
Abstract
Background:
In metabolic syndrome, hypertension has been noted as one of the most important risk factors that contributes to cardiovascular disease. We have evaluated the effect of a selective adrenergic β1-receptor blocker, atenolol, on blood pressure and pulse rate in metabolic syndrome.
Methods:
Metabolic syndrome patients with hypertension (n=28) and a control group (n=20) were given atenolol (50 mg/day) for 4 weeks. Blood pressure, pulse rate, and blood biochemical parameters were monitored.
Results:
Pulse rate in the metabolic syndrome group before the treatment was significantly higher than in the control group (control 74±2/min, metabolic syndrome 84±2/min, P<0.05). Decrease in pulse rate resulting from the treatment was greater in the metabolic syndrome group than in the control group (control 14±3/min, metabolic syndrome 21±2/min, P<0.05). Decrease in systolic (SBP) and diastolic (DBP) blood pressure was greater in the metabolic syndrome group than in the control group (SBP, control 8±3, metabolic syndrome 23±3 mmHg, P<0.05; DBP, control 6±3, metabolic syndrome 13±2 mmHg, P<0.05). There was a positive association between decrease in SBP and the waist measurements of patients, between the decrease in DBP and the waist measurements, and between the decrease in pulse rate and the waist measurements. We also found that there was a positive association between the decrease in SBP and initial SBP, between the decrease in DBP and initial DBP, and between the decrease in pulse rate and initial pulse rate.
Conclusions:
These data showed that atenolol has an enhanced effect on blood pressure and on pulse rate in metabolic syndrome. It may be useful in treating severe hypertension with elevated heart rate in metabolic syndrome.
Introduction
Insulin resistance plays a key role in metabolic syndrome, and this underlies increasing blood pressure in obese and metabolic syndrome patients. 4 Moreover, hyperinsulinemia stimulates the sympathetic nervous system and results in elevating blood pressure and heart rate. 5 Insulin increases sodium reabsorption in the kidneys and activates the renin–angiotensin system; therefore, blood pressure is elevated with an increase in circulating volume and cardiac output. 6 In response to positive energy balance, sympathetic activity is stimulated in obese and in metabolic syndrome patients in the presence of insulin resistance, 7 resulting in the elevation of blood pressure with constriction of peripheral blood vessels and also in the elevation of heart rate. 8
There is increased leptin secretion in the white fat cells, and a positive relationship between blood leptin levels and fat accumulation is observed. 9 Along with insulin resistance, leptin resistance also contributes to hypertension, increasing sympathetic activity. 10 These factors may elevate heart rates in obese or metabolic syndrome. It has been reported that some β-receptor blockers decrease circulating leptin levels. 11,12
β-Receptor blockers have been reported to be effective in treating hypertension with diabetes, because blood pressure reduction due to the administration of captopril or atenolol was similarly effective in reducing the incidence of diabetic complications. 13 However, adrenergic β-receptor blockers are not recommended as the first choice for hypertension patients with diabetes or obesity because these medications can cause metabolic side effects and mask symptoms of hypoglycemia. 14 By using nonselective β-blockers, adverse effects such as abnormalities of glycemic and lipid profiles may occur. 14 Atenolol is a highly selective adrenergic β1-blocker, and its lowering of heat rate is novel compared to other β1-blockers without possessing intrinsic sympathetic activity. 15
Previous studies show that increased heart rate is associated with higher incidence of cardiovascular events and higher mortality, 16 suggesting that not only blood pressure but also heart rate should be taken into account for preventing cardiovascular events. We investigated whether or not atenolol is useful in reducing sympathetic activity and consequently reducing blood pressure and pulse rate in hypertension patients with metabolic syndrome.
Materials and Procedures
Subjects and study design
A total of 28 patients with hypertension, who exhibited metabolic syndrome, and a control group of 20 patients, who had essential hypertension [systolic blood pressure (SBP) ≥130 mmHg or diastolic blood pressure (DBP) ≥85 mmHg] received atenolol (50 mg/day) for 4 weeks. Metabolic syndrome was diagnosed based on new Japanese criteria (CEDSMSL 2005) that include a waist measurement of 85 cm or over with at least two cardiovascular risk factors, among which are high blood pressure (SBP≥130 mmHg or DBP ≥85 mmHg), hyperglycemia (fasting blood glucose ≥110 mg/dL), and dyslipidemia [triglycerides ≥150 mg/dL, or high-density lipoprotein cholesterol (HDL-C)<40 mg/dL]. 17
Patients were advised to maintain the same diet and exercise as before the study. Body weight, height, and waist circumference of patients were measured. Blood pressure and pulse rate were monitored before and after the administration of atenolol. Blood pressure was measured in the morning at the hospital. All of the patients were instructed to sit and rest for at least 10 min before having their blood pressure measured in the sitting position. Blood samples were taken before and at the end of the study, measuring fasting blood glucose, fasting serum insulin, triglycerides, HDL-C, and free fatty acid. All patients gave informed consent to participate in the study, which had been approved by the hospital's ethics committee.
Determination of blood biochemical parameters
Serum glucose was determined by hexokinase method (Flex Cartridge Glucose GLU, Siemens Healthcare Diagnostics, Tokyo, Japan), insulin by a chemiluminescent-immunometric assay (Immulite 2000 Insulin, Siemens Medical Solutions Diagnostics, Los Angeles, CA), triglyceride by the GPO-HDAOS method (L-Type TG-H kit, WAKO Japan Co. Ltd., Osaka, Japan), HDL-C by using standard enzymatic methods (HDL-C kit, Siemens Healthcare Diagnostics, Tokyo, Japan), and free fatty acid by a commercial enzymatic procedure (NEFA-HR kit, ACS-ACOD Method, Wako Pure Chemical Industries, Osaka, Japan).
Statistical analyses
Results were expressed as mean value±standard error (SE). Comparison of blood pressure, pulse rate, and blood parameters before and after the treatment were analyzed by a paired t-test. Decreases in blood pressure and pulse rate in the metabolic syndrome group resulting from the treatment were analyzed by an unpaired t-test. The Pearson correlation coefficient was calculated by linear regression. Multiple linear regression analyses were used to examine association of parameters. Significance was set at P<0.05 for all analyses.
Results
Waist measurement, body mass index (BMI), and body weight in the metabolic syndrome group were significantly greater than in the control group (Table 1). Fasting plasma insulin (IRI) and homeostasis model assessment of insulin resistance (HOMA-IR) before treatment were significantly greater in the metabolic syndrome group than in the control group (Table 2).
P<0.01 vs. control group.
P<0.01 vs. control group.
FBG, fasting blood glucose; FIRI, fasting plasma insulin; HOMA-IR, homeostasis model assessment of insulin resistance; FFA, free fatty acid; HDL-C, high-density lipoprotein cholesterol.
Pulse rate in metabolic syndrome
Before treatment, the pulse rate in the group of metabolic syndrome patients was significantly higher than in the control group (84±2, 74±2/min, P<0.01; Table1), and there was positive association between pulse rate and waist measurement in all of the patients (r=0.475, P<0.002).
Effect of atenolol on blood pressure and pulse rate
Atenolol decreased SBP after 4 weeks in the metabolic syndrome patients and in the control group (161±3 to 139±4 mmHg, P<0.01, 159±3 to 150±4 mmHg, P<0.05; Fig. 1). Decreases in SBP in the metabolic syndrome group were significantly greater than in the control group (23±3, 8±3 mmHg, P<0.01; Fig. 1). Atenolol also decreased DBP after 4 weeks in the metabolic syndrome group and in the control group (96±3 to 83±2 mmHg, P<0.01, 92±4 to 86±3 mmHg, P<0.05, Fig. 2). Decreases in SBP and DBP in the metabolic syndrome group were significantly greater than the control group (13±2, 6±3 mmHg, P<0.001; Fig. 2). There was a positive association between the decrease in SBP and waist measurements (r=0.377, P<0.01), and a positive association between the decrease in DBP and waist measurements of the patients (r=0.373, P<0.02). We also found that there was a positive association between the decrease in SBP and initial SBP (r=0.392, P<0.01), and a positive association between the decrease in DBP and initial DBP (r=0.577, P<0.001). These associations were found in all the patients in this study.

The effect of atenolol on systolic blood pressure (SBP). SBP at week 0 and week 4 and decrease in SBP in each group are shown. (*) P<0.05 vs. the control group by unpaired t-test; (#) P<0.05 vs. week 0 by paired t-test. MS, metabolic syndrome.
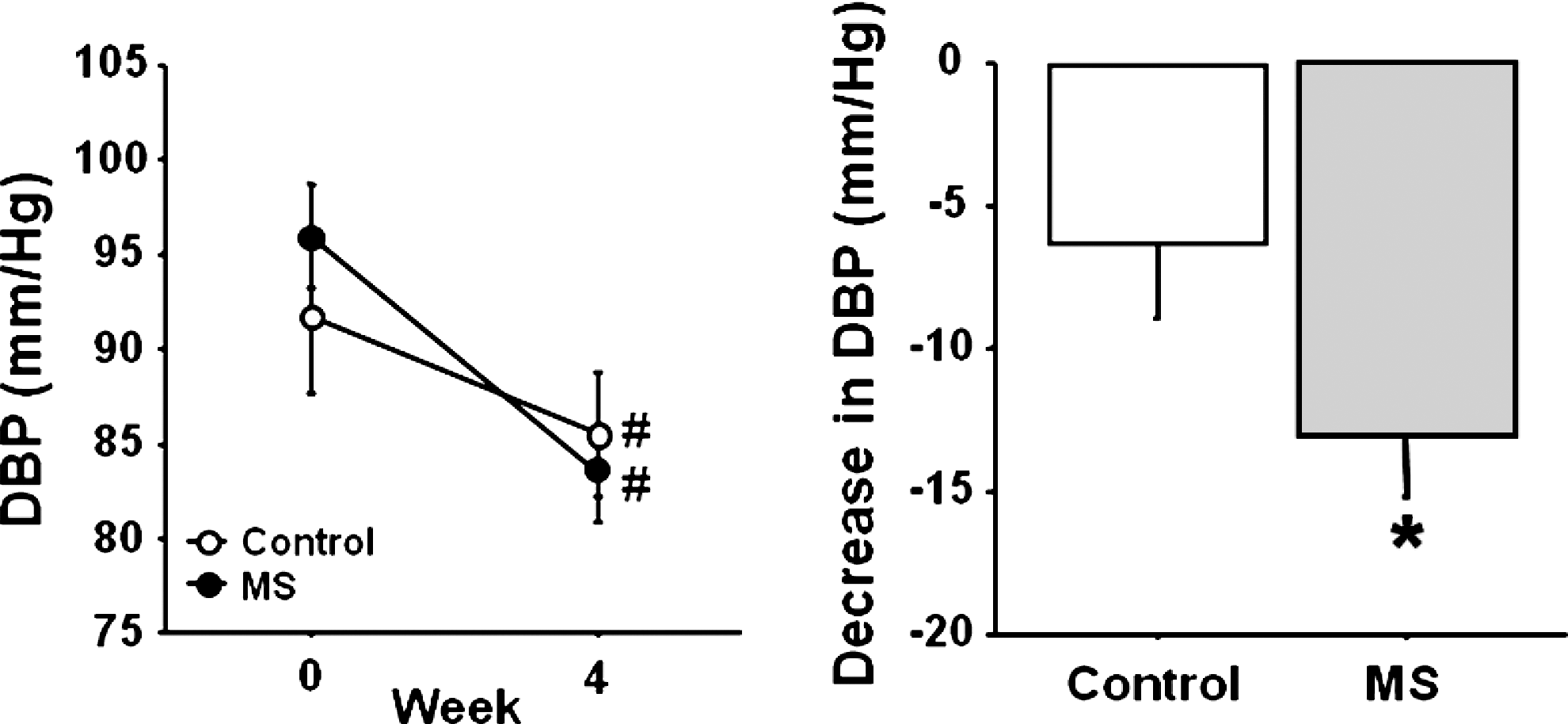
The effect of atenolol on diastolic blood pressure (DBP). DBP at week 0 and week 4 and decrease in DBP in each group are shown. (*) P<0.05 vs. control group by unpaired t-test; (#) P<0.05 vs. week 0 by paired t-test. MS, metabolic syndrome.
Effect of atenolol on pulse rate
Atenolol decreased pulse rate after 4 weeks in the metabolic syndrome group and in the control group (84.3±2.3, 61.8±1.9 beats/min, P<0.0001, 74.3±2.1, 61.4±2.7 beats/min P<0.0001; Fig. 3). Decrease in pulse rate due to the administration of atenolol was significantly greater in metabolic syndrome group than in the control group (21±2, 14±3 mmHg, P<0.05; Fig. 3). There was a positive association between the decrease in pulse rate and waist measurements of the patients (r=0.335, P<0.05). We also found a positive association between the decrease in pulse rate and initial pulse rate (r=0.566, P<0.002). These associations were found in all the patients in this study.

The effect of atenolol on pulse rate (PR). Pulse rate at week 0 and week 4 and decrease in pulse rate in each group are shown. (*) P<0.05 vs. control group by unpaired t-test; (#) P<0.0001 vs. week 0 by paired t-test. MS, metabolic syndrome.
Adverse effects of atenolol
There were no changes in metabolic parameters 4 weeks after the administration of atenolol, and no adverse effects were seen in these patients during the study.
Discussion
In this study, we investigated the potential effect of atenolol on blood pressure and pulse rate in metabolic syndrome patients. First, we found that there was a significant increase in pulse rate in the metabolic syndrome group compared to the control group, and there was a positive association between pulse rate and waist measurement. These findings are consistent with previous data that heart rate is increased in obesity and associated with elevated sympathetic activity. 8,18 Insulin resistance in metabolic syndrome patients can cause increased sympathetic activity. In other words, accumulation of visceral fat due to metabolic syndrome may contribute to increased sympathetic activity and elevating pulse rate. Our data show sympathetic activity may be increased also in metabolic syndrome patients because pulse rate is increased in this group. Because there was a positive association between waist measurement and pulse rate, waist measurement may reflect the severity of sympathetic nerve activity in patients with metabolic syndrome. Patients with early manifestation of diabetic neuropathy may exhibit resting tachycardia. In our study, we compared pulse rate in metabolic syndrome patients with diabetes and without diabetes. However, there was no difference between these groups (81.0±2.3, 80.1±3.2/min).
Decreases in pulse rate, SBP, and DBP due to the treatment were greater in the metabolic syndrome group than in the control group. There was a positive association between decrease in pulse rate and waist measurement, and between decrease in blood pressure and waist measurement. Atenolol seems reasonably to take effect on pulse rate and blood pressure depending on the severity of accumulation of visceral fat, which causes insulin resistance and reflects sympathetic activity. This may show that increased sympathetic nerve activity in metabolic syndrome patients may be attenuated by selectively blocking adrenergic β1-receptor and may result in decreasing pulse rate and blood pressure. There was a positive association between a decrease in pulse rate and initial pulse rate, and a positive association between decrease in blood pressure (SBP and DBP) and initial blood pressure (SBP and DBP) due to the treatment. These results show that higher pulse rate and blood pressure are more sensitive to atenolol, and sympathetic activity is crucial for higher pulse rate and blood pressure in metabolic syndrome patients. Atenolol may exert its effect depending on the severity of high pulse rate and high blood pressure as well as on the severity of the visceral fat.
Essential hypertension has been reported to underlie the pathophysiology of hypertension in obesity and metabolic syndrome. 19 The mechanism of essential hypertension may be involved, at least in part, in insulin resistance. 20 Atenolol may have a stronger effect on increased sympathetic nerve activity caused by insulin resistance in metabolic syndrome compared to essential hypertension with no visceral obesity.
Atenolol does not stimulate intrinsic sympathetic activity (ISA), which can cause a paradoxical phenomenon with increased sympathetic activity such as elevating heart rate. Some advantages of using β-blockers with ISA are that they are not likely to worsen metabolic profiles. 21 However, in controlling blood pressure and heart rate, β-blockers without ISA may have a stronger effect in terms of decreasing blood pressure and heart rate. Among adrenergic β-receptor antagonists, we used atenolol because it is a highly selective β1- antagonist. 22 β-Blockers, especially nonselective ones, have been shown to cause adverse effects on metabolism. Blocking β2-receptors in the β cells in the pancreas may decrease insulin secretion. 23 It is possible that these can deteriorate glucose tolerance, unless the agents are highly selective β1-receptor antagonists. Therefore, atenolol may have less of an influence in worsening glucose metabolism. However, compared to the treatment with carvedilol, a nonselective β-blocker with α1-blocking agent, atenolol decreased blood pressure in the same way in diabetic patients, but it deteriorated glucose and lipid metabolism while carvedilol improved them. 24 In the INternational VErapamil SR-Trandolapril study (INVEST), hypertensives randomized to verapamil-based therapy had a 15% lower incidence of new-onset diabetes than subjects in the atenolol group. 25 In our study, we did not observe any deterioration in those parameters. This may be due to the short duration of the experimental period. Although atenolol may have negative metabolic effects for longer time usage, it may have stronger effects on blood pressure and pulse rate in patients with metabolic syndrome.
In treatment for hypertension with obesity or diabetes, renin–angiotensin drugs are recommended as the first choice. However, oral monotherapy has not been satisfactory in controlling elevated blood pressure in many cases. 26 Although treatment such as increasing the dose of renin–angiotensin drug, adding diuretics, or adding calcium antagonist should be considered if blood pressure control is still poor after administration of the first medicine, 27 adding atenolol in patients with metabolic syndrome might be one strategy for treating hypertension during the period if no deterioration of metabolic profiles or other adverse effects in metabolic syndrome are manifest, especially with increased sympathetic activity reflected by greater waist measurement, higher blood pressure, and higher pulse rate.
Increased heart rate is associated with cardiovascular events and may be due to insulin resistance or hyperinsulinemia. 28,29 Because the importance of controlling heart rate, as well as blood pressure to prevent cardiovascular event has been emphasized, decreasing sympathetic activity in hypertension patients may be crucial to their treatment. Further investigation is needed to clarify the effect of atenolol on metabolic profiles in metabolic syndrome patients with hypertension. Although careful attention to adverse effects should be paid for periods of longer administration, atenolol may be useful in treating elevated blood pressure and heart rate in severe metabolic syndrome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.