
Abstract
Objective:
The present study was designed to assess the impact of intensive and repetitive nutrition education and lifestyle interventions on insulin resistance, β-cell function, disposition index (DI), and subclinical inflammation in Asian Indian adolescents (15–17 years) residing in North India.
Method:
In this prospective study, two matched schools were randomly allocated to the intervention (n = 56; 31 boys and 25 girls) or control group (n = 50; 30 boys and 20 girls). The intervention consisted of seven components: (1) Dissemination of health-related information through lectures and focused group discussions, (2) planning of activities such as quizzes, (3) individual counseling of students, (4) promotion of physical activity, (5) change in the canteen menu to healthier alternatives, (6) conducting health camps involving parents and teachers, and (7) training of student volunteers for sustainability of the program in school. Impact of intervention was studied on surrogate markers of insulin resistance, β-cell function, disposition index, and subclinical inflammation.
Results:
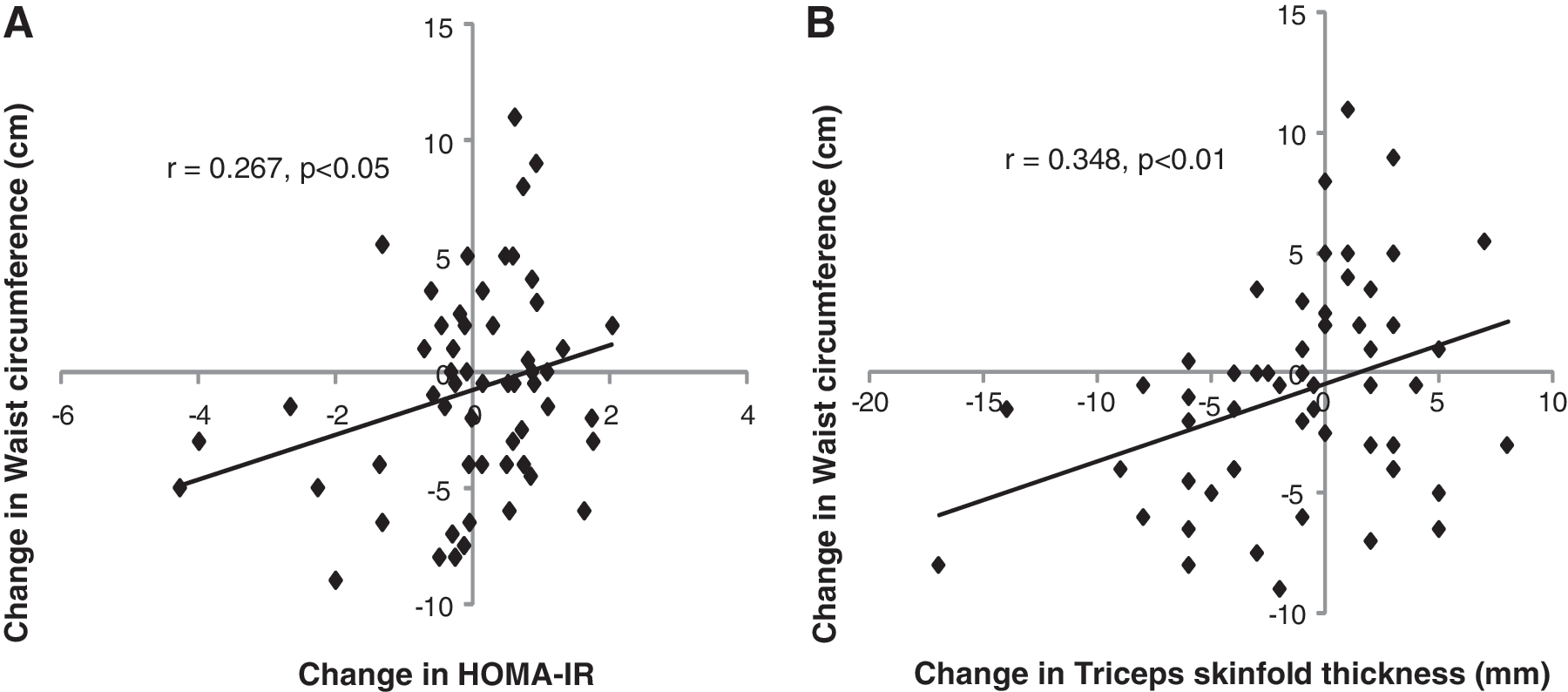
At 6 months follow-up, significantly higher (P = 0.037) mean value of homeostasis model assessment denoting β-cell function (HOMA-βCF) was seen in the intervention group compared to the control group, whereas high sensitivity C-reactive protein (hs-CRP) was significantly lowered (P < 0.001). The increase (30.3 ± 73.4; P < 0.037) observed in the DI in adolescents in the intervention group was significantly higher compared to the control group. The Pearson's coefficient of correlation in the intervention group showed that the Δ-decrease in mean waist circumference was significantly correlated (r = 0.267, P < 0.05) with Δ-decrease in homeostasis model assessment of insulin resistance (HOMA-IR).
Conclusion:
The intervention model developed by us could be used for amelioration of insulin resistance with potential of preventing type 2 diabetes mellitus in Asian Indian adolescents.
Introduction
Schools offer an ideal medium for lifestyle interventions because the obesogenic lifestyle behaviors are less well developed in children and are therefore amenable to change. 2 Moreover, it is important to identify the adolescents at risk for T2DM and CHD at an early age and use appropriate prevention strategies while the pathological processes are still reversible. 10 Prevention of obesity in childhood will also reduce the burden and cost of obesity, T2DM, and CHD in India, particularly because the number of patients with latter diseases in India are one of the highest globally. 11
We hypothesized that intensive and repetitive school-based nutrition education interventions involving parents and teachers would result in beneficial changes in insulin resistance and subclinical inflammation in Asian Indian adolescents. Therefore, the present study was conducted to assess the impact of intensive and repetitive nutrition education and lifestyle interventions on insulin resistance, β-cell function, and subclinical inflammation in a sample of Asian Indian adolescents (15–17 years old) residing in North India.
Methods
Study design, sampling, and sample size
This substudy was a part of large school-based program (MARG, “
Anthropometric measurements
The measurements of height, weight, WC, and TSF thickness were carried out by the same trained nutritionist in both the schools using standard procedures. 14 Results of the complete sample of children (n = 99 in the intervention school and n = 101 in the control school) whose anthropometric data at baseline and follow-up were available have been published previously. 13 This paper gives the anthropometric results of the sample (n = 56, intervention school; n = 50, control school) studied in the present manuscript with the primary aim of correlating it with surrogate markers of insulin resistance, β-cell function, and subclinical inflammation.
Biochemical measurements
Serum insulin and hs-CRP were assayed as previously described. 15 For serum insulin, the intraassay and interassay coefficients of variation were below or equal to 4.3% and 3.4%, respectively. The lower limit of detection was 0.01 μU/mL. The reference range of the assay was 2.1–22 μU/mL. The lowest detectable limit for hs-CRP was 0.005 mg/L, and intra-assay variation (range) was 1.7%–3.3%. The results of fasting blood glucose (FBG) have already been published previously. 13
The gold standard methods for measuring insulin sensitivity and pancreatic β-cell function are the hyperinsulinemic–euglycemic clamp and hyperglycemic clamp, respectively. 16 However, because these procedures are invasive and labor intensive, we used simple surrogate measures that have been shown to correlate with the clamp procedures. 17,18 The values of FBG and fasting insulin have been used to calculate insulin resistance by homeostasis model assessment (HOMA). The value of HOMA denoting insulin resistance was termed as HOMA-IR and was calculated as: [fasting insulin (μU/mL) × fasting glucose (mmol/L)/22.5]. 19 The value of HOMA denoting β-cell function was termed as HOMA-βCF and was calculated as: [20 × fasting plasma insulin (μIU/mL)/fasting plasma glucose (mmol/L) −3.5]. 20 The disposition index (DI) provides a measure of βCF adjusted for insulin sensitivity and was calculated as: Insulin sensitivity [(22.5/fasting insulin (μU/mL) × fasting glucose (mmol/L)] × HOMA-βCF. 21
Nutrition and lifestyle education interventions
Children in the intervention group were provided with nutrition education and lifestyle interventions as previously described, 13 whereas those in the control group were not provided with any intervention. Briefly, the entire nutrition education intervention consisted of seven components and spanned over 24 weeks. The initial 6 weeks were used for introduction of the program to the school and for collecting baseline data. During the remaining 18 weeks, intensive and repetitive nutrition education intervention was delivered to the eleventh-grade students. The individual components of the nutrition education model were: (1) Dissemination of health-related information and lifestyle-related diseases through lectures and focused group discussions for initial 10 weeks. The students were given lectures in batches of 30 in each class in 30-min sessions each week for 10 weeks on the basics of food groups; importance of each food group for health; difference between simple and complex carbohydrates, concept of empty calories and its sources; importance of fiber in the diet; sources and adverse effects of trans-fats; sources of protein in the diet; harmful effects of consuming deep-fried, high-calorie Indian "junk" food everyday; and antioxidant and fiber content of fruits and vegetables and importance of eating nuts. In addition, knowledge of lifestyle-related diseases such as diabetes, cardiovascular disease (CVD), and hypertension was provided to them. (2) Promotion of physical activity in school every week for at least 30 min. (3) Other activities conducted for a period of 8 weeks, including quiz competitions, extempore, planning healthy lunch boxes, planning healthy alternatives to high calorie junk foods. (4) Individual counseling for an hour every week regarding diet, lifestyle, and physical activity with the children in groups of 4–5 by the trained nutritionist (N.S.). (5) Policy-level changes in the school wherein the school canteen menu was changed to healthier alternatives. The sale of aerated drinks and high-calorie foods such as burgers, bread pakodas (deep-fried Bengal gram flour-coated bread slices), and noodles were stopped. Healthy Indian foods providing satiety such as rajmah-chawal (bean curry and boiled rice) kadi-chawal (Bengal gram flour curry and boiled rice), idli-sambar (fermented and steamed rice and pulse flour and red gram dhal with vegetables), and cucumber sandwiches made of whole wheat bread were made available. (6) Involvement of teachers and parents through health camps where they were given free of cost assessment of their BMI, blood pressure, and blood glucose by a physician. Furthermore, parents of each child were counseled by telephone for 5–10 min every month. (7) For sustainability of the program in the school, student volunteers were trained with instructions to disseminate the health messages to their peers and juniors through skits in the morning assembly on nutrition-related topics, checking lunch boxes of junior classes, and demonstration of healthy and easy-to-prepare snacks.
Statistical analysis
The distribution of all quantitative variables was assessed for normal distribution. Variables following non-normal distribution were transformed into normal distribution through log-transformation. Except hs-CRP, all other quantitative variables were normally distributed. BMI was considered as the primary outcome measure in this intervention study. The baseline characteristics of intervention and control group, including log hs-CRP, were compared using independent sample t-test. Except for log hs-CRP, all other variables were statistically comparable between the groups, hence, the difference in mean values of these variables, post-intervention were compared using the two-group independent Student t-test.
Due to imbalance of log hs-CRP between the two groups at baseline, we used the baseline values as confounding factors in the regression analysis to adjust for the difference in the mean values between the two groups post-intervention. In addition, we also compared the baseline and follow-up values of all variables (except hs-CRP, because the baseline values were significantly different between the two groups) in the intervention and control groups using the Student paired t-test, whereas the mean change in the intervention and control groups was compared using the two-sided independent sample Student t-test. The Pearson coefficient of correlation (r) was used to analyze the correlation between changes (Δ) in various parameters in the intervention group. All analysis was based on intention-to-treat principle; i.e., the children were compared in the groups to which they were originally assigned. 22 SPSS (Release 10, SPSS Inc., Chicago, IL) was used for data analysis. The significance level was set as P < 0.05.
Results
The present study consisted of 56 subjects (31 boys and 25 girls) in the intervention school and 50 subjects (30 boys and 20 girls) in the control school for whom the biochemical measurements were available at both baseline and follow-up. It was found that the baseline characteristics of the subjects whose follow-up measurements were not available did not differ significantly from the baseline characteristics of those subjects whose follow-up measurements were available (data not shown). There was no statistically significant difference [P = not significant (N.S.)] in any of the baseline parameters of subjects between the intervention and control groups, except for hs-CRP (P = 0.017) (Table 1). There was no significant difference (P = N.S.) in the mean [±standard deviation (SD)] age (years) of the subjects between the intervention (16.02 ± 0.35) and control groups (16.02 ± 0.55). After 6 months of intervention, no significant change in the primary outcome measure, BMI, was observed between the two groups. However, WC was significantly lowered (P = 0.028) in the intervention group compared to the control group. Importantly, post-intervention, the intervention group had significantly higher HOMA-βCF values (P = 0.037) and significantly lower hs-CRP values (P < 0.001) than the control group (Table 1). Although the postintervention values of DI were not significantly different between the intervention and control groups (Table 1), we found that the increase (30.3 ± 73.4; P < 0.037) observed in DI in adolescents in the intervention group was significantly higher compared to the control group (Table 2). The Pearson coefficient of correlation in the intervention group showed that the Δ-decrease in mean WC was significantly correlated with Δ-decrease in insulin resistance (as assessed by HOMA-IR) (r = 0.267, P < 0.05) (Fig. 1A) as well as a Δ-decrease in mean TSF thickness (r = 0.348, p < 0.01) (Fig. 1B).
Pearson's coefficient of correlation between:
Values are presented as mean ± standard deviation (SD).
BMI, body mass index; WC, waist circumference; TSF, triceps skinfold; FBG, fasting blood glucose; hs-CRP, high-sensitivity C-reactive protein; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-βCF, homeostasis model assessment of β-cell function.
Values are presented as mean ± standard deviation (SD).
BMI, body mass index; WC, waist circumference; TSF, triceps skinfold; FBG, fasting blood glucose; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-βCF, homeostasis model assessment of β-cell function.
Discussion
This is the first study to evaluate the impact of school-based nutrition education and lifestyle interventions carried out over 6 months on measures of insulin resistance and subclinical inflammation on a sample of Asian Indian adolescents. We observed a significantly higher mean value of HOMA-βCF and significantly lower mean value of hs-CRP, a marker of subclinical inflammation, in the intervention group compared to the control group at 6 months of follow-up. Improvements in knowledge, attitude, practices, anthropometric measurements, and other biochemical parameters have been published previously. 13
We did not observe any significant difference in insulin resistance between the two groups, which may have been due to the short duration of intervention. However, a significantly higher HOMA-βCF value (P = 0.037) was observed at 6 months of follow-up in the intervention group compared to the control group. This finding is important because low HOMA-βCF has been associated with increased prevalence of impaired glucose tolerance (IGT) and T2DM. 23,24 The DI, which was significantly increased (30.3 ± 73.4, P < 0.037) in the intervention group has been shown to be predictive of development of diabetes over a 10-year period in non-diabetic individuals. 25 Waist circumference, a surrogate marker of abdominal adiposity, has also been associated with insulin resistance and predicts the presence of cardiovascular risk factors in children and adolescents, 2,9 independently of BMI. 26 We showed a significant decrease in WC after intervention and a significant positive association (r = 0.267; p < 0.05) between decrease in WC and decrease in insulin resistance (HOMA-IR).
Our study observed a significant decrease in subclinical inflammation in the intervention group compared to the control group. This finding is important because subclinical inflammation in childhood has been shown to be positively associated with abdominal obesity, 27 heart rate, systolic blood pressure, and plasma fibrinogen levels and negatively associated with high-density lipoprotein cholesterol (HDL-C) levels 28 and physical fitness. 29 Furthermore, low flow-mediated dilatation of brachial artery (marker for dysfunctional endothelium) and greater carotid intima media thickness (a marker for atherosclerosis) were seen in children with high hs-CRP levels. 30 Thus, high levels of hs-CRP during childhood may predict early-onset atherosclerosis. 31 This is particularly important for Asian Indians, because we have previously shown that 13% overall and nearly 25% of overweight and obese urban Asian Indian adolescents have high levels of hs-CRP. 6 We have also reported that raised hs-CRP levels in adolescent Asian Indians correlate to diet high (>7% energy) in saturated dietary fat. 32 Importantly, appropriate diet and physical activity may ameliorate insulin resistance and subclinical inflammation. In the current study, an improvement in health-related knowledge of the adolescents in the intervention group may have enabled them to adopt healthy dietary behavior, particularly decreased consumption of energy-dense and high saturated fat junk food and increased physical activity. 13 This may have further resulted in reduced abdominal obesity and a consequent decrease in subclinical inflammation in them.
Table 3 summarizes school-based interventions that were carried out to assess the impact of nutrition and lifestyle interventions on insulin resistance and subclinical inflammation in other countries and ethnic groups. Except for one study, 33 all of the previous studies have been conducted in developed countries (United States and Korea). 34 –39 The effects of a school-based intervention on HOMA-βCF and DI have not been previously reported. In addition, unlike other previous studies, 33,34,38 our interventions not only focused on the “obese and at-risk” group but also included normal-weight adolescents displaying normal glucose homeostasis. Our strategy not only avoided stigmatization of overweight and obese adolescents but also proved that our interventions were beneficial to all adolescents, regardless of their obesity and metabolic status. Significantly, the number of subjects in the experimental (n = 56) and control groups (n = 50) in the present study were higher than most of the previously reported studies. Moreover, two intervention studies 36,37 did not have a control group that would not have eliminated the effects of confounding variables. One of the studies found that there was no significant difference in benefits obtained between subjects participating only in the classroom intervention versus both the classroom and exercise interventions. 35
Arrow pointed downward, decrease; arrow pointed upwards, increase.
Refer to text for details.
hs-CRP, high sensitivity C-reactive protein; IL-6, interleukin 6; BF%, percentage of body fat; DI, disposition index; TC, total cholesterol; BMI, body mass index; TNF, tumor necrosis factor; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TSF, triceps skinfold; FBG, fasting blood glucose; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-βCF, homeostasis model assessment of β-cell function.
Our intervention particularly employed easy-to-use props, such as focused group discussions and lectures, as opposed to print media and audio-visual aids. Additionally, involvement of parents and teachers during the interventions, modification of the canteen menu to healthier alternatives, and training of student volunteers for dissemination of nutrition education to the peers and juniors helped in making the nutrition and lifestyle education program sustainable in the school setting. The intervention emphasized that trained health professionals together with the involvement of teachers and parents can play a major role making an intervention successful. Previously, we have reported that our interventions did not lead to any undesirable effects such as eating disorders or unphysiological weight loss. 13 Finally, we showed that our multi-component intervention model led to positive behavioral, anthropometric, and metabolic changes in the adolescents during a relatively short span of 6 months. The limitations of the study included a substantial drop-out rate for biochemical data at follow-up in both groups.
In conclusion, we report that culturally specific, intensive, repetitive, school-based nutrition education interventions can ameliorate obesity, associated insulin resistance, and subclinical inflammation in adolescents over a period of 6 months. Because there is substantial evidence now that obesity and insulin resistance in childhood cause early-onset T2DM and CHD, 40 our intervention model could be useful for prevention of obesity, the metabolic syndrome, and T2DM in risk-prone adolescents.
Footnotes
Acknowledgments
This study was fully supported by grant from World Diabetes Foundation, Denmark (WDF05-120). We are thankful to the children for their cooperation in the study and to the principals, teachers (Rema Alex Daniel, Ms. Sheela Rao, Ms. Mini Khanna), and the staff of the schools for their extended help.
Author Disclosure Statement
The authors have no conflicts of interest to report.