
Abstract
Objective:
The aim of this study was to determine the prevalence of metabolic syndrome and the most common combination of cardiometabolic disorders among different ethnic groups of obese adolescents in Malaysia.
Research Design and Methods:
A cross-sectional study among 335 obese adolescent boys and girls aged 12–18 years from 10 randomly selected schools was conducted. After recording blood pressure and waist circumference (WC), a fasting blood sample was obtained and analyzed for glucose and lipids. Metabolic syndrome was diagnosed on the basis of adolescent metabolic syndrome criteria specified by National Cholesterol Education Program Adult Treatment Panel III if three of the five risk factors—hypertriglyceridemia, hyperglycemia, hypertension, low high-density lipoprotein C, and increased WC—were present. The prevalence among different ethnic groups was analyzed.
Results:
The obesity rate among adolescents was 8.4%, and nearly one-third of the obese adolescents had metabolic syndrome. More than 90% of obese adolescents had at least one metabolic abnormality. Metabolic syndrome was more prevalent among obese boys (40.2%) compared to obese girls (17%). Boys had significantly higher mean WC and triglycerides and lower HDL-C (P value 0.0001). Increased WC and triglycerides and high blood pressure comprised the most prevalent (34.3%) risk factor combination followed by WC, low HDL, and high blood pressure (22.5%). Over all, Indians had the highest prevalence of metabolic syndrome (36.4%), followed by Chinese (33.8%) and Malays (27.4%). Elevated triglyceride levels were more prevalent among Chinese, hypertension among Malays, and the other three abnormalities among Indians.
Conclusion:
Indians had the highest prevalence of metabolic syndrome. Increased WC and triglycerides and high blood pressure comprised the most prevalent risk factor combination
Introduction
The prevalence of metabolic syndrome differs in different countries and among different ethnic groups. Asian Indians are said to be a group that is characteristically more insulin resistant and has more components of metabolic syndrome compared to others. 7,8 Although the combination of any three of the five cardiometabolic risk factors constitutes metabolic syndrome, different countries report different combinations of risk factors contributing to the diagnosis. 9,10 Epidemiological data on the distribution of different combination types are sparse. Malaysia is a multiethnic country composed of Malays, Chinese, and Indians. The Penang State's ethnic composition was 42% Chinese, 41% Malays, 10% Indians, and 7% non-Malaysian citizens in 2008 as per a report from Statistics Department of Malaysia.
The combination of metabolic syndrome traits among Malaysians, especially among adolescents, is not known and thus a targeted screening was proposed to answer our research question. Screening of adolescents based on family history was not an option because it failed to detect 30%–60% of children with abnormal lipids and also yielded more false positives. 11,12 Although Reaven, who described this syndrome, did not include obesity in his initial list of metabolic disorders, his suggestion of maintenance of a healthy weight as the best treatment for the syndrome implied that obesity plays a pivotal role in the development of metabolic syndrome. 13 Recent studies have shown that metabolic syndrome is strikingly high among overweight adolescents, and the prevalence is said to increase with increasing obesity. 14 –16 Thus, we carried out a targeted screening of obese adolescent school children to determine the difference in prevalence of metabolic syndrome among the various ethnic groups and the most common combination of risk factors contributing to the diagnosis of metabolic syndrome in this region.
Research Design and Methods
This was a school-based cross-sectional study of adolescents between the ages of 12 and 18 from ten schools in the five districts of Penang State in Malaysia. A random sampling of two schools in each of the four districts of Penang state was performed from a list of all the coeducational schools that had children between 12 and 18 years old and all classes in the morning. There was no suitable coeducational school for the North East District, so one boys' school and one girls' school were chosen.
As part of the School Health Program, the height and weight of all the students were measured without shoes and with light clothing, and body mass index (BMI; the weight in kilograms divided by the square of the height in meters) calculated. Subjects were considered eligible for this study if they were healthy, were between 12 and 18 years of age, and had a BMI that exceeded the cutoff point for their age and gender for obesity as per the International Obesity Task Force (IOTF) standard definition for childhood overweight and obesity worldwide. 17 Exclusion criteria were known cardiac or great vessels abnormalities and known diabetes mellitus.
The study was conducted in compliance with International Ethical Guidelines for Epidemiological studies, which has its origin from the Declaration of Helsinki. It was approved by the Medical Research Ethics Committee (MREC) of the Ministry of Health Malaysia, and informed consent from the parents or guardian and assent from all participating adolescents were obtained.
Information on the use of medication that alters blood pressure, glucose, or lipid metabolism was obtained. Parents provided information about race or ethnic group of the participant and any family history of diabetes, hypertension, hyperlipidemia, or coronary heart disease. The participants were requested to fast for 10–12 h during the night before the study visit. Demographic information, including birth weight, ethnicity, and family and personal history of risk factors for cardiovascular disease, any diagnosed medical condition, and history of taking any medication, was recorded.
During the examination, resting blood pressure after resting in a seated position for 5 min was obtained from the nondominant arm using an automated blood pressure monitor (A&D Medical, Tokyo, Japan) Technicians took waist circumference (WC) measurements rounded to the nearest 0.1 cm. WC was measured at the narrowest part between lowest rib and superior iliac crest.
Fasting venous blood samples obtained from participants were analyzed in a central laboratory for glucose, total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG) using standard laboratory procedures. The fasting plasma glucose was measured using hexokinase method [nicotinamide adenine dinucleotide (NADH), Analyser: AU640], TG by the lipase/glycerokinase/glycerol-3-phosphate oxidase (GPO)/phenol + aminophenazone (PAP) method (Analyser: AU640), and total cholesterol and HDL by the cholesterol esterase method (Analyser: AU640).
Data from the case report forms and laboratory results were entered into the study database by research coordinators following the Cinical Research Centre's internal standard operating procedures and were analyzed by a biostatistician using the statistical software STATA.
Definition
The diagnosis of metabolic syndrome was based on adolescent metabolic syndrome criteria specified by National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III),
14
which defines metabolic syndrome during adolescence as having three or more of the following abnormalities: • Serum triglyceride level of 110 mg/dL (1.24 mmol/L) or higher, • HDL-C level of 40 mg/dL (1.03 mmol/L) or lower, • Elevated fasting glucose of 110 mg/dL (6.05mmol/L) or higher, • Blood pressure at or above the 90th percentile for age, sex, and height, • Waist circumference at or above the 90th percentile for age and sex [Third National Health And Nutrition Examination Survey (NHANES III) data set].
On the basis of the Penang State's childhood obesity rate of 6% and a 28.7% prevalence rate of metabolic syndrome among obese American adolescents, a sample size of 315 was determined. 14
Results
The profile of the study population is given in Fig. 1. A total of 335 adolescents (194 obese boys and 141 obese girls) aged 12–18 years old and confirmed to be obese for age, gender, and height were enrolled in the study. Anthropometric and metabolic characteristics of enrolled adolescents are given in Table 1.

Study profile.
SD, standard deviation; CI, confidence interval; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
The prevalence of obesity was highest among Malays (9.7%), followed by Indians (8.1%) and then Chinese (6.6%). Obesity was more prevalent among boys than girls (9.9% vs 6.7%). Because this study was on obese adolescents, there were more boys enrolled in the study, and the percentage of boys among Malays, Chinese, and Indians was 49.2%, 67.5%, and 74.5%, respectively. The mean BMI of enrolled adolescents was almost the same in both genders (32 and 32.4)
The prevalence of family history of diabetes mellitus, hypertension, hyperlipidemia, and coronary heart disease among the children identified to have metabolic syndrome was 33%, 31%, 21%, and 11.5%, respectively, compared to 24%, 32%, 16%, and 6.4% of adolescents without metabolic syndrome, and there was no significant difference between the two groups. There was no family history of the above illnesses in 50% of adolescents with metabolic syndrome and 49% without metabolic syndrome. However, these were self-reported history by parents, and the reliability of the information was not verified. The prevalence of metabolic syndrome and individual risk factor components among enrolled adolescents based on the NCEP ATP III criteria are shown in Table 2.
Data are percentages±standard error of the mean (SEM).
Chi-squared test.
Of the 335 students enrolled, only 19 (5.7%) did not have any abnormality. A total of 316 students, or 94.3% [confidence interval (CI) 91.4–96.6], had at least one metabolic abnormality, 66.9% (CI 61.5–71.9) had at least two abnormalities, and 102 students, or 30.4% (CI 25.6–35.7), had three or four abnormalities fulfilling the criteria for diagnosis of metabolic syndrome. Twenty-one adolescents (6.3%) had four abnormalities and no one had all five abnormalities. Among the ethinic groups, 93% of Indians and Malays and 96% of Chinese had at east one metabolic abnormality.
Frequency of cardiometabolic abnormalities
The prevalence of individual cardiometabolic abnormalities among enrolled adolescents is shown in the Table 3. The most common abnormality was elevated blood pressure, followed by central obesity despite using a WC cutoff point used for American adolescents. Hypertriglyceridemia and low HDL-C followed as third and fourth in the order. Plasma glucose was elevated only in 3 students.
HDL-C, high-density lipoprotein cholesterol.
Prevalence of metabolic syndrome by gender and ethnic group is shown in Fig. 2. Boys had a higher prevalence of metabolic syndrome compared to obese girls [odds ratio (OR)=0.31; 95% CI 0.18–0.54]. Other researchers have also reported this higher prevalence among boys. 18 Individual metabolic abnormalities also were significantly higher among boys compared to girls, except for high blood pressure, which was more prevalent among girls. In a subset analysis, the mean WC and triglycerides were found to be significantly lower among girls compared to boys (P<0.0001 and P=0.003, respectively). Mean HDL-C was also lower among boys compared to girls (p=0.0001). The mean systolic blood pressure (SBP) was 2 mm higher among boys and mean diastolic blood pressure (DBP) was 2 mm higher among girls; the difference was not statistically significant.
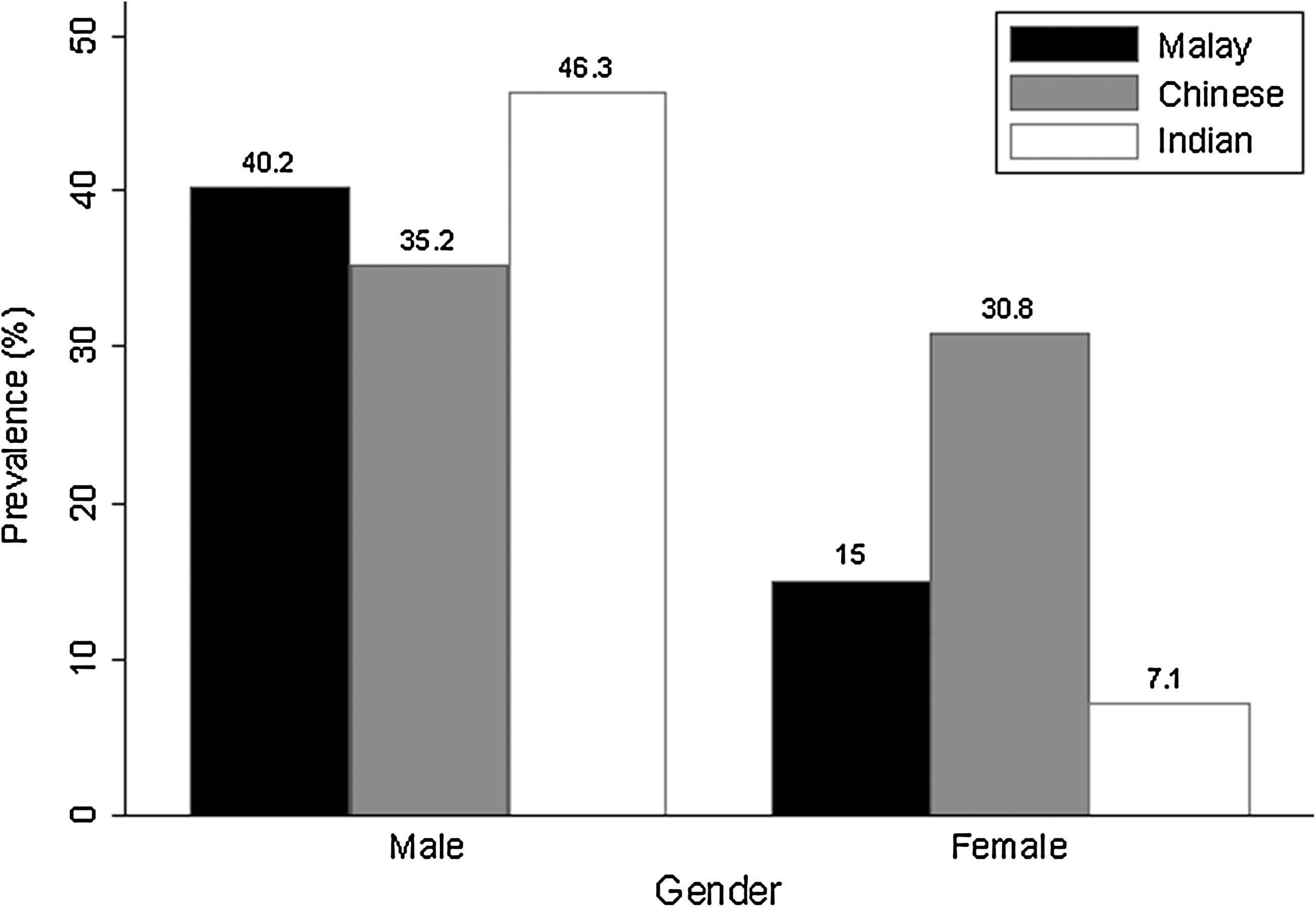
Prevalence of metabolic syndrome by gender and race/ethnicity.
Among the three major ethnic groups in Penang State, Indians had the highest prevalence of metabolic syndrome followed by Chinese and then the Malays (36.4%, 33.8%, and 27.4%). Indians had higher prevalence for hyperglycemia, large WC, and low HDL-C, whereas Chinese had a higher prevalence for hypertriglyceridemia and Malays had a higher prevalence of hypertension. However, the difference was statistically significant only for mean HDL-C level. When gender-specific data were considered, Indian boys had the highest rate of metabolic syndrome (46.3%), followed by Malay (40.2%) and Chinese boys (35.2%). Among girls, Chinese had highest prevalence of metabolic syndrome (30.8%), followed by Malay (15%) and Indian girls (7.1%).
The 13-year-old age group had the highest prevalence of metabolic syndrome; the lowest prevalence was among 16-year-olds, although the difference in prevalence between different age groups was not statistically significant.
Combination of metabolic syndrome traits
In the analysis on the combination of the metabolic abnormalities, increases in WC, TG, and hypertension were the most prevalent (34.3%) risk factor combination in both boys and girls, followed by WC, low HDL, and high blood pressure (22.5%). The most prevalent combination among Malays and Chinese was WC, TG, and blood pressure, but the most prevalent combination among Indians was WC, TG, blood pressure, and low HDL.
Discussion
Obese individuals are known to have a higher prevalence of metabolic syndrome. Even among obese students, the mean BMI of children with metabolic syndrome was higher than the mean BMI of those not diagnosed with metabolic syndrome. Ram Weiss found that each half-unit increase in the BMI and each unit of increase in insulin resistance was associated with an increase in the risk of the metabolic syndrome (OR of 1.55 and 1.12, respectively). 18
Family history did not provide any indication of the presence or absence of metabolic syndrome, because an equal number of adolescents both in metabolic syndrome and nonmetabolic syndrome groups did not give any family history of cardiometabolic disorders. Elizabeth et al. have noted that lipid screening based on positive family history will miss a substantial number of children with hyperlipidemia. 11
Our prevalence rate of one abnormality in 94% is much higher than the prevalence reported in the study among adolescents in South India, where 85% of overweight children had one or more cardiometabolic abnormalities. 19 In this study, 6.4% had four cardiometabolic abnormalities. It has been reported that greater the number of the risk factors a person has, the greater will be the extent and severity of atherogenic disease. 20
In our study, slightly more than one-third of obese Indian adolescents had metabolic syndrome compared to two-thirds of adolescent Indians with high BMI reported by Anoop Misra. 21 Adult Indians were also said to have low HDL-C, insulin resistance, and high plasminogen activator inhibitor type 1, making them more susceptible to coronary heart disease (CHD). 22 This trend probably tracks from childhood through adolescence to adult life. In this study, whereas the most prevalent combination among Malays and Chinese was WC, TG, and blood pressure, Indians had low HDL added to that as the fourth component.
In a hierarchy of combinations of risk factors, WC stands out foremost (93%) and this is in agreement with the proposal made by International Diabetes Federation that central obesity is an essential component of metabolic syndrome. 23 One Japanese and a Korean study also reports abdominal obesity to be the most prevalent of the metabolic syndrome criteria in their obese adolescents. 24,25 The hypertiglyceridemic waist (HW) phenotype rather than overweight is said to predict the presence of cardiovascular risk factors better. 26
Combination of risk factors
On the basis of the definition of three out of five traits needed for the diagnosis of metabolic syndrome, there could be 16 different combinations. It is being debated whether each combination uniformly increases the risk for cardiovascular outcome. Differences in the clustering of metabolic parameters have been shown in different ethnic groups. There is a suggestion that different combinations of the metabolic syndrome criteria best predict cardiovascular risk in different ethnic groups. 27 Among Hispanic and white adolescents, a large WC and high fasting TG and low HDL-C concentrations were the most prevalent combination. 28 Studies done in Iran found high TG and low levels of HDL-C as the most common components of metabolic syndrome among children and adults, probably reflecting the ethnic predisposition in that region. 29 –32
In our study, WC, TG, and blood pressure were the most common combination, followed by WC, low HDL, and blood pressure. A study analyzing the data among Germans- “GErman Metabolic and CArdiovascular RiSk Project (GEMCAS) Data” also reported WC, TG, and blood pressure to be the most prevalent combination among the younger age group of men (18–35 years), just as in our study. 33 This study also reported that a 10-year risk of myocardial infarction was highest for young men with the WC, TG, and HDL combination and young women with the TG, HDL, and blood pressure combination. A prospective cohort study needs to be undertaken to determine the cardiovascular risk posed by each metabolic syndrome combination type.
Strength and limitations
The strengths of our study are the statewide approach and random selection of schools. Being a community-based sample, it provides greater generalizability than the clinic-based samples of overweight adolescents. Clustering of risk factors confirms the high prevalence of this syndrome among obese adolescents in Penang, and the impact of the data may be far reaching.
Limitations of this study are the cross-sectional design that does not give any indication regarding the duration of the existence of any risk factor and does not include the effect of pubertal changes. The lack of data on pubertal staging, which might possibly affect WC differentially in boys and girls, was controlled by using age and gender-based WC percentiles. The selection of only school-going adolescents from co-educational schools may not be representative of all adolescents of Penang State and may limit the generalizability of the findings.
Conclusions
We already know that: • Metabolic syndrome was considered to be an adult problem. • Now it is accepted that the clustering starts early in life may be even in utero. • The prevalence and the components differ among different ethnic groups and different combinations confer different cardiovascular risk rates. • The prevalence of metabolic syndrome among Malaysian adolescents or the commonest combination in different ethnic groups is not known.
Despite using a pediatric definition of NHANES, which leads to lower prevalence estimates in adolescents by 4%, nearly one-third of obese Malaysian adolescents were found to have metabolic syndrome.
14
Our findings suggest that obese adolescents, regardless of ethnic differences, have a high prevalence of metabolic syndrome. Our study has found that: • Nearly one-third of obese adolescents in Penang suffer from metabolic syndrome. • The commonest combination in this region is WC, blood pressure, and TG. • Just as in adults, even during adolescence Indians have the highest prevalence of metabolic syndrome and they have more risk factors; their significant difference is low HDL-C.
The impact of the data is far reaching and will help the policy makers to implement preventive measures.
Further research is needed to investigate the various genetic, cultural, and environmental factors that might influence the overall prevalence and the different combinations of metabolic syndrome. To date, there have been no studies determining the disease burden of metabolic syndrome among adolescents of different ethnicity in Malaysia. Routine screening of obese adolescents for metabolic syndrome may be necessary to identify the subgroup at risk for cardiovascular disease and to target for lifestyle behavior changes. Comparative nationally representative data are needed for policy makers to plan primary prevention strategies.
Footnotes
Acknowledgments
This study was funded by Ministry of Health Malaysia. We thank the Ministry of Health Malaysia and the Director General of Health for giving us permission to publish this article; the Ministry of Education, Malaysia, the school principals, teachers, parents, and students who participated in the study; and the staff of Clinical Research Centre of Penang Hospital for helping with data collection.
Author contributions were: P.N. researched the data, contributed to discussion, and wrote and edited the manuscript; O.L.M. contributed to the discussion and reviewed the manuscript; M.O. researched the data and helped with statistical analysis.
Author Disclosure Statement
The authors do not have any conflict of interest to disclose. No competing financial interests exist.