
Abstract
Background:
The aim of this study was to compare the prevalence of metabolic syndrome in human immunodeficiency virus (HIV)–infected patients treated with highly active antiretroviral therapy (HAART), using the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), European Group for the Study of Insulin Resistance (EGIR), and International Diabetes Federation (IDF) definitions.
Methods:
A cross-sectional study was carried out with 159 consecutive adult HIV-infected subjects (120 males and 39 females) under HAART. Anthropometric and laboratory parameters were measured by standard methods. Hyperinsulinemia was defined by a fasting concentration >75th percentile of values obtained in healthy individuals (107.5 pmol/L).
Results:
The prevalence of ATP III-defined metabolic syndrome was 10.1%; it was 28.3% according to EGIR criteria and 15.1% using the IDF definition. The concordance between the definitions was low (kappa coefficient ranging between 0.134 and 0.296). All subjects with EGIR-defined metabolic syndrome had hyperinsulinemia, but only 50% of those with ATP III-defined metabolic syndrome and 62.5% in the IDF metabolic syndrome population had hyperinsulinemia.
Conclusions:
The inclusion of hyperinsulinemia as a criterion in the EGIR metabolic syndrome definition made it more discriminative than the ATP III definition, both in men and women, and than the IDF definition in men to identify metabolic syndrome in HIV-infected subjects under HAART.
Introduction
The aim of the present study was: (1) To determine the prevalence of metabolic syndrome in HIV-1-infected patients treated with antiretroviral therapy by using the criteria from the NCEP ATP III guidelines, 20 the European Group for the Study of Insulin Resistance (EGIR), 21 and International Diabetes Federation (IDF) 22 definitions and (2) to compare the populations identified by these definitions.
Materials and Methods
Study subjects
A total of 159 consecutive adult HIV-infected patients participated in this cross-sectional study. All patients had biologically documented HIV-1 infection, were receiving their first antiretroviral regimen, and were under active follow-up. Patients were excluded if they had kidney or liver disease or if they used concomitant therapy with anabolic hormones or systemic glucocorticoids, recombinant human growth hormone, appetite stimulants, or hypolipidemic agents. The study protocol was approved by the Hospital Ethics Committee, and all patients gave their informed consent.
Anthropometric measurements
The patients wore light indoor clothes and no shoes when the anthropometric measurements were taken. Weight, height, and waist and hip circumferences were measured by standard methods. 23 Body mass index (BMI) was calculated as weight/height 2 (kg/m2). Lipodystrophy was defined by the presence of lipoatrophy, lipohypertrophy, or mixed syndrome, as previously described. 23
Laboratory methods
All laboratory investigations were performed after fasting for 12 h. Total cholesterol and triglycerides were measured using enzymatic standard method and high-density lipoprotein cholesterol (HDL-C) by a direct method (Roche Diagnostics, Basel, Switzerland). We calculated low-density lipoprotein cholesterol (LDL-C) by the Friedewald formula when triglyceride did not exceed 3.45 mmol/L (300 mg/dL), and otherwise by ultracentrifugation. Serum glucose concentration was measured using an enzymatic reaction (Hitachi Modular D2400; Roche, Basel, Switzerland). Serum insulin concentration was measured by an automated solid-phase, two-site chemiluminiscent immunometric assay (Immulite 2000®, Diagnostic Products Corp., Los Angeles, CA), with a 8% cross-reactivity with proinsulin and a total analytical imprecision less than 7.5% for values between 55 and 2100 pmol/L (7.7 and 291 μIU/mL). CD4 cell count (×106/L) and quantitative HIV-1 RNA (viral load, log10 copies/mL) were measured in venous blood. Plasma HIV-1 RNA concentrations were determined with the Roche Amplicor HIV-1 Monitor assay, which has a lowest limit of detection of 200 copies/mL. 24 Results below the assay limit of detection were assigned a value of 2.3 log10.
Definition of metabolic syndrome
Metabolic syndrome was defined using the criteria proposed by the NCEP ATP III, 20 EGIR, 21 and IDF. 22 According to NCEP ATP III, metablic syndrome was defined as the presence of three or more of the following criteria: Abdominal obesity (waist circumference >102 cm in men or >88 cm in women), triglycerides ≥150 mg/dL (1.69 mmol/L), HDL-C <40 mg/dL (1.04 mmol/L) in men or <50 mg/dL (1.30 mmol/L) in women, high blood pressure >130/85 mmHg, and fasting glucose ≥110 mg/dL (≥6.1 mmol/L).
Under the EGIR criteria, metabolic syndrome was defined by the presence of fasting serum insulin concentration above the 75th percentile of values obtained by our assay method in healthy individuals (107.5 pmol/L) and two or more of the following criteria: Abdominal obesity (waist circumference ≥94 cm in men and ≥80 cm in women, and/or BMI >30 kg/m2), triglycerides >180 mg/dL (>2.0 mmol/L), or HDL-C concentration <40 mg/dL (<1.0 mmol/L), blood pressure >140/90 mmHg or being under antihypertensive treatment, and fasting glucose ≥110 mg/dL (≥6.1 mmol/L).
The IDF definition of metabolic syndrome includes central obesity (in our country, waist circumference ≥94 cm in men and ≥80 cm in women, and/or BMI ≥30 kg/m2) plus any two of the following criteria: Triglycerides ≥150 mg/dL (≥1.7 mmol/L) or specific treatment for this lipid abnormality, HDL-C <40 mg/dL (<1.04 mmol/L) in males or <50 mg/dL (<1.30 mmol/L) in females, blood pressure ≥130/85 mmHg or being under antihypertensive treatment, and fasting plasma glucose ≥100 mg/dL (≥5.6 mmol/L) or previously diagnosed type 2 diabetes.
Statistical analysis
Statistical analysis was performed using the SPSS 10.0 program for MSWindows. The continuous variables were expressed as a mean and standard deviation and the categorical variables as frequencies. Continuous variables were compared, using the Student t-test for paired data (Gaussian distribution) or Mann–Whitney test (non-Gaussian distribution), and categorical variables, using the chi-squared test. The kappa coeficient was used to evaluate the homogeneity between two populations of patients with metabolic syndrome defined according to the NCEP ATP III criteria, the EGIR criteria, or the IDF definition. Populations having metabolic syndrome according to the three definitions were compared globally using an analysis of variance (ANOVA) analysis and also one type to any other type using T test or no parametric tests. A p value <0.05 (two-tailed) was considered to be significant.
Results
The clinical and metabolic characteristics of the study population are presented in Table 1. Thirty three percent of subjects were overweight or obese (BMI ≥25 kg/m2) and 6.9% had abdominal obesity (waist circumference >102 cm in men or >88 cm in women). The prevalence of diabetes or impaired fasting glucose was 11.3%, and 39.6% had insulin levels above the 75th percentile of nondiabetic subjects, 3.8% had blood pressure ≥130/85 mmHg or were currently on antihypertensive therapy, and 74.8% were dyslipidemic [LDL-C ≥160 mg/dL (4.13 mmol/L) and/or tryglicerides ≥150 mg/dL (1.69 mmol/L) and/or HDL-C cholesterol <40 mg/dL (1.04 mmol/L) in men or <50 mg/dL (1.30 mmol/L) in women].
Abdominal obesity (waist circumference >102 cm in men or >88 cm in women).
Hyperinsulinemia (concentrations above 75thpercentile of nondiabetic subjects).
Hypertension (blood pressure ≥130/85 mmHg or under antihypertensive therapy).
Dyslipidemia (LDL-C ≥4.13 mmol/L and/or tryglicerides ≥1.69mmol/L and/or HDL-C <1.04 mmol/L (men) or <1.3 mmol/L (women).
HIV-1, human immunodeficiency virus type 1; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
The prevalence of metabolic syndrome using NCEP ATP III criteria was 10.06% and according to the ATP III revised criteria 25 16.9%, whereas that using the EGIR criteria was 28.30% and 15.1% according to IDF metabolic syndrome definition (Table 2). The syndrome was more common in males than women with ATP III (10.83% vs. 7.69 %) and EGIR (30% vs. 23.07%), but not with the IDF (10% vs. 30.8%) definition.
ATP III, Adult Treatment Panel III; EGIR, European Group for the Study of Insulin Resistance; IDF, International Diabetes Federation; HIV, human immunodeficiency virus; BMI, body mass index; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Patients with ATP III-defined metabolic syndrome, but not EGIR-defined nor IDF-defined metabolic syndrome, were older (45.3 vs. 38 years, p=0.014) than those without metabolic syndrome. Overall, there were no significative differences in the variables related with the HIV infection (time of HIV infection, CD4 cell count, viral load, mean time antiretroviral therapy with protease inhibitors) between patients with and without metabolic syndrome.
The characteristics of the individuals classified as metabolic syndrome according to ATP III, EGIR, and IDF definitions are shown in the Table 2. There were significative differences in the glucose-to-insulin ratio, which was higher in patients with ATP III-defined metabolic syndrome (0.044±0.023) and IDF-defined metabolic syndrome (0.040±0.024) than in EGIR-defined metabolic syndrome (0.0274±0.013). No other differences in demographic, HIV-infection related, and analytical variables were found between HIV-infected subjects with metabolic syndrome defined according ATP III, EGIR, and IDF guidelines.
The prevalence of the individual components of metabolic syndrome according to ATP III, EGIR, and IDF criteria are displayed in Fig. 1. As expected, hyperinsulinemia was the most common component in EGIR-defined metabolic syndrome, whereas it was present in only 50% of patients with ATP III-defined metabolic syndrome and in 62.5% of IDF-defined metabolic syndrome. The other components were generally more common in ATP III-defined metabolic syndrome, except for the abdominal obesity, whose essential role in the IDF metabolic syndrome definition made it more frequent in this group.
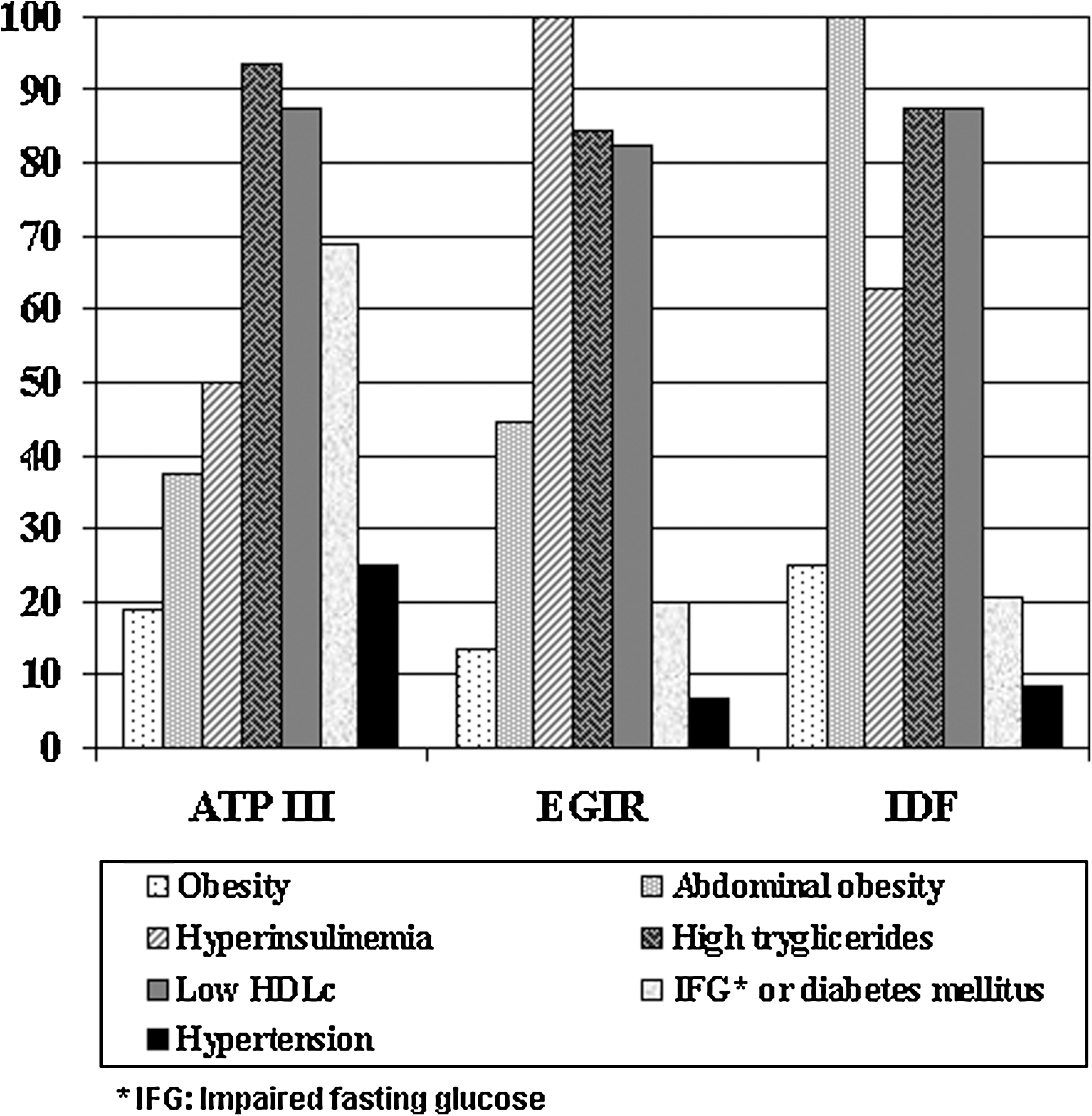
Prevalence of the individual components of the metabolic syndrome according to Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), the European Group for the Study of Insulin Resistance (EGIR), and the International Diabetes Federation (IDF) definitions.
Concordance between the definitions of metabolic syndrome was low (kappa coeficient: 0.261 (IDF vs. ATP III), 0.296 (IDF vs. EGIR), and 0.134 (ATP III vs. EGIR). Among subjects meeting ATP III criteria, they also met simultaneously the EGIR or the IDF criteria in 50% and 44% of the cases, respectively. The ATP III metabolic syndrome definition selected 29% of the subjects with metabolic syndrome according the IDF criteria while 62% were identified if the EGIR metabolic syndrome definition was applied. Patients with EGIR-defined metabolic syndrome were identified as also having the syndrome according to ATP III or IDF criteria in 18% and 33% of the cases, respectively.
Finally, when we considered the subgroup of patients with lypodystrophy, 12.7% of subjects had metabolic syndrome using ATP III criteria, 39.4% according to EGIR criteria, and 22.5% according to IDF definition. Only 4.22% of the subjects with lypodystrophy were classified as having metabolic syndrome for the three definitions. Among the subjects with lypodystrophy, 8.45% of them were classified as having metabolic syndrome under both the ATP III and IDF criteria, 16.90% under the EGIR and IDF criteria, and 7.04% under the ATP III and EGIR criteria simultaneously.
Discussion
In the present study we demostrate that, in HIV-1-infected subjects under HAART, the prevalence of the metabolic syndrome is widely influenced by the selection of the diagnostic criteria. Lack of criteria for insulin resistance hyperinsulinemia in the ATP III and the IDF guidelines definitions may be an explanation for the identification of a lower number of cases of metabolic syndrome using these criteria with respect to the EGIR definition. Moreover, the lower prevalence of abdominal obesity in the ATP III definition may also contribute to explaining the differences in the metabolic syndrome prevalence with respect to the EGIR and IDF metabolic syndrome subgroups. Therefore, metabolic syndrome definitions that consider insulin resistance may be more useful for detecting metabolic syndrome in HIV-infected subjects.
The metabolic syndrome represents a constellation of metabolic risk factors for cardiovascular disease and type 2 diabetes, 26 –30 and major underlying risk factors for this syndrome are obesity and insulin resistance. 31 –35 The contribution of these underlying factors and the prevalence of metabolic syndrome vary among different populations and criteria used for clinical diagnosis of metabolic syndrome. 18,27,36 –38,39 In HIV-infected subjects, information about the prevalence of metabolic syndrome using different criteria is very limited, 9 –15,40,41 and there are no available data comparing metabolic syndrome definitions requiring versus not requiring insulin measurements.
As far as we know, our study provides the first comparison of prevalences of metabolic syndrome in and HIV-infected population using more than two different definitions and comparing definitions requiring and not requiring insulin measurement. The prevalence of metabolic syndrome was higher than that reported in the general Spanish population using the EGIR and ATP III revised definitions, but lower with IDF and ATP III criteria. 42 –46 The prevalence of metabolic syndrome with the EGIR criteria is similar to the one reported by Gazzaruso et al. in an HIV-infected population, 12 but higher than the reported prevalence in the Spanish general population using the same criteria. 42 Only 10% of the patients had metabolic syndrome using ATP III criteria, which is very similar to that reported in HIV-infected subjects in Spain but lower than that reported in other HIV-infected populations with similar age and gender distribution. 9 –11,13,14,47 The few data available in HIV-infected subjects using the IDF definition show similar results to the observed in our study. 13,48,49 Finally, the use of a lower cut-off point for glycemia in the ATP III revised criteria 25 increased the prevalence of metabolic syndrome, being similar to that observed with IDF definition but lower than that obtained with EGIR criteria.
There is debate about the relative importance of both insulin resistance and obesity as the major underlying cause of the metabolic syndrome, but the contribution in the pathophysiology and prevalence of other components of metabolic syndrome may vary among different populations. 50,51 In this context, there is growing evidence that supports the central role of insulin resistance as the underlying and primary disorder of metabolic alterations in the HIV-infected subjects under HAART. 52 –54 In addition, BMI is often normal and insulin resistance precedes lipodystrophy. 55 In the present study, only 50% and 62.5% of the subjects satisfying ATP III and IDF criteria, respectively, had hyperinsulinemia, and most of the insulin-resistant individuals did not satisfy the ATP III (87.3%) or the IDF (76.2%) criteria. These results are in agreement with studies suggesting that using glucose clamp techniques demonstrates that metabolic syndrome defined by ATP III guidelines did not identify subjects with insulin resistance. 16,56,57 Finally, the lower thresholds of abdominal obesity in the EGIR and IDF syndrome definitions result in a higher frequency of central obesity with these criteria. Because the major differences between metabolic syndrome definitions relate to the differences in the thresholds of abdominal obesity and the inclusion of hyperinsulinemia as a diagnostic feature in EGIR criteria definition, differences in prevalence and identification of subjects with metabolic syndrome in our study are not surprising.
Although the long-term effects on cardiovascular disease have not been yet determined, there is a growing concern about an increased risk for cardiovascular disease in HIV-1-infected patients receiving combination antiretroviral therapy and this risk could be related to metabolic abnormalities associated with long-term use of antiretroviral drugs. 58 –63 In this context, hyperinsulinemia and atherogenic dyslipidemia are the most prevalent alterations in HIV-infected subjects, and subjects with hyperinsulinemia and dyslipidemia are at increased risk for cardiovascular disease. 50,56,64 –66 Moreover, some studies reported higher cardiovascular risk in subjects with metabolic syndrome defined with EGIR criteria with respect to IDF and ATP III criteria, 67 although prospective studies are needed to confirm it in an HIV-infected population. If these data are confirmed, metabolic syndorme defined by EGIR criteria may be a more useful definition to identify HIV-infected subjects with a particularly high cardiovascular risk.
Footnotes
Acknowledgment
This study was funded by the grant FIS PI 05/2099.
Author Disclosure Statement
All authors declare having no competing financial interests.