
Abstract
Background:
The International Diabetes Federation (IDF) defines metabolic syndrome among children. In addition to the abdominal obesity (waist circumference ≥90 percentile of locally representative sample), the risk criteria for metabolic syndrome includes elevated blood pressure, hypertriglyceridemia, low high-density lipoprotein cholesterol (HDL-C) levels, and elevated fasting glucose. In this study, we compared the association of anthropometric indices with metabolic syndrome risk criteria in 9-year-old children.
Methods:
A cross-sectional study of 9-year-old children (n=1,194) was performed in 2007–2008. Using the international cutoff points and percentiles, we determined subjects with elevated blood pressure, hypertriglyceridemia (≥90 percentile), low HDL-C (≤ 10 percentile), and elevated fasting glucose (≥100 mg/dL). We compared several anthropometric indices [triceps skin-fold thickness (SFT), waist circumference, hip circumference, waist-to-hip ratio, body mass index (BMI) and waist-to-height ratio] and their association with metabolic syndrome risk criteria other than waist circumference among 9-year-old children.
Results:
Metabolic syndrome risk criteria were commonly observed among 9-year-old children: 244 students (20.4%) had hypertriglyceridemia and/or low HDL-C, 362 students (30.3%) had elevated blood pressure, and 254 (21.3%) students were overweight or obese. Among covariates of SFT, BMI, waist circumference, waist-to-hip, or waist-to-height ratio categories, the BMI category was the only significant predictor of having two or more metabolic syndrome risk variables [odds ratio (OR)=3.5, 95% confidence interval (CI) 1.69–7.41, P=0.001 for boys and OR=4.7, 95% CI 1.61–13.55, P=0.005 for girls].
Conclusions:
Assessing anthropometric indices is crucial for early detection and prevention of metabolic syndrome among children and adolescents. Age- and sex-specific cutoff points of BMI can be used to screen for the metabolic syndrome and related risk criteria among 9-year-old children.
Introduction
Recently, the International Diabetes Federation (IDF) published a consensus definition of metabolic syndrome for children and adolescents. 4 The IDF definition consists of abdominal obesity and two or more clinical features, including high blood pressure, hypertriglyceridemia, low high-density lipoprotein cholesterol (HDL-C), and elevated fasting glucose. More research and data are needed for children under 10 years of age. The IDF definition considers abdominal obesity (waist circumference ≥90th percentile of locally representative sample) as a prerequisite for metabolic syndrome. Waist circumference percentiles in a population are influenced by the population's ethnicity. More importantly, adequate percentile information in a locally representative sample may not be available particularly for developing countries. Therefore, alternative and readily available anthropometric criteria are needed.
Body proportions normally change during pubertal development and may vary among children of different races and ethnic groups. Age- and sex-specific cutoff points of body mass index (BMI) are provided to assess the overweight and obesity status in children. 5,6 Certain disadvantages exist with BMI as a sole anthropometric assessment tool. BMI is not a measure of fat distribution and may underestimate the excess fat. Hence, additional anthropometric indices are required to estimate the fat distribution among children. For instance, an increase in waist circumference defines central obesity. Waist-to-hip ratio indicates abdominal obesity and correlates well with metabolic syndrome risk criteria. 7 Recently, waist-to-height ratio is reported as another anthropometric index of fat distribution in children. An increased waist-to-height ratio is associated with higher metabolic risk in children. 8 Similarly, skin-fold thickness (SFT) is a well-established anthropometric index for cardiovascular risk assessment among children. 9
In this study, we compared the association of anthropometric indices (triceps SFT, waist circumference, hip circumference, BMI, and waist-to-hip and waist-to-height ratios) with metabolic syndrome risk criteria (other than waist circumference) in children.
Methods
This cross-sectional study was performed in 2007–2008 among 9-year-old elementary school students attending state schools in the Uskudar region of Istanbul, Turkey. The study was designed to determine the prevalence of cardiovascular risk factors, including high blood pressure and elevated fasting blood glucose or lipid levels among school students. Each student underwent complete medical history and physical examination. Students with acute or chronic medical problems and/or those who did not want to participate in the survey were excluded (∼20%). Subjects were instructed to fast for at least 12 h before the screening. Their compliance was ascertained by an interview on the day of examination. The fasting status was based on self-report. Blood samples were drawn at 9 a.m. and screening took place during normal school hours.
Measurements
Anthropometric measurements included weight, height, blood pressure, SFT, waist and hip circumferences, and arm span. Standardized protocols were used by the trained examiners. The weight of children wearing minimal clothing was measured to the nearest 0.1 kg with a portable electronic scale. Each time it was moved, the scale was recalibrated and standardized. Height was measured with a fiberglass tape. BMI was calculated as weight (kg) divided by height square (m2). Body circumferences were measured with subjects in the standing position. Hip and waist (just above the iliac crest) circumferences were measured to the nearest 0.1 cm. Using the tables provided by the waist circumference percentiles in a nationally representative sample, we determined subjects with increased waist circumference (≥90th percentile). 10
Body proportions normally change during pubertal development and may vary among persons of different race and ethnic groups. Age- and sex-specific cutoff points of BMI were used to assess the overweight or obesity status. The cutoff points of BMI were previously developed and published from the centile curves of an international reference population. 5,6 Height, waist and hip circumferences were used to calculate the waist-to-hip or waist-to-height ratios. A waist-to-hip ratio >0.9 and a waist-to-height ratio >0.5 were considered as indicators of abdominal obesity. 7,8 Triceps SFT was measured to the nearest 1.0 mm with a Holtain caliper. SFT was compared to the U.S. data adopted from National Center for Health Statistics. 11 Increased SFT is defined as >85th percentile.
Blood pressure was measured three times while the subjects were seated by an automatic blood pressure monitor (Omron®). The average of the last two measurements was used for the analysis. Small and medium-sized cuffs were used for the arm circumferences of <22 and 22–32 cm, respectively. To find the age-specific height percentile, we used the growth curves drawn for healthy Turkish Children. 12 Using the tables provided by the Task Force Report on High Blood Pressure in Children and Adolescents, we determined children and adolescents with elevated blood pressure (≥95th percentile). 13
Triglycerides (TG), HDL-C, and glucose were measured by enzymatic colorimetric-assay methods. Because age- and sex-specific lipid percentiles are not available in Turkish children, we used the National Heart Lung and Blood Institute Growth and Health Study (NGHS) as the reference population. 14 A TG level ≥90th percentile or HDL-C level≤10th percentile were considered as risk determinants of metabolic syndrome in children.
Metabolic syndrome risk criteria
The IDF definition of metabolic syndrome among children consists of abdominal obesity and two or more clinical risk features, including high blood pressure, hypertriglyceridemia, low HDL-C, and elevated fasting glucose. 4 Using the international cutoff points and percentiles, we determined subjects with high blood pressure (systolic or diastolic blood preesure ≥95th percentile), 13 elevated TG (≥90th percentile), 14 low HDL-C (≤10th percentile), 14 and elevated fasting glucose ≥100 mg/dL. 15
Statistical analysis
The Kolmogorov–Smirnov test was used to analyze the distribution of the variables. Anthropometric indices displayed skewed distribution. Median [interquartile range (IQR)] numbers were displayed for variables with skewed distribution. Comparisons between the groups were performed using Mann–Whitney test (Table 1). Percentages were displayed for categorical variables, and the chi-squared test was used to compare the groups. The nonparametric Spearman test was used to analyze the correlation between the total number of metabolic syndrome risk criteria other than waist circumference (elevated glucose, elevated TG, elevated blood pressure, and low HDL-C) and anthropometric indices.
Categorical variables are presented in percentages.
BMI, body mass index; SFT, triceps skin fold thickness.
Receiver operating characteristic (ROC) curves were constructed to assess the anthropometric indices (triceps SFT, waist circumference, waist-to-hip ratio, waist-to-height ratio, and BMI) and presence of two or more metabolic syndrome risk criteria other than waist circumference. Logistic regression analysis was performed to determine the predictors of subjects with two or more metabolic syndrome risk criteria (elevated glucose, elevated TG, elevated blood pressure, and low HDL-C). Covariates included SFT (≤ or >85th percentile), BMI (overweight and obesity based on age- and sex-specific cutoff points), waist circumference (<or ≥90th percentile), waist-to-hip (≤ or >0.9) or waist to height (≤ or >0.5) ratio categories. A P value <0.05 on the two-sided test was considered to be statistically significant. The statistical analysis was performed by STATA 11.
Results
Nine-year-old elementary school students were enrolled in the study (N=1,194, 586 boys and 608 girls). A total of 244 children (20.4%) had hypertriglyceridemia (≥90th percentile) and/or low HDL-C (≤10th percentile). Only 4 (0.3%) had elevated fasting glucose; on the other hand, 362 (30.3%) subjects had elevated blood pressure (≥95th percentile).
Anthropometric indices revealed that 254 subjects (21.3%) were overweight or obese based on BMI according to the international criteria, 161 subjects (13.5%) had elevated waist-to-height ratio (>0.5), 141 subjects (11.8%) had elevated waist-to-hip ratio (>0.9), 218 subjects (18.3%) had increased waist circumference (≥90 percentile), and 151 subjects (12.6%) had increased SFT. Comparisons of anthropometric indices were performed between the subjects with two or more or less than two risk criteria for metabolic syndrome (other than waist circumference) (Table 1).
We analyzed the correlations between the total number of metabolic syndrome risk criteria (elevated glucose, elevated TG, elevated blood pressure, and low HDL-C) and anthropometric indices. Among girls and boys, BMI displayed the most significant correlations with the total number of metabolic syndrome risk criteria (r=0.239, P<0.0001 and r=0.274, P<0.0001, respectively). Hip circumference (r=0.212, P<0.0001 for girls and r=0.195, P<0.0001 for boys), waist-to-height ratio (r=0.185, P<0.0001 for girls and r=0.119, P=0.004 for boys), waist circumference (r=0.197, P<0.0001 for girls and r=0.139, P=0.001 for boys), and SFT (r=0.185, P<0.0001 for girls and r=0.195, P<0.0001 for boys) also displayed significant correlations with the total number of metabolic syndrome risk criteria (Fig. 1).
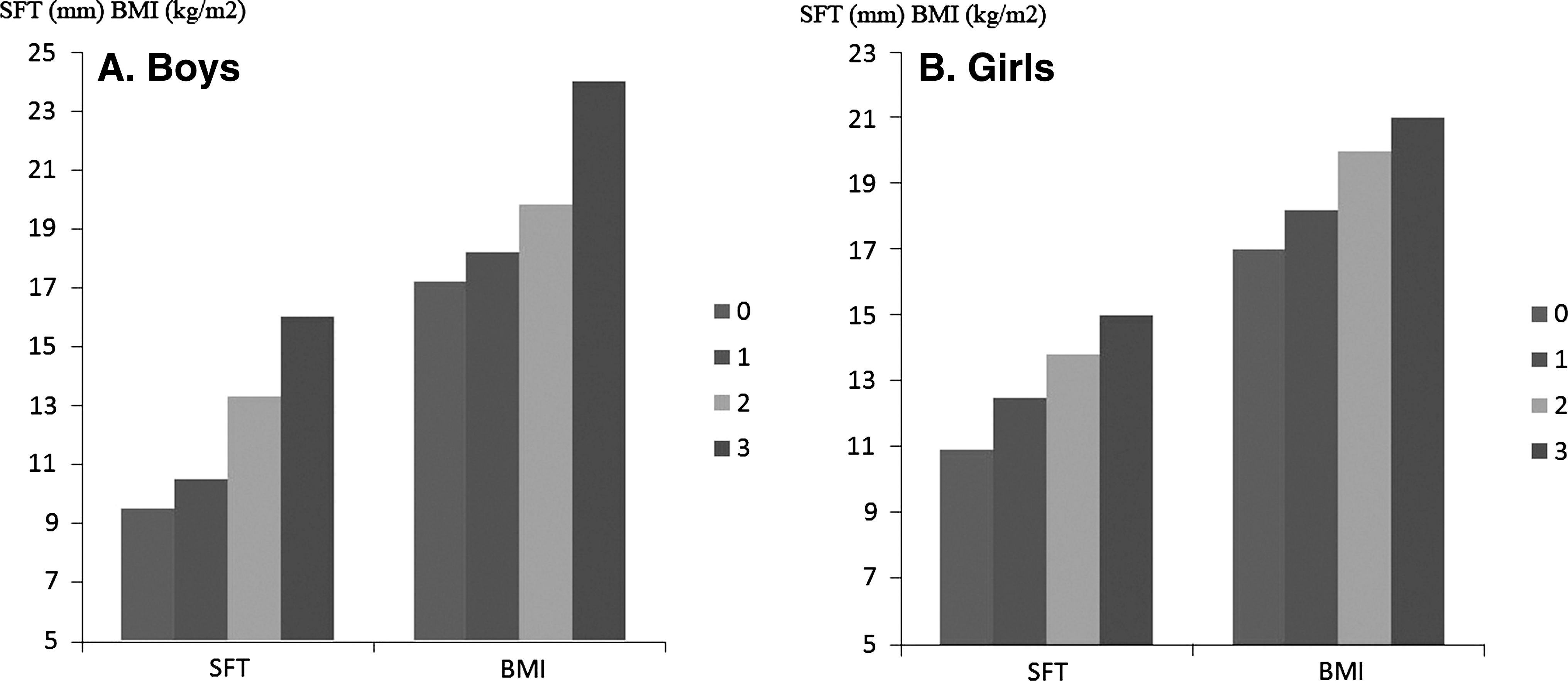
Skin fold thickness (SFT) and body mass index (BMI) display significant correlations with the total number of metabolic syndrome risk criteria (other than waist circumference).
ROC curves (for having two or more metabolic syndrome risk criteria other than waist circumference) are shown in Fig. 2. Areas under the curve (AUC) for BMI were 0.69 and 0.74, for SFT were 0.65 and 0.68, for waist circumference were 0.65 and 0.63, and for hip circumference were 0.66 and 0.68 among girls and boys, respectively.
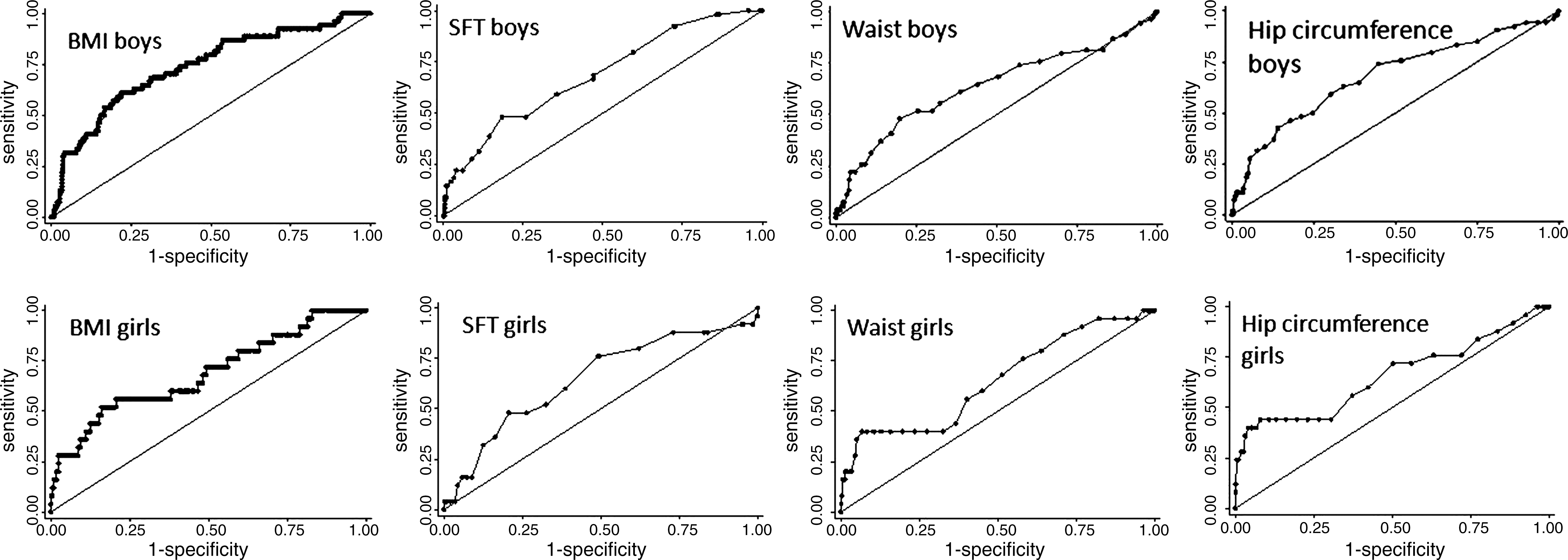
Receiver operating characteristic (ROC) analysis curves for metabolic syndrome and anthropometric indices [triceps skin fold thickness (SFT), waist circumference, hip circumference, body mass index (BMI)].
Logistic regression analysis was performed to find the predictors of having two or more metabolic syndrome risk criteria other than waist circumference (elevated glucose, elevated TG, elevated blood pressure, and low HDL-C). Among covariates of SFT (≤ or >85th percentile), BMI (overweight and obesity based on age- and sex-specific cutoff points), waist circumference (<or ≥90th percentile), waist-to-hip (≤ or >0.9) or waist-to-height (≤ or >0.5) ratio categories; BMI category [odds ratio (OR)=3.5, 95% confidence interval (CI) for OR were 1.69–7.41, P=0.001 for boys and OR=4.7, 95% CI for OR were 1.61–13.55, P=0.005 for girls] was the only significant predictor of having ≥2 metabolic syndrome risk criteria (Table 2). Hence, overweight and obesity status (based on age- and sex-specific cutoff points) increased the risk of having two or more metabolic syndrome risk variables (other than waist circumference) by 3.5- and 4.7-fold among boys and girls, respectively.
OR, odds ratio; CI, confidence interval; BMI, body mass index; SFT, triceps skin fold thickness.
Discussion
In this study, we compared several anthropometric measures and their relation to metabolic syndrome risk criteria in 9-year-old children. Overweight or obesity status based on the curves of an international reference population was the most significant predictor of having two or more metabolic syndrome risk criteria other than waist circumference. Assessing anthropometric indices regularly may enable early interventions to prevent metabolic syndrome.
Our study has several limitations. The study was cross sectional. We did not perform analysis of diet and physical acitvity. We selected public schools from a low to middle socioeconomic class region. It is difficult to prove that these children are representative of all schoolchildren. Obviously, larger prospective studies are needed to assess temporal changes in anthropometric indices among children. Socioeconomic status and diet can affect serum lipid levels and the prevalence of metabolic syndrome among children. To test the effects of diet and other environmental factors, larger cohorts are needed.
The National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), the World Health Organization (WHO), and the IDF define metabolic syndrome in adults. 1,16,17 These definitions consider different anthropometric indices. The NCEP definition is based on a number of risk factors, including abdominal obesity. 16 The IDF definition considers central obesity as the prerequisite, and it has broader criteria for waist circumference. 1
Childhood obesity is an important public health concern. The clustering of metabolic syndrome risk criteria increases the risk for cardiovascular disease and the new onset of diabetes, although prospective studies are limited in children. 1,16,17 There is increasing evidence that metabolic syndrome starts early in life. 2,3 The IDF criteria considers waist circumference ≥90 percentile as a prerequisite for metabolic syndrome among children ≥10 years of age. 4 IDF suggests that metabolic syndrome should not be diagnosed in children younger than 10 years, but a strong message for weight reduction should be delivered. On the other hand, the Bogalusa Heart Study indicates that cardiovascular risk starts early in childhood. 18,19 Hence, it is particularly important to identify anthropometric indices associated with cardiovascular risk for children under 10 years of age. In fact, our findings suggest that metabolic syndrome risk criteria are commonly observed in 9-year-old school children.
Ethnic differences exist in the criteria, definition, and prevalence of metabolic syndrome in children between populations. 20,21 It is crucial to understand the ethnic differences to develop effective screening strategies. We examined a representative sample of apparently healthy students from Istanbul. Each country must have its own reference values to identify obesity and metabolic disturbances. Further disparity among antropometric indices may exist among different regions and socioeconomical classes within the same country. Our findings suggest that overweight or obesity based on the internationally defined curves of BMI may help to monitor the cardiovascular risk among children. We studied children under 10 years of age who were not included in the IDF definition. 4 The current results underscore the importance of assessing BMI in children to identify overweight or obese subjects based on the international cutoff points. BMI may present a more practical anthropometric index, particularly in the absence of the local percentile information for waist circumference.
Our observations support prior studies suggesting that BMI correlates better with blood pressure and dyslipidemia than does waist circumference. 22 On the other hand, both general and abdominal adiposity are associated with cardiovascular risk. It is important to estimate the body fat distribution accurately for the prevention of metabolic syndrome in children.
Metabolic syndrome in childhood predicts the impending cardiovascular disease and type 2 diabetes mellitus in adulthood. 23 Anthropometric indices are useful for identifying children with metabolic syndrome and its components. In obese children, physical training alone can improve the lipid levels and prevent metabolic syndrome. 24 Future prospective studies are needed to identify the anthropometric criteria that associate with metabolic syndrome risk criteria among children. Dietary, physical activity scores, and ethnic differences are all crucial to build up the effective screening strategies for metabolic syndrome and childhood obesity particularly among the developing countries.
Footnotes
Acknowledgments
The authors would like to thank the schools and students for their participation. This study is funded by Scientific Research and Projects Commission of Marmara University (BAPKO SAG-D-131008-0241) and Uskudar Municipality.
Author Disclosure Statement
The authors have no conflicts to disclose.