
Abstract
Aims:
Obstructive sleep apnea/hypoapnea syndrome (OSAHS) and metabolic syndrome are both growing health concerns, owing to the worldwide obesity epidemic. This study evaluates the potential association between the parameters of metabolic syndrome and OSAHS.
Methods:
A total of 125 consecutive patients undergoing complete full night polysomnography were included. Insulin resistance (IR) was estimated using the homeostasis model assessment (HOMA), and metabolic syndrme was diagnosed according to the National Cholesterol Education Program (NCEP) criteria.
Results:
The prevelance of metabolic syndrome was 23.8% among patients with OSAHS. We found that IR, age, weight, hypertension, and metabolic syndrome prevalence increased significantly with severity of OSAHS. There were no differences between groups for lipid panels including total cholesterol, triglycerides, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C). Subjects with metabolic syndrome had significantly lowest desaturation value (76% vs. 81%) desaturation (76% vs. 81%, P = 0.003), lower mean nocturnal oxygen saturation (89.9% vs. 92.3%, P < 0.00.1), higher apnea–hypopnea index (AHI) (40.9 vs. 17, P < 0.001), and higher oxygen desaturation index (38 vs. 17, P = 0.002). Lowest desaturation and mean nocturnal oxygen saturation were significantly lower in subjects with IR (76% vs. 85%, P = 0.004 and 90.4% vs. 93.0%, P = 0.02). In multivariate analysis, the percent of time below 90% saturation [%T < 90]) (P = 0.04) was independently associated with IR.
Conclusions:
Our results suggested that metabolic syndrome prevalence increased with severity of OSAHS and vice versa. Nocturnal hypoxic episodes in OSAHS patients could be a risk factor for developing hypertension and IR.
Introduction
Metabolic abnormalities can affect sleep regulation, and sleep problems may interfere with endocrine function and metabolic conditions. Obstructive sleep apnea/hypopnea syndrome (OSAHS), which is characterized by loud snoring, disrupted sleep, and observed apneas, can lead to chronic intermittent hypoxia (CIH) with increased sympathetic activation and insulin resistance during sleep. 3 –6 Obese subjects are at increased risk of developing OSAHS; however, upper airway anatomical features are also determinative for OSAHS. Marin et al. found that severe untreated OSAHS is associated with an increased risk of cardiovascular mortality, defined by fatal myocardial infarction or stroke [odds ratio (OR), 2.87]. 7 Recent guidelines for the management of hypertension have stressed the importance of OSAHS, and the International Diabetes Federation (IDF) published a consensus statement on sleep apnea and type 2 diabetes mellitus (T2DM). 8,9 Despite substantial evidence from both clinical and population studies suggesting an independent link between OSAHS and metabolic abnormalities, the influence of OSAHS on metabolic syndrome and its components has not been clarified.
The aim of our study was to determine the prevalence of metabolic syndrome in patients with OSAHS and also the influence of CIH and OSAHS severity (apnea–hypopnea index (AHI), lowest oxygen saturation level, oxygen desaturation index, and percent of time below 90% saturation) on components of metabolic syndrome.
Methods
Subjects
A total of 125 consecutive patients who underwent a polysomnography test in our Sleep Disorders Center were included to the study. Oral informed consent for the study was obtained from all patients. The presence or a history of hypertension, diabetes mellitus, or dyslipidemia was recorded. To be eligible for the study, patients had to fulfill the following criteria: No history and clinical signs of heart failure, autoimmune disease, acute inflammatory disease, or any severe disease shortening life expectancy, such as diagnosed cancer, chronic liver disease, and severe renal disease. After polysomnography, 105 patient were considered to have OSAHS (AHI >5), and 20 subjects that were considered not to have OSAHS (AHI <5) were enrolled as a control group.
All the participants' height, weight, neck, and waist circumferences were measured by the same person with using the same equipment. Weight was measured by using a calibrated hospital scale with subjects dressed in normal indoor clothing without shoes. Height was measured against a wall using a fixed tape measure with subjects standing shoeless on a hard surface in centimeters. Body mass index (BMI) was calculated by dividing body weight by height squared (kg/m2).
Blood pressure was also recorded after at least 5 min of rest in a chair, with feet on the floor and the arm supported at heart level, using a mercury sphygmomanometer. All blood samples were obtained in the morning after a 12 h overnight fast. Fasting glucose, total cholesterol, triglyceride, and high-density lipoprotein cholesterol (HDL-C) were measured, and fasting insulin sensitivity was estimated using the homeostasis model assessment of insulin resistance (HOMA-IR) 10 in all patients. The value of HOMA was calculated by the following equation: [fasting insulin (μU/mL) × fasting glucose (mmol/L)]/22.5 and depicted as the HOMA-IR value. Diagnosis of IR was made if the patient had a HOMA-IR value >2.3 or had a previous history of diabetes mellitus. 11
Definition of metabolic syndrome
Metabolic syndrome was diagnosed according to the National Cholesterol Education Program Expert Panel on Detection, and Treatment of High Blood Cholesterol in Adults (NCEP III) criteria. 8 A diagnosis of metabolic syndrome was made if the patient met at least three of the following criteria: (1) Fasting plasma glucose ≥100 mg/dL (or presence of diabetes mellitus); (2) blood pressure ≥130/85 mmHg or current use of antihypertensive drugs; (3) triglycerides ≥150 mg/dL; (4) HDL-C <40 mg/dL and 50 mg/dL in men and women; (5) waist circumference in men >102 cm, in women >88 cm.
Polysomnographical evaluation
Overnight polysomnography (PSG) was recorded with a Grass polysomnogram (Comet XL Lab-based PSG), which recorded the following parameters: Electrocardiogram; central, temporal, and occipital electroencephalogram; bilateral electrooculogram; submental and anterior tibialis electomyogram; nasal airflow using a nasal cannula and pressure transducer; nasooral airflow using a thermistor; and respiratory effort using chest and abdominal piezoelectric belts. The electromyelogram, electrooculogram, and electroencephalogram leads were applied according to the international 1020 electrode placement system. Oxyhemoglobin saturation (SpO2) was monitored using a pulse oximeter (Biox 3740; Ohmeda: Louisville, CO). Sleep staging was scored according to the criteria of American Academia of Sleep Medicine (AASM) published in 2007. 12 Apneas were defined as decrements in airflow ≥90% from baseline for ≥10 sec. Hypopnea were defined as a 30% or greater decrease in flow lasting at least 10 sec and associated with a 4% or greater oxyhemoglobin desaturation. The number of apneas and hypopneas per hour of sleep were calculated to obtain the AHI. Respiratory events were derived primarily from the nasal cannula pressure transducer. The oxygen desaturation index (ODI) was defined as the total number of episodes of oxyhemoglobin desaturation ≥4% from the immediate baseline, ≥10 sec but <3 min, divided by the total sleep time. Severity of OSAHS was measured by AHI, ODI, minimum oxygen saturation (SaO2), time duration with SaO2 < 90% during sleep.
Statistical analysis
All results were expressed as means ± standard deviation (SD) values. Comparisons on continuous variables were made using the Student t-test or Wilcoxon–Mann–Whitney test. Categorical variables were compared using a chi-squared or Fisher exact test. Pearson simple linear regression and correlation analysis were used to evaluate the interrelationship between parameters. A P value of <0.05 was considered significant for all analyses, which were performed with SPSS version 13.0 software (SPSS Inc., Chicago, IL).
Results
In this study, a total of 125 patients (90 male, 35 female, mean age 50.3 ± 13.1 years, BMI 31.9 ± 6.7 kg/m2 (min = 21.9, max = 44.8), fasting serum glucose 98.1 ± 16.2 mg/dL, fasting serum triglycerides 157.1 ± 69.4 mg/dL, 32.8% hypertension, and 16.8% diabetes mellitus) with detailed PSG data and biochemistry were included.
According to AHI value, 20 patients had AHI <5 and were considered as normal, 17 patients had AHI values between 5 and 14.9 and were considered as having mild OSAHS, 24 patients had AHI values between 15 and 29.9 and were considered as having moderate OSAHS, and 54 patients had AHI values ≥30 and considered as having severe OSAHS. The prevalence of metabolic syndrome was 23.8% among patients with OSAHS. In the non-OSAHS group, the prevalence of metabolic syndrome was 10%, and this reached with an increasing prevalence up to 37% in severe OSAHS. We found that IR, age, prevalence of hypertension, and metabolic syndrome increased with severity of OSAHS (Table 1). Weight, neck, and waist circumferences also increased with severity of OSAHS (Fig. 1). In the present study, the prevalence of visceral obesity in snorers and in mild, moderate, and severe OSAHS patients was 35%, 66.7%, 79.2%, and 90.7%, respectively (P = 0.001). We could not find any effect of gender on both the presence of OSAHS and metabolic syndrome (P > 0.05). There were no differences between groups for lipid panels, including total cholesterol, triglycerides, low-density lipoprotein cholesterol (LDL-C), and HDL-C.
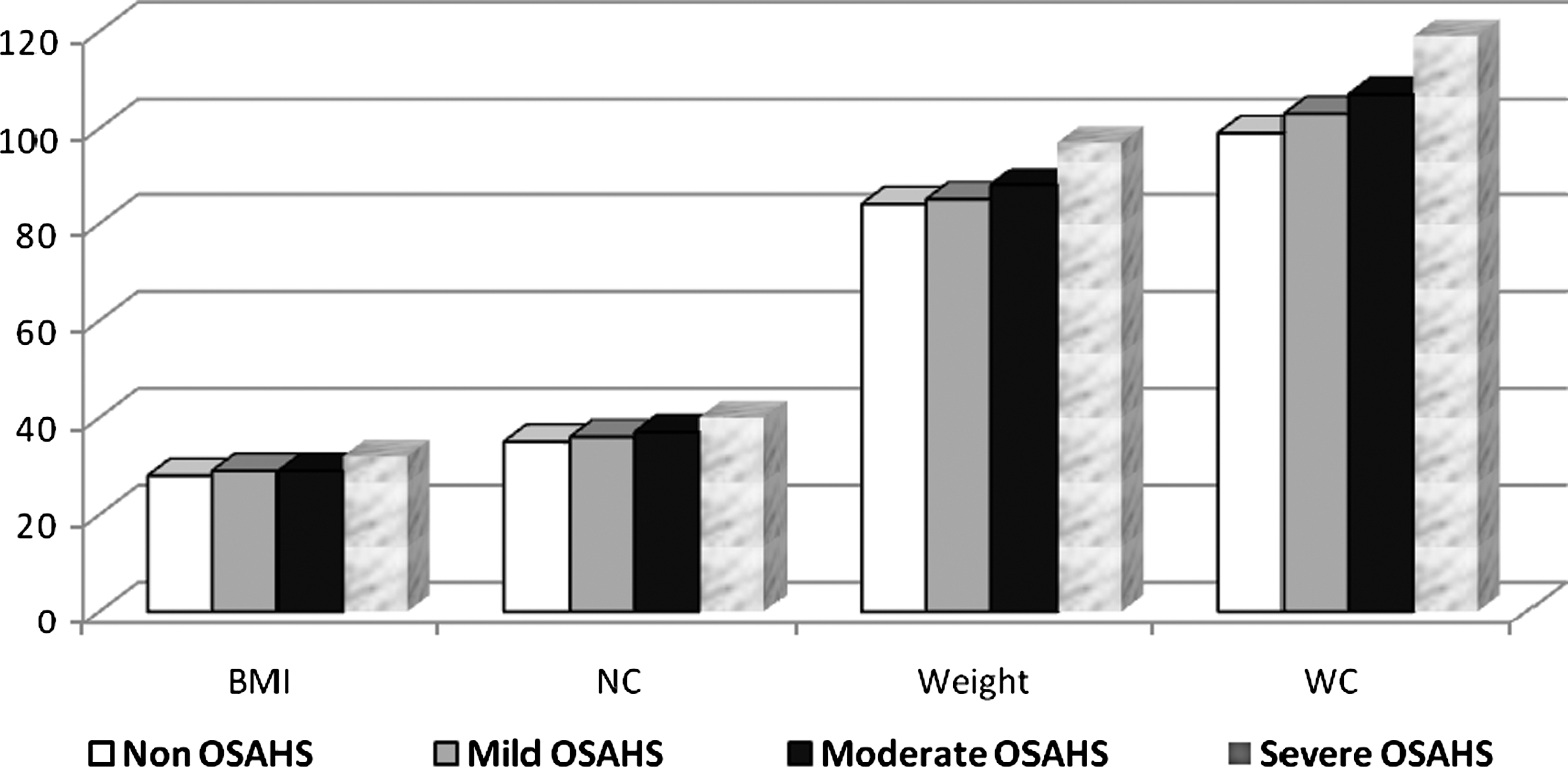
Relationship between OSAHS severity and obesity parameters. OSAHS, obstructive sleep apnea/hypopnea syndrome; BMI, body mass index; NC, neck circumference; WC, waist circumference.
Difference between the non-OSAHS group and severe OSAHS group is statistically significant (P < 0.05).
Difference between the mild OSAHS group and severe OSAHS group is statistically significant (P < 0.05).
Difference between the moderate OSAHS group and severe OSAHS group is statistically significant (P < 0.05).
Difference between the non-OSAHS group and moderate OSAHS group is statistically significant (P < 0.05).
OSAHS, obstructive sleep apnea/hypoapnea syndrome; HOMA, homeostasis model assessment; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Total 27 patients had metabolic syndrome according to NCEP criteria. Patients with metabolic syndrome are older than patients without metabolic syndrome, and all of their oxygen saturation parameters were significantly worse than patients without metabolic syndrome (Table 2). We found that metabolic syndrome was associated with CIH during sleep.
AHI, apnea–hypopnea index; ODI, oxygen desaturation index.
Insulin resistance as calculated by HOMA-IR was significantly higher in severe OSAHS patients. The percentages of patients with a high level of HOMA were 45.5%, 42.1%, 36.8%, and 62.8% for snorers and mild, moderate, and severe OSAHS, respectively. We could not find any effect of gender on IR (P = 0.513). There was statistically significant interaction between IR and AHI values. The only percent of time below 90% saturation remained significant after adjustment for weight and body mass (Table 3). The prevalence of hypertension also increased with severity of OSAHS (Fig. 2).

Relationship between prevalence of hypertension and severity of OSAHS. OSAHS, obstructive sleep apnea/hypopnea syndrome.
Remained significant after adjustment for weight and body mass index.
AHI, apnea hypoapnea indexl; ODI, oxygen desaturation index.
Discussion
These findings suggested that metabolic syndrome prevalence increased with severity of OSAHS and vice versa. Severe OSAHS was an important risk factor for hypertension and IR. Also patients with metabolic syndrome had more severe OSAHS and more severe hypoxia during sleep.
The AHI is commonly used to define the severity of OSAHS. However, the AHI cannot be considered as the best or only marker of OSAHS severity, because it does not provide information on the degree of oxygen desaturation. The CIH in OSAHS closely mimics what is seen in the ischemia–reperfusion injury. 4 CIH can lead to a systemic inflammation with endothelial injury, thus it seems to be the hallmark of OSAHS-related events. For this reason, the oxygen desaturation index and percent of time below 90% saturation are also important in addition to the AHI. Our findings are consistent with previous studies performed in sleep disorders clinics demonstrating the vicious cycle fed by OSAHS and metabolic syndrome. 13 In a retrospective review of 250 consecutive patients referred to a sleep disorders Center in the United States, 14 the prevalence of metabolic syndrome was significantly higher in patients with OSAHS. In our study patients, the prevalence of OSAHS was higher in metabolic syndrome patients as compared with those without, and patients with metabolic syndrome also had significantly worse oxygen saturation parameters than patients without metabolic syndrome. We found a parallel increase between metabolic syndrome and its components with AHI and ODI. In our study, metabolic syndrome was 3.7 times more likely to be present in subjects with AHI ≥30. Similarly Coughlin et al. 15 showed that OSAHS was independently associated with an increased prevalence of metabolic syndrome, and they found the prevalence of metabolic syndrome was about 40% greater in patients with OSAHS. OSAHS may be contributing to and/or modulating the severity of components of metabolic syndrome.
Obesity is defined as an increase in body weight resulting from excessive body fat, and a rise in the prevalence of metabolic syndrome seems to have occurred over the same time period with obesity. Also it is known that obesity, in particular visceral obesity, is strictly connected with OSAHS. 16,17 Apnea–hypopnea episodes and oxygen desaturation have been correlated to narrowed upper airway dimensions due to the fatty tissue deposits within the airway walls, which increase the collapsibility of the pharyngeal lumen. We also found that both weight and waist circumferences were significantly associated with OSAHS patients with a prevalence reaching to 90.7% in patients AHI >30. Visceral obesity, however, is also associated to metabolic syndrome, 8 which in turn may induce OSAHS; thus, it seems difficult to define which is the cause and which the consequence.
The most important underlying mechanism in metabolic syndrome is insulin resistance. Insulin resistance is usually evaluated by fasting insulin levels, the Quantitative Insulin Check Index (QUICKI), HOMA-IR, C-peptide/insulin ratio, oral glucose tolerance test, and hyperinsulinemic euglycemic clamp. 18 Because IR measurement is complex and expensive, the model proposed by Mathews estimating the degree of insulin resistance at baseline by the HOMA-IR has acquired importance. In our study, we calculated the HOMA-IR index in all of our patients to establish glucose intolerance better and found that subjects with IR had significantly worse nocturnal oxygen values and, in multivariate analysis, the percent of time below 90% saturation was independently associated with IR. Our results suggested that the frequent nocturnal hypoxic episodes in OSAHS patients might contribute to developing IR. Similarly, in the Sleep Heart Health Study that covers 2,656 research subjects, the prevelance of diabetic impaired 2 hour glucose values rose from 9.3% to 15%, in subjects with AHI of <5 and with AHI of >15 respectively, correlations were also noted for the degree of oxygen desaturation at night. 19 In healthy subjects, experimental sleep restriction caused insulin resistance and increased evening cortisol and sympathetic activation. 20 However Davies 21 and Sharma 22 could not find an association between sleep apnea and insulin resistance. On the other hand both Punjabi 23 and Ip 24 found that severe OSAHS is associated with insulin resistance in individuals and may contribute to progression of insulin resistance to T2DM. In the Wisconsin Cohort Study, subjects with OSAHS were no more likely to develop diabetes mellitus than subjects without OSAHS. 25
The reason for these conflicting results could be the use of various techniques for the assessment of glucose metabolism and differences in study populations. Also studies looking at the effect of treatment of OSA on insulin resistance have also produced contradictory reports that can be explained by discrepancies in treatment compliance and methodological differences. However, the high prevalence of OSAHS among patients with T2DM, 7 coupled with the relentless rise in the prevalence of diabetes worldwide, 8 has led the IDF Task Force on Epidemiology and Prevention to publish a consensus statement on sleep apnea and T2DM. 9 The report makes recommendations for screening patients with T2DM for OSAHS, and conversely, it also recommends that all patients with known OSAHS should be screened for hyperlipidemia, hypertension, and T2DM.
Recent epidemiologic and clinical data suggest a causal role of severe OSAHS in development of hypertension. 26 –28 There is a strong interaction between hemodynamic and inflammatory changes in promoting vascular remodeling. 29,30 In our study, more than half of severe OSAHS patients had hypertension and AHI >30 increased the risk of hypertension 2.5 times. Similarly Angelico et al. 31 found that 84.8% patients with severe OSAHS had hypertension. In the Wisconsin Sleep Cohort Study covering 709 patients, odds ratios for developing systemic hypertension were found to be 1.42, 2.03, and 2.89 for patients with AHI <4.9, AHI between 5 and 14.9, and AHI >15, respectively, in a 4-year follow-up period. 32 Effective treatment of OSAHS with continuous positive airway pressure reduces the elevated inflammatory markers and causes significant fall in blood pressure. 33 OSAHS seems to be a risk factor for hypertension and consequent cardiovascular morbidity in the general population.
In summary, it can be assumed that OSAHS affects components of metabolic syndrome and vice versa. A bidirectional association between the two can be postulated. Both clearly share a common risk factor, namely obesity. But also the percentage of time that was spent below 90% saturation during sleep was an important independent risk factor for insulin resistance. So clinicians should be encouraged to systematically evaluate and give treatment for OSAHS symptoms in patients with metabolic syndrome to protect them from nocturnal hypoxia.