
Abstract
In this article we review the association of three principal factors of the metabolic syndrome— insulin resistance, hypertension, and increased levels of inflammation factors—with several chronic, nonatherosclerotic conditions associated with aging—frailty, cognitive decline, impaired cardiovascular autonomic control, and possibly osteoporosis. We hypothesize that the metabolic syndrome is associated with “accelerated” aging.
Introduction
The purpose of this brief review is to bring to the reader's attention several age-related, nonatherosclerotic, chronic diseases that are associated with metabolic syndrome. These disorders include frailty, cognitive decline, impaired cardiovascular autonomic control, and possibly osteoporosis (Fig. 1). We present data to suggest that the principal factors underlying metabolic syndrome may lead to “accelerated aging.”
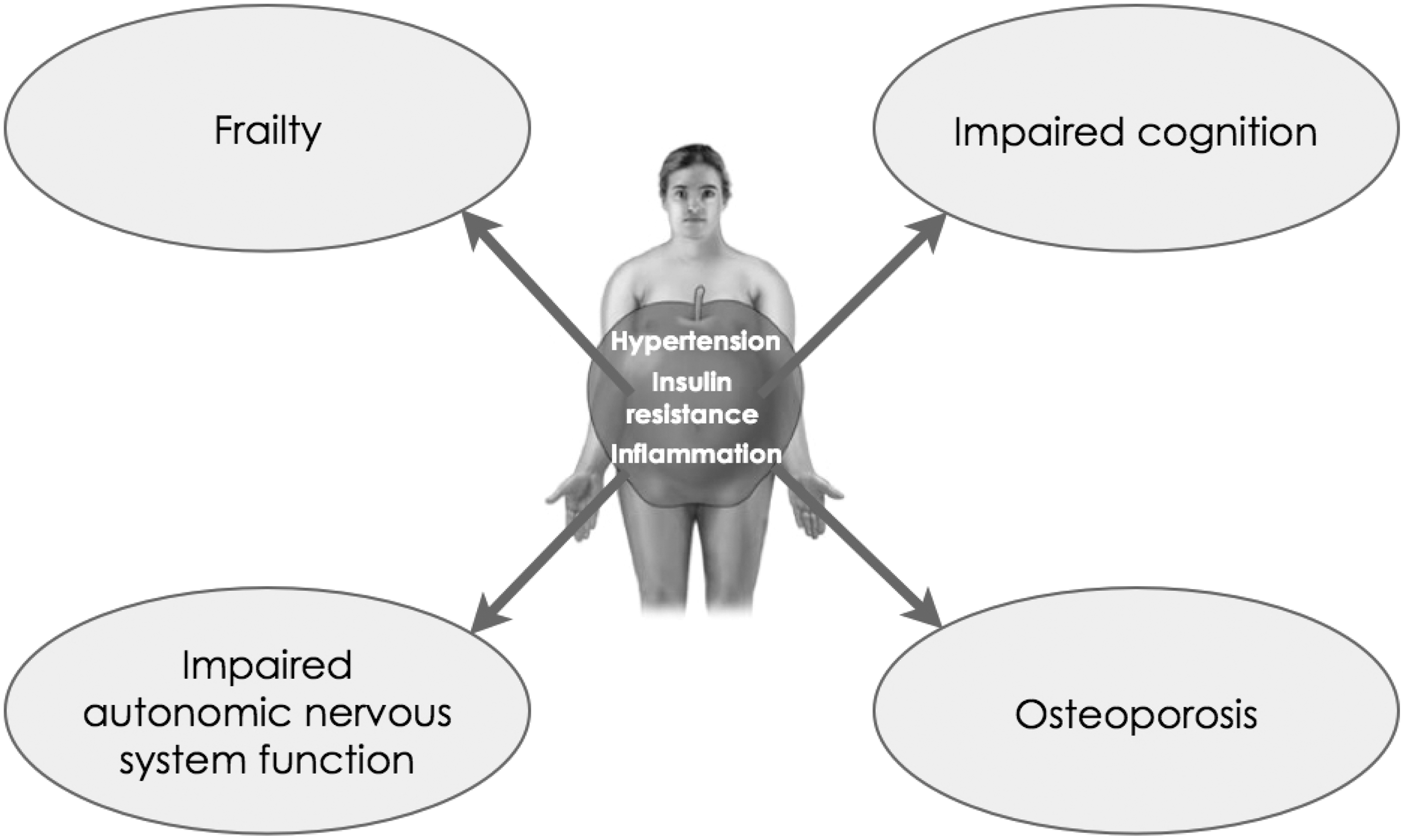
Noncardiovascular complications of the metabolic syndrome.
Frailty
The geriatric syndrome of frailty is characterized by decreased reserve in multiple physiological systems. 6 It predicts adverse health outcomes independent of advancing age, chronic disease, and functional limitations, thereby suggesting that it is a distinct condition. 7 On the basis of data derived from the Cardiovascular Health Study (CHS) and the Women's Heath and Aging Studies, frailty is characterized by involuntary weight loss, exhaustion, low physical activity, slowness, and weakness. Those with three or more of these criteria are considered frail, whereas those with one or two criteria are considered “pre-frail,” an intermediate syndrome with increased risk for the development of frailty. Weakness (diminished grip strength), diminished walking speed (time to walk 15 feet), exhaustion (“everything is an effort”), and low activity levels are frailty's most common factors; weight loss is less common.
We examined the association of metabolic syndrome with frailty. In our first paper, 8 based on a cross-sectional evaluation of CHS participants, we found significant elevations in fasting insulin levels and glucose levels 2 h after an oral glucose tolerance test in association with decline in physiological function. This decline was independent of diabetes and cardiovascular disease. We also found that the inflammation proteins C-reactive protein (CRP), fibrinogen, and factors VII and VIII were elevated among those with declines in physical function. These variables are characteristic of the metabolic syndrome. In a subsequent study, we reexamined these findings prospectively. 9 We found that two principal components of the metabolic syndrome—insulin resistance, as measured by homeostasis model assessment (HOMA-IR), and increased levels of the inflammation protein CRP—were associated with increased risk for the development of frailty. A 1 standard deviation increase in each factor independently and significantly increased the risk of incident frailty by 1.15 (1.02, 1.31) and 1.16 (1.02, 1.32), respectively. Of interest, metabolic syndrome itself was not a significant risk factor for frailty [hazard ratio (HR) 1.05 (0.92, 1.19)], although it was significantly associated with prefrailty [HR 1.28 (1.07, 1.53)]. Our analyses were performed in people who did not have diabetes, cardiovascular disease, or other chronic illnesses. As such, these estimates were conservative because many people with metabolic syndrome have a high burden of chronic illness. We also found that participants who developed frailty during follow-up were twice as likely to develop diabetes as those who did not develop frailty.
We speculated about how frailty could be related to insulin resistance and inflammation. One possibility was that inflammation and oxidative stress were the primary factors underlying this association. Increased levels of inflammation factors have been implicated in muscle weakness and age-related declines in physical function. 10 Alternatively, it was possible that a primary defect in muscle sensitivity to insulin was the connecting link between frailty, HOMA-IR, and inflammation. Supporting this possibility are studies of older adults with impaired insulin sensitivity who demonstrate impaired muscle protein breakdown or production. 11 Also, impaired muscle quality may result in impaired energy regulation and performance as seen in frailty. 12 An analysis of the Health, Aging, and Body Composition (Health ABC) Study supports this latter possibility. 13 In this study, HOMA-IR was associated with decreased quadriceps muscle strength (P<0.001) in regression analysis in nondiabetic adults, aged ≥70 years, even after accounting for total body fat mass, level of physical activity, and quadriceps muscle fat content [as measured by magnetic resonance imaging (MRI)]. The decrease in strength, while measurable, was subclinical because all of the participants in this study had no difficulty walking or climbing. In line with this latter hypothesis are findings from the Diabetes Prevention Program, showing that the greatest reduction in progression to diabetes in people with insulin resistance was in people who exercised and increased muscle strength as compared to those who do not so do [HR 0.470, 95% confidence interval (CI) 0.28,0.78]. 14 Another prospective study demonstrated that older adults who exercised >1 h per day had insulin sensitivity similar to trained younger adults. 15
In summary, several aspects of frailty appear to be related to inflammation and insulin resistance, supporting the hypothesis that the conditions are causally related.
Cognitive Decline
People with diabetes mellitus (DM), a downstream consequence of metabolic syndrome, have an increased odds of having or developing cognitive impairment. 16 The risk has been estimated at 1.6 (95% CI 1.4, 1.8) that of nondiabetic individuals. The role of elevated glucose in the development of cognitive impairment is uncertain. A prospective analysis of elevated fasting glucose levels and cognitive function in more than 8,400 older individuals 17 without a history of DM did not find a relationship between baseline elevated fasting glucose (FG) levels and executive function or memory decline on follow-up. As of this writing, there are no prospective studies that have examined whether lowering glucose levels prevents cognitive impairment or at least slows its progression. The results of the ACCORD MIND study are awaited in 2011. 18 In that study, approximately 3,000 people with type 2 DM were allocated to either intensive or standard treatment of glucose [glycosylated hemoglobin (HbA1c) 6.4% vs. 7.5%] and followed for nearly 5 years using a battery of neuropsychological tests.
Several studies have demonstrated that cognitive impairment may be present at the time of DM diagnosis or predate its appearance (reviewed in ref. 19). As an example, a study from the Netherlands 20 demonstrated reduced memory performance at the time of diabetes diagnosis [mean difference in z-scores −0.15 (95% CI −0.28, −0.03)]. These studies are consistent with the notion that factors predating the onset of elevated glucose levels may lead to the onset of cognitive impairment in people with DM. Chief among these factors is metabolic syndrome itself and its principal components of inflammation, hypertension, and insulin resistance.
With regard to metabolic syndrome itself as a risk factor for cognitive impairment, the findings are mixed. Several longitudinal reports showed that metabolic syndrome predicts cognitive impairment, 21 cognitive decline, 22,23 and vascular dementia. 24,25 On the other hand, other studies showed no deficits. 26 –28 Differences in study design, the tool(s) used to measure cognitive function, age of the people studied, duration of metabolic syndrome, differences in outcomes (cognitive decline, mild cognitive impairment, dementia), and differences in socioeconomic status may explain some of the differences between study outcomes.
As to elevated levels of inflammation as factors predisposing to cognitive decline, a study of middle-aged and elderly community-dwelling adults found that participants with metabolic syndrome did worse on tasks assessing memory and executive function than did those without metabolic syndrome 29 β coefficient −0.65 (95% CI −1.14, −0.15)]. Importantly, inflammation appeared to mediate this relationship in men, because men with metabolic syndrome and high levels of CRP had more severe cognitive dysfunction than those with metabolic syndrome and low CRP levels. A multivariate regression analysis showed that men with metabolic syndrome who had high high-sensitivity (hs)-CRP levels (i.e., >1.9 mg/L) performed significantly worse on tests of memory (β −0.44; 95% CI −0.94–0.04; P=0.074) and executive functions (β −2.21; 95% CI −3.81 to −0.62; P=0.007) than their male counterparts with low hs-CRP (memory, β −0.05; 95% CI −0.45 to 0.33; P=0.774; executive functions, β 0.48; 95% CI −0.74 to 1.7; P=0.437). The interaction between hs-CRP and metabolic syndrome was significant for executive functions (β −2.79; 95% CI −4.67 to −0.92; P=0.004) and showed a nonsignificant trend for memory (β −0.56; 95% CI −1.17 to 0.04]; P=0.068). The Longitudinal Aging Study Amsterdam 30 reported similar results (highest tertile for both CRP and α1-antichymotrypsin; β values ranging from −0.86, −1.94, P<0.05). Metabolic syndrome was negatively associated with cognition in subjects with high inflammation levels, whereas an association was absent in subjects with low levels of inflammation.
Similar cross-sectional results were reported from the Health ABC study. 23 That study demonstrated that participants with metabolic syndrome and high levels of inflammation were more likely to develop lower cognition test scores [adjusted relative risk (RR) 1.66; 95% CI 1.19, 2.32] than participants with metabolic syndrome and low levels of inflammation factors. A population study from the Mayo Clinic reported more cognitive impairment with raised CRP levels in people with metabolic syndrome. 31 The combination of metabolic syndrome and high CRP (compared to no metabolic syndrome and lowest CRP tertile) was associated with nonamnestic mild cognitive impairment [odds ratio (OR)=2.31; 95% CI 1.07, 5.00]. The Italian Longitudinal Study of Ageing 32 found that participants with metabolic syndrome had an increased risk of dementia due to vascular disease [HR 3.71 (1.40, 9.83)] as compared to those without metabolic syndrome. When results were categorized by inflammation factors, those with metabolic syndrome and high levels of inflammation had an even higher risk of vascular dementia [HR 9.55 (1.17, 78.17)], whereas those with low inflammation did not have a significant risk of dementia.
There are also studies to show that insulin resistance is a risk factor for cognitive decline in the context of metabolic syndrome. In a study of older adults (mean age 73 years), insulin resistance was significantly associated with poor visual scanning and poor cognitive flexibility. 33 Insulin resistance was an independent determinant of the Trail Making Test (β=11.005; P=0.021). In the Nurses' Health Study, 34 elevated levels of insulin (the marker of insulin resistance used in that study) were associated with faster cognitive decline as compared to lower levels during >10 years of follow up. Compared to the lowest quartile, adjusted differences in the annual rates of decline for the second, third and fourth quartiles were: Telephone interview for cognitive status (TICS) performance, −0.06 (95% CI, −0.16, 0.03), −0.14 (−0.24, −0.04), and −0.09 (−0.19, 0.01) points (P trend=0.04); verbal memory, −0.01 (−0.04, 0.02), −0.05 (−0.08, −0.02), and −0.02 (−0.05, 0.01) units (P trend=0.02). These associations remained after multivariable adjustment. A study from the Netherlands 35 of middle-aged adults showed HOMA-IR to be associated cross-sectionally with poor executive function in women (metabolic syndrome and high HOMA-IR, P=0.03 and P=0.009, respectively). In a study of women, aged 50–65 years, with intact cognitive function, there was a significant negative association between HOMA-IR and right and total hippocampal brain volume, overall cognitive performance, and selective tests of verbal and nonverbal memory. 36 Not all studies, however, find a relation between insulin resistance and cognitive impairment. A European study of middle-aged and older men did not find an association between insulin resistance and cognitive impairment. 37
Hypertension is related to cognitive decline. Much of the association is owing to its strong association with vascular disease events such as strokes and lacunar infarcts. Beyond these associations, the evidence is inconclusive. Longitudinal epidemiological studies show that elevated blood pressure and hypertension in middle age are associated with mild cognitive impairment and dementia later in life. 38,39 The association is strongest for vascular dementia and less for Alzheimer disease. Autopsy studies show more neurofibrillary tangles and brain atrophy in hypertensive individuals. 40 On the other hand, cross-sectional studies or studies with short follow-up observe associations of low blood pressure and dementia or no association of hypertension with dementia. Also the effect of antihypertensive medications on cognitive decline is uncertain.
In the CHS, people with mild cognitive impairment had a higher prevalence of hypertension. 41 In a study from New York City, 42 hypertension was associated with an increased risk for the development of mild cognitive impairment in general [HR, 1.40 (1.06, 1.77)] and for the nonamnestic form of mild cognitive impairment in particular [1.70 (1.13, 2.42)]. Hypertension was associated with the rate of change in executive ability but not in memory or language, suggesting that most of its impact was in the areas of the frontal lobes. The mechanisms for these associations were not known. The authors of that study speculated that oxidative stress, disease of the microcirculation, or exudation of proteins from the microcirculation could have played roles.
With regard to the last possibility, we have found that albuminuria, or the factor(s) that lead to albuminuria, are a risk factor for cognitive decline. Hypertension is the most common condition under which albuminuria develops. 43 Kidneys that excrete excessive amounts of albumin have many of the same microvascular features that are found in the brains of people with cognitive impairment, i.e., capillary basement membrane thickening, luminal narrowing, and leakiness. 44,45 These observations suggested to us that both conditions may share a common pathogenesis, and may share similar natural histories. In our first study, based on the CHS, 46 we found a cross-sectional association between albuminuria and the presence of cognitive impairment. In unadjusted analyses, the odds of dementia were 33% higher (OR 1.33, 95% CI, 1.22, 1.45) in the presence of albuminuria as compared to its absence (19.3% vs. 10.5%). Adjustment for cardiovascular risk factors, lipid levels, CRP, and apo-protein E-4 genotype attenuated this association, but it remained statistically significant [OR 1.16 (1.02, 1.32)]. There were no differences in the distribution of prior stroke, ankle arm index, or internal carotid artery intimal medial wall thickness between those with or without albuminuria. In a more recent analysis, 47 based on the ONTARGET and TRANSCEND studies (in which almost all participants had hypertension), we demonstrated a prospective association between the presence of albuminuria and the development of cognitive decline. Participants with baseline albuminuria were at significantly increased risk of cognitive decline compared to those with normoalbuminuria [OR 1.21 (1.07, 1.38) microalbuminuria; 1.21([0.94, 1.54) macroalbuminuria]. Participants who developed new albuminuria during follow-up also had an increased risk of cognitive decline compared to those who remained normoalbuminuric [OR 1.30; (1.12, 1.52) new microalbuminuria; 1.77 (1.24, 2.54) new macroalbuminuria]. Importantly, these associations were independent of clinical cardiovascular and renal disease and cardiovascular risk factors, which cluster with albuminuria.
How do these findings relate to metabolic syndrome? Albuminuria is a common finding in the general population as it ages. Up to ≈15%–32% of adults by age >60 years have albuminuria. 48 In an analysis of the Third National Health and Nutrition Examination Survey (NHANES III), participants with metabolic syndrome were almost twice as likely as participants without metabolic syndrome to have microalbuminuria. 49 Participants with four or five components of the metabolic syndrome were 2.5 and 3.2 times more likely to have albuminuria as compared to those with no or one component. Thus, a large percent of older adults with metabolic syndrome have albuminuria. Previously, we have shown that albuminuria, in the absence or presence of hypertension and/or diabetes, is associated with elevated levels of inflammation factors and raised SBP. 50 Both of these are principal factors of the metabolic syndrome.
There are at least two potential explanations for the relationship of albuminuria and cognitive decline. The cerebral and renal circulations are characterized by high flow and low impedance. Autoregulation of the microvasculature serves to bring blood flow to these organs, at the same time limiting excess pressure exposure in the capillaries. 51 Endothelial dysfunction and loss of microvascular autoregulation can disrupt the normal milieu within the extracellular matrix of both the brain and kidney. 52 Strain in the microcirculation can also increase the generation of reactive oxygen species (ROS). Alternatively, the exudation of proteins into the pericapillary area may lead to an inflammatory response in the brain with subsequent loss of function, much as albuminuria in the renal tubules leads to renal parenchymal inflammation. 53 Consistent with these speculations, a magnetic resonance imaging (MRI) study showed a statistically significant association between leukoaraiosis and metabolic syndrome in healthy adults. 54 A recent genome–wide association study (GWAS) of Alzheimer disease patients suggested that endocytosis—the way a cell brings in big molecules from outside—plays a role in the pathogenesis of this disease. 55
In summary, there is strong evidence for the association of metabolic syndrome with cognitive impairment. The mechanisms of association have not been clearly elucidated, but they are most likely mediated in part by elevated levels of inflammation factors and microvascular disease.
Cardiovascular Autonomic Neuropathy and Altered Circadian Rhythms
It is customary to ascribe the increased risk of cardiovascular disease that is associated with the metabolic syndrome to atherosclerosis. While this is true, another important risk factor for cardiovascular disease (CVD) in the context of metabolic syndrome is impaired cardiovascular autonomic regulation. Unlike the autonomic dysfunction that is found in association with diabetes that presents clinically as orthostatic hypotension or fixed tachycardia, the cardiovascular autonomic dysfunction found in association with metabolic syndrome is subclinical and presents as reduced heart rate variability (HRV). Diminished HRV has been shown to be an independent marker of risk for cardiovascular morbidity and mortality. 56 It is of interest that HRV has an estimated prevalence of 25%–50% 57 in adults ≥65 years of age, similar to the prevalence of metabolic syndrome in this age group. 58
We examined cardiovascular autonomic dysfunction in a subset of the CHS. 59 This subset consisted of participants who underwent 18–24 h of Holter monitoring from which markers of autonomic control of the heart were derived. In our first study, we examined the impact of fasting glucose levels on measures of HRV. We found that there were few differences in HRV measures between participants with FG levels of <100 mg/dL and those with FG levels of 100–110 mg/dL. Above 110 mg/dL, however, there were noticeable decreases in HRV. Strong differences were found in HRV indices related to circadian rhythms, including SDNN, which is the standard deviation of the intervals between normal heart beats. We also found that there were few differences in HRV measures between participants with FG levels of 110–125 mg/dL and those with diabetes (FG>125 mg/dL), suggesting that impairment of cardiac autonomic function (well known to be present in diabetes) actually begins early in the prediabetic period. These findings are similar to those from the Atherosclerosis Risk in Communities (ARIC) study 60 and the Framingham Offspring Study, 61 supporting the notion that the adverse effects of cardiac autonomic dysfunction precede the development of clinical diabetes.
Next we extended our findings. We reasoned that the majority of people with impaired fasting glucose have insulin resistance and metabolic syndrome. Among participants with FG <110 mg/dL, we found that an increasing number of components of metabolic syndrome (as defined by the Adult Treatment Panel III criteria) was associated with diminished HRV indices, including circadian measures of HRV like the SDNN. Likewise, among participants with either FG >110 mg/dL or diabetes, circadian HRV indices were more impaired among those with metabolic syndrome than among those without metabolic syndrome. Taken together, these findings suggested to us that factors associated with the metabolic syndrome played a role in the development of impaired HRV independent of FG levels.
In our next study, 62 we examined, cross-sectionally, the association of insulin resistance (as measured by HOMA-IR) and inflammation factors with HRV. The study was done in CHS participants, aged ≥65 years, with FG <100 mg/dL, to avoid the confounding effects of elevated glucose levels on autonomic function. We found strong independent associations between increased levels of interleukin-6 (IL-6), CRP, and fibrinogen, with diminished indices of HRV, including SDNN. These relationships remained robust after accounting for the presence of clinical cardiovascular disease, suggesting that cardiovascular disease did not explain these associations. We also found that HOMA-IR had a positive relationship with heart rate and a negative association with markers of HRV. These associations were somewhat attenuated upon adjustment for inflammation factors, but remained statistically significant. It was our conclusion that both insulin resistance and inflammation were associated with declines in autonomic cardiovascular function. Because our analyses were cross-sectional, we could not assess whether the autonomic impairment gave rise to the elevated inflammation factors or vice versa.
Several other studies have reported results consistent with our findings. In the ARIC Study, 63 multiple components of the metabolic syndrome were associated with low HRV. The Insulin Resistance Atherosclerosis Study 64 reported higher heart rate with lower insulin sensitivity. A small study of normoglycemic individuals also reported lower HRV in association with elevated HOMA-IR values as compared to lower values. 65 From these studies and ours, it would appear that impaired autonomic function is directly related to the presence of components of the metabolic syndrome.
Autonomic impairment in people with the metabolic syndrome is expressed as decreases in circadian measures of HRV. Autonomic activity usually shows a circadian rhythm, with a prevalence of sympathetic tone during the day and an increase in parasympathetic tone during the night and in the first hours after awakening. Heart rate variation and variability depend on the influence of sympathetic and parasympathetic activity on the sinus node and reflect spontaneous changes in autonomic activity. For example, lower SDNN values are observed in the evening hours following work and in the early morning. Clinical studies have shown that artificially interfering with circadian rhythms has adverse effects. People whose “day” is extended to 28 h, 66 under controlled conditions with dim light, develop hyperinsulinemia, fasting hyperglycemia, and elevated postprandial glucose levels. Blood pressure also rises. In children, reduced sleep duration is associated with overweight. 67 It is hypothesized that altered duration of sleep and activity disrupt the synchrony of feeding, energy storage, and periods of energy utilization. Up to 20% of genes have a 24-h rhythm pattern of expression. 68 Some of these genes are found in tissues important to metabolic processes such as fat, liver, intestinal cells, and skeletal muscle tissues. Asynchrony of gene activity expression with the availability of energy leads to altered metabolism. 69 It follows that disruption of the function of metabolic genes that are sensitive to circadian rhythms may set the stage for metabolic syndrome. Of note, altered circadian rhythms are common with aging 70,71 and shift work.
While it is generally believed that abnormal circadian rhythms lead to metabolic syndrome, it is also possible that metabolic syndrome, once established, can also impact circadian rhythms, thereby propagating itself. A case in point is sleep apnea. Visceral adiposity is a strong correlate of obstructive sleep apnea. Increased levels of IL-6 and tumor necrosis factor-α (TNF-α), produced in visceral obesity, impair circadian oscillations at the level of genes associated with circadian rhythms and promote inappropriate sleep. 71 The corollary of this finding would be that lowering inflammation levels could improve sleep apnea. In a preliminary study, 72 etanercept, a medication that neutralizes TNF-α, was given to 8 obese male participants with sleep apnea. There was a significant and marked decrease in sleepiness by etanercept, and a decrease in the number of apneas/hypopneas per hour.
Asynchronous circadian rhythms can also impact vascular reactivity and the production of fibrinolytic factors, which are present in the metabolic syndrome. A discussion of these matters is beyond the scope of this review article and can be found elsewhere. 73,74
In summary, impaired cardiovascular autonomic nervous control is found in the metabolic syndrome. We and others have shown that such impairment has an independent effect on CVD morbidity and mortality. 75,76 With greater awareness of this association, more attention to prevention and treatment may be forthcoming in the future.
Osteroporosis
Among the factors associated with the development of osteoporosis and osteoporotic fractures are: increasing age; loss of estrogen in women or testosterone in men; chronic medical conditions such as liver, lung and kidney disease; increased levels of inflammation factors; and metabolic disorders of vitamin D, calcium, and glucose. Some of these factors are present in the metabolic syndrome.
Whether the metabolic syndrome is associated with osteoporosis and osteoporotic fractures is not certain. Population studies have provided conflicting results, with some demonstrating a protective effect on bone health, whereas others show a detrimental effect. This conundrum is most likely due to the competing effects of concomitant obesity that increases mechanical loading on bone, and the proinflammatory effect of visceral adiposity that decreases bone health. Both these conditions are characteristics of the metabolic syndrome.
In an analysis of the NHANES III data set (a representative sample of the U.S. population), people with metabolic syndrome had higher bone density in the femoral neck than people without metabolic syndrome. 77 This association was believed to be due to increased abdominal obesity and indices of insulin resistance. In that study, the higher the number of metabolic syndrome components, the greater was the bone density in the femoral neck. There was a trend for lower bone density in men with high CRP levels. In contrast, the Rancho Bernardo Study 78 (a study of predominantly white, middle class, older adults) found decreased bone density in people with metabolic syndrome when adjustment was made for body mass index (BMI). There were also more incident fractures in the metabolic syndrome group. There were statistically significant negative associations between the number of metabolic syndrome components with hip and spine density. In a third study, from the Veterans Administration, 79 men with metabolic syndrome and no diabetes had lower bone density than nondiabetic men without metabolic syndrome. Other conflicting results have also been reported. 80 –82 Thus, at this point, no firm conclusions can be reached regarding the association of metabolic syndrome and bone health.
Aging, Adiposity, and Metabolic Syndrome
The strongest causative factor for the development of metabolic syndrome is visceral adiposity. Aging is associated with increases in total body and visceral fat. Concurrently, there is loss of lean body mass (sarcopenia). Thus, even if a person maintains stable weight or BMI, the percentage of body fat increases with age. Strongly related with increased visceral fat is increased liver fat, due in part to the direct access of visceral fat and free fatty acids to the portal circulation. Increased liver fat results in reduced insulin clearance, hyperinsulinemia, and increased gluconeogenesis.
Given these facts, it is reasonable to ask whether the nonatherosclerostic complications of metabolic syndrome described here are due to the aging process per se or are more strongly related to adiposity. We believe that the latter explanation is more correct. While aging is associated with metabolic defects and increased oxidative stress, the insulin resistance and increased inflammation levels of metabolic syndrome are modifiable. For example, the Diabetes Prevention Program (DPP) 83 aimed at discovering whether modest weight loss through dietary changes and increased physical activity or treatment with metformin could prevent or delay the onset of type 2 DM. At the beginning of the DPP, participants were all overweight and had impaired glucose levels, consistent with insulin resistance. Those participants receiving intensive individual counseling and motivational support on effective diet, exercise, and behavior modification reduced their risk of developing diabetes by 58%. This finding was true across all participating ethnic groups and for both men and women. Lifestyle changes worked particularly well for participants aged 60 and older (the prime age for metabolic syndrome), reducing their risk by 71%. Were the effects of metabolic syndrome related to aging per se, one would not expect decreases in insulin resistance with lifestyle change.
Telomere biology is consistent with this notion. Telomeres are the DNA caps on the ends of chromosomes that prevent aberration or loss of genetic information during cell division. Longer telomeres correlate with longevity and reduced disease burden. 84 In a study of obese individuals who lost weight, telomere length increased. 85 Were metabolic syndrome related to age per se, one would not expect telomere length to increase with change in lifestyle. Thus, addressing metabolic syndrome through lifestyle modification holds out the possibility of slowing down or ameliorating the aging process itself.
Summary
In this review we have highlighted several chronic, age-related conditions that are associated with the metabolic syndrome. It may be that the presence of the metabolic syndrome “accelerates” the aging process or is a manifestation of processes related to aging. Put differently, visceral adiposity with its increased production of inflammation factors and increased insulin resistance impacts the body as a whole, beyond the cardiovascular system. With this knowledge in mind, it may be possible to encourage people, individually and as a society, to improve their lifestyle so as to forestall the negative effects of the metabolic syndrome on health. To date, lifestyle changes alone (e.g., exercise, weight loss) have been shown to impact metabolic syndrome. This is similar to other age-related disorders, such as CVD, stroke, and DM, that can be largely prevented or delayed by lifestyle intervention. A recent study 86 has demonstrated that blocking inflammation at the cellular level, through the use of medications, may decrease insulin resistance in people with DM, most of whom had metabolic syndrome. This finding holds out the promise that medications that modify the underlying factors in metabolic syndrome may also result in improved health.
Footnotes
Author Disclosure Statement
No competing financial interests exist.