
Abstract
Background:
We conducted a systematic review of randomized controlled trials (RCTs) that evaluated the effectiveness of insulin regimens with insulin analogs to reach the glycosylated hemoglobin (HbA1c) target of <7% in patients with type 2 diabetes.
Methods:
RCTs involving insulin regimens (basal, prandial, biphasic, and basal-bolus) with insulin analogs in type 2 diabetes were identified through electronic searches [MEDLINE, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and The Cochrane Library] through September, 2010. We included any study arm of RCTs if they were at least 12 weeks in duration and reported HbA1c as an outcome.
Results:
We identified 55 RCTs, with 96 arms and 33,244 patients, that reported the HbA1c target, and 32 RCTs, with 32 arms and 5,559 patients, that did not report the target. The missing targets were calculated with an algorithm that explained 88% of variability between studies. Overall, the proportion of patients at target (HbA1c <7%) was 37.2% [95% confidence interval (CI), 31.5–43.1%] with basal insulin, 35.3% (28.9–42.1%) with biphasic insulin, 37.5% (27.7–47.9%) with prandial insulin, and 51.2% (41.4–61.1%) for basal-bolus insulin, with high heterogeneity (I2 >80% for all).
Conclusions:
The HbA1c target <7% can be achieved in a proportion of patients ranging from 35% to 51%, depending on the particular insulin regimen. At least one half of patients with type 2 diabetes receiving insulin analogs do not reach the HbA1c target.
Introduction
Methods
We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist for reporting systematic reviews and meta-analyses. 5
Data sources and searches
We updated our previous systematic review and continued the search through September, 2010. Reports of RCTs of insulin analogs in type 2 diabetes patients were identified through systematic literature search of MEDLINE, EMBASE, The Cochrane Library, and Cumulative Index to Nursing and Allied Health Literature (CINAHL). The main search terms were type 2 diabetes, hemoglobin A1c, long-acting insulin analogs, short-acting insulin analogs, biphasic insulin analogs, glargine, detemir, neutral protamine lispro, lispro, aspart, glulisine, randomized controlled trials, and clinical trials. We also reviewed reference lists of included articles, the U.S. Food and Drug Administration and European Medicines Agency websites for the insulin analogs, and websites of public registries of clinical trials (
Study selection
For a study to be included in the systematic review, it had to be (1) a RCT that evaluated different insulin regimens (basal, biphasic, prandial, or basal-bolus) with insulin analogs in type 2 diabetes and (2) reported HbA1c as an outcome measure. Because being a RCT was a prerequisite for inclusion, any other arm of a given RCT that assessed human insulin or oral drugs was excluded. So, many RCTs could only have one arm. We included crossover trials with at least 12 weeks of follow-up before and after the crossover phase. The search had no language restriction; we excluded reviews, editorials, comments, letters, and abstracts. Trials were rejected if the intervention time was <3 months or the number of patients in any arm was less than 30 patients.
Data extraction and quality assessments
Titles, abstracts, and articles were reviewed independently by two authors (D.G. and K.E.), and any disagreements were resolved by consensus. Methodological quality was scored using criteria set out by Jadad et al. 6 This 5-point quality scale included points for randomization (described as randomized, 1 point; table of random numbers or computer-generated randomization, additional 1 point), double-blind (described as double-blind, 1 point; use of masking such as identical placebo, additional 1 point), and follow-up (the numbers and reasons for withdrawal in each group are stated; 1 point) in the report of an RCT. We gave an additional point if the analysis was by intention-to-treat. We considered scores of 2 or less as low quality, and a score of 3 or more as high quality, because none but one of the studies were double-blinded, which is difficult with this type of intervention.
Insulin regimens
We evaluated four insulin regimens: (1) Basal insulin consisted of long-acting insulin analogs (glargine, detemir, and lispro NPL); (2) biphasic insulin consisted of premixed insulin analogs (lispro 25/75, lispro 50/50, aspart 30/70, aspart 50/50, aspart 70/30, with the numbers denoting the percentage of the rapid-acting to the long-acting component, respectively); (3) prandial insulin consisted of short-acting insulin analogs (lispro, aspart, glulisine); and (4) basal-bolus insulin consisted of any combination of prandial and basal insulin analogs. Humalog NPL is not available in the United States at present.
Data synthesis and analyses
The proportion of patients with HbA1c <7% at the end of treatment was the primary outcome. Statistically, binomial proportion lacks consensus over the calculation of the confidence intervals. We transformed the proportions into a quantity suitable for the usual fixed and random effects summaries (the Freeman–Tukey variant of the arcsine square root transformed proportion). 7 The pooled proportion is calculated as back-transformation of the weighted mean of the transformed proportions, using inverse arcsine variance weights for the fixed effects model and DerSimonian–Laird weights 8 for the random effects model. We used the calculated proportions for descriptive purposes, because claim for superiority can be drawn from meta-analysis of comparative trials. Meta-regression models to check for prognostic factors of response, were fitted by using the SAS proc Mixed procedure.
In 32 trials (39 arms and 5,559 patients) that qualified for inclusion/exclusion criteria, the proportion of patients with HbA1c <7% at the end of treatment was not reported. We used the available information from the 55 trials (96 arms and 33,244 patients) that reported the proportion of patients with HbA1c <7% for developing an algorithm for the estimate of the proportion of patients with HbA1c <7% (p) starting from the mean value of HbA1c reported at the end of treatment. The algorithm was a linear regression model relating the logit of the success rate [log(p/(1−p)], with the HbA1c at the end of the treatment. Following there is the resulting equation to predict the logit of the success rate: log(p/1−p)=11.68167−164.3119×HbA1c−end. This equation explained the 88% of the variability between studies, and just little deviance between observed and predicted success rates were reported. The proportion of patients at target (p) was then given by simple mathematical transformations.
Heterogeneity of the effect across studies was assessed by the Q 2 statistics, which is distributed as a chi-squared statistic. A p value <0.10 was used to indicate lack of homogeneity among effects. I 2 statistics were also provided to quantify the percentage of total variation across studies that were attributable to heterogeneity rather than to chance. 9 A value greater than 50% represented substantial heterogeneity.
Results
The process of selecting the RCTs utilized in the final analyses from the 2,700 citations originally identified is described in Fig. 1. We found 87 studies (refs. 10 –96), with a total of 135 arms, that satisfied the inclusion/exclusion criteria. Most trials were multinational and sponsored by industry. Publication years ranged from 1997 to 2010. All studies were randomized controlled trials (Table 1): Among these, most were parallel group and 8 were crossover studies. All studies were of open-label design except one. Trial duration ranged from 12 to 134 weeks. The trials enrolled a total of 38,803 patients (range, 41 to 2,493 patients per arm); baseline HbA1c ranged from 7.2% to 10.6%. Scores of methodological quality ranged from 1 to 6 (median score 3).
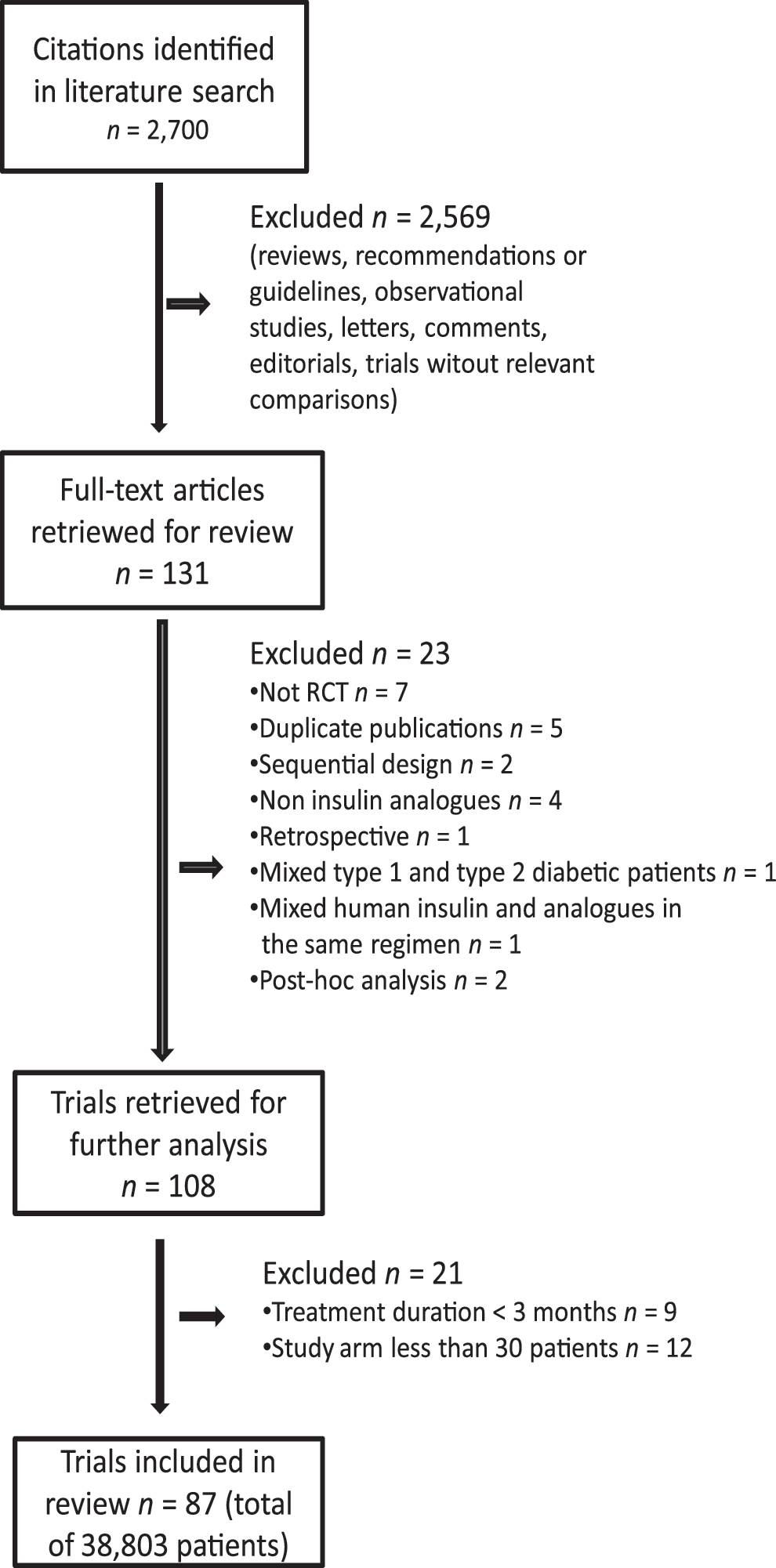
Process of selecting the randomized controlled trials (RCTs) used in the final analyses from the 2,700 citations originally identified. RCT, randomized controlled trial.
OADs, oral antidiabetic drugs; HbA1c, glycosylated hemoglobin; R, randomized; O, open; DB, double-blind; P, parallel; CO, cross-over; Met, metformin; Su, sulfonylurea; Tzd, thiazolidinedione; Pio, pioglitazone; Glimep, glimepiride; α-g, α-glucosidase inhibitor; Big, biguanide.
All results are given in Table 2; they are presented for the four insulin regimens (basal, biphasic, prandial, and basal-bolus) and divided for reported targets (arms in which the proportion of patients with HbA1c <7% was reported), calculated target (arms in which the proportion of patients with HbA1c <7% was not reported but calculated with the algorithm), and pooled data (both reported and calculated). There were 45, 26, 9, and 13 arms that reported the proportion of patients at target with basal, biphasic, prandial, and basal-bolus insulin, respectively. The proportion of patients with HbA1c <7% was 42.5%, 46.5%, 39.6%, and 52.2%, respectively. Heterogeneity was high for all regimens (I 2 >50%).
The I2 parameter represents the percentage of total variation across studies that is attributable to heterogeneity rather than chance. P value refers to the difference of post-treatment (final) HbA1c values between published and estimated target.
HbA1c, glycosylated hemoglobin; CI, confidence interval.
Additional 37 arms (12, 20, 4, and 3, for basal, biphasic, prandial and basal-bolus insulin, respectively) with a total of 5,426 patients did not report the target. The overall proportion of patients at target for both basal and biphasic regimens was 30% and 53% less in comparison with the pooled estimate provided by the analysis of reported target; on the other hand, there were smaller differences for the prandial and basal-bolus regimens between reported and calculated targets. The median of final HbA1c level was higher for the basal and the biphasic insulin regimens in the arms with calculated target as compared with the arms with reported target. There was no difference in terms of variability attributable to heterogeneity across studies.
The proportion of patients at target in the pooled data (both reported and calculated) was closer to that observed in arms with reported target than that in arms with calculated target, owing to the greater number of arms (and patients) that reported the target.
Discussion
Insulin analogs are modified human insulins developed to address the limitations of human insulin preparations. 2 Conversion of the insulin market to analogs, estimated to be 40%–45% in 2005, was projected to reach saturation within 2010. 97 On the basis of the present analysis extended to 135 arms with 38,803 patients, we found that insulin analogs currently adopted in the clinical management of type 2 diabetes resulted in different proportions of patients achieving the recommended HbA1c target of <7%. The proportion of patients at target within the four insulin regimens derived by the arms with reported target ranged from the least value of 39.6% with the prandial to the highest value of 52.2% with the basal-bolus regimen. These figures were quite similar to those reported in the previous analysis, 4 which makes it unlikely that further future studies will change them consistently. On the other hand, the proportions changed substantially, at least for basal and biphasic insulin regimens, by taking into account the studies that did not report the target. For the basal and biphasic insulin regimens, the calculated targets were between 30% and 50% lower than the reported targets. Because the algorithm we developed used the final HbA1c for calculating the target, this difference could be almost entirely explained by the higher posttreatment HbA1c values observed in the 39 arms. The mean difference between final HbA1c level ranged from 0.29% for the prandial to 0.8% for the biphasic regimen; this fully explained the differences in the proportion of patients at target between calculated and reported targets.
Selective outcome reporting occurs too often in medical studies, perhaps as a consequence of the situation that negative or less-than expected results are less likely to be published or reported than positive or fully expected results: Meta-analyses based on these studies are subject to some degree of publication bias because they may be drawing conclusions on less than all of the data. 98 This might have occurred in trials selected for the present analysis. Taking into consideration the biphasic regimen, for example, only 21% (on the average) of the 1,832 patients included in the 20 arms were at target, a deluding result as compared with the average 46% of patients at target with this regimen in the 29 arms with reported targets. Insulin is the most effective of diabetes medications in lowering glycemia. It can, when used in adequate doses, decrease any level of elevated HbA1C to, or close to, the therapeutic goal. Unlike the other blood glucose-lowering medications, there is no maximum dose of insulin beyond which a therapeutic effect will not occur. 99 We have no plausible explanation for the difference between reported and calculated target with basal or biphasic insulin regimens. Some study characteristics, including year of publication, quality score, starting HbA1c, insulin titration, and concomitant use of oral drugs, did not explain the difference, which seems inherent to the protocol of the particular study.
This study has limitations. The methodological quality of the trials ranged from low to high, and the degree of heterogeneity was high. In most cases, results were qualitatively similar across studies in terms of directions of effect, even in the presence of large I 2 values. Most trials had a short follow-up and firm conclusions cannot be drawn about the long-term comparative effectiveness of the various regimens, although trials with longer follow-up are present in the analysis. On the other hand, intermediate outcomes, such as HbA1c, are commonly used clinically to optimize glycemic control. Moreover, the different methods of HbA1c assay used in the various studies may introduce some confounding, although this may apply to similar analyses. Finally, this analysis focused on a HbA1c target of <7%; however, specific diabetic populations or specific situations may require targets more or less stringent. Therefore, targets from 6.5% to 8% may be suggested depending on, although not limited to age, life expectancy, co-morbid conditions, patient preferences, and medication adverse effects. 100,101 At the very end, the higher cost of insulin analogs, as compared with human insulins, may be a deterrent in some “real-world” situations. This study has also strengths. To our knowledge, it represents the first comprehensive analysis describing the attainment of the currently recommended HbA1c target of <7% in type 2 diabetes using insulin analogs for optimization of glycemic control; moreover, the high number of RCTs included (87 RCTs with 135 arms) and the huge number of patients investigated (38,803) makes unlikely the possibility that even missed (nonpublished) data may alter the proportion herein reported.
Our analysis of 38,803 type 2 diabetic patients using insulin analogs in type 2 diabetes indicates that the HbA1c target of <7% can be achieved in a proportion of patients ranging from 35% to 51%, depending on the particular insulin regimen. This poses the problem of how to manage the half of patients that are not at the HbA1c goal with the best, and ultimate, insulin regimen now available (basal-bolus) for controlling hyperglycemia in the real world of the diabetic patient.
Footnotes
Author Disclosure Statement
No conflict of interest exists for any of the authors.