 1 and perceived health status, 35 these results may be useful for reducing the risk of weight gain in the general population or for helping people to lose weight.
Footnotes
Author Disclosure Statement
No competing financial interests exist for all authors.
Author contributions were as follows: Dr Esposito and Giugliano had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Esposito and Giugliano. Acquisition of data: Esposito, Giugliano, Kastorini and Panagiotakos. Analysis and interpretation of data: Esposito, Giugliano, Kastorini and Panagiotakos. Drafting of the manuscript: Esposito, Giugliano, Kastorini and Panagiotakos. Critical revision of the manuscript for important intellectual content: Esposito, Giugliano, Kastorini and Panagiotakos. Statistical analysis: Kastorini and Giugliano. Administrative, technical, and material support: Esposito and Giugliano. Study supervision: Esposito, Giugliano and Panagiotakos.