
Abstract
Background:
The aim of this study was to assess prevalence of metabolic syndrome and its components according to different criteria in the population of bank employees in St. Petersburg, Russia.
Methods:
A total of 1,600 office workers were screened at their working places from the Sberbank state bank in St. Petersburg. All subjects were interviewed by a special questionnaire that included personal data, smoking status, physical activity, alcohol consumption, and medical history. Anthropometry measurements, vital signs, and fasting blood samples were obtained. Serum lipids and plasma glucose were measured.
Results:
In all, 1,561 responders were included in the final analysis. Hypertension (HTN) was observed in 35.2% of subjects (64% in males and 25.4% in females), abdominal obesity (AO) according to Internation Diabetes Federation (IDF) criteria in 45.6% (51.5% in males and 44.0% in females), high triglyceride levels in 28.4%, low high-density lipoprotein cholesterol (HDL-C) levels in 23.9%, and elevated fasting glucose over 5.6 mmol/L in 28.4% of subjects. AO associated with HTN was observed in 24.3%. Metabolic syndrome according to IDF criteria was diagnosed in 21.5% (17.9% in females and 34.6% in males, P<0.01), and according to Adult Treatment Panel III (ATP III) (2005) criteria in 18.8% of subjects (16.2% in females and 28.4% in males, P<0.01). The correlation between criteria was ρS=0.79. Low physical activity, smoking, and alcohol abuse were associated with metabolic syndrome.
Conclusions:
Metabolic syndrome and its distinct components were very prevalent in Russian bank office workers. AO was most prevalent component for females with metabolic syndrome, whereas HTN was most prevalent for males. Coexistence of HTN and AO was the most frequent coupling of metabolic syndrome components. Unhealthy lifestyle characterized the selected group and was associated with metabolic syndrome, especially low physical activity.
Introduction
However, the prognostic value of metabolic syndrome and its distinct components has not been determined in all populations, and the prevalence of metabolic syndrome is underestimated in many regions. The data obtained indicate that several metabolic syndrome criteria can be more sensitive in one population and less sensitive in the other. For example, International Diabetes Federation (IDF) criteria 4 appear to verify more metabolic syndrome patients in Germany whereas the Adult Treatment Panel III (ATP III) (2005) 4 verifies more patients in the United States. 6 Concordance of different criteria also varies between studies from 50% to 90%. 7 –9 In this context, any epidemiology data concerning other populations can be very informative and useful for ruling out further ethnic-specific criteria of the syndrome and its general interpretation. Socioeconomic status and occupation contribute to the occurrence of cardiovascular risk factors, as well as metabolic syndrome. 10,11 Highly educated subjects can demonstrate lower prevalence of obesity and better compliance with a healthy lifestyle, 12 whereas mental work is usually associated with low physical activity and, thus, can predispose to metabolic syndrome.
The aim of the present study was to assess the prevalence of different components of metabolic syndrome and the syndrome as a whole entity according to different criteria in a population of bank employees in St. Petersburg, Russia. This sample was chosen because of two circumstances—a predominantly sedentary lifestyle and, therefore, possible high prevalence of metabolic risk factors, as well as high educational level and expected good compliance with screening procedures.
Methods
A total of 1,600 office workers were screened at their working places in five central bank offices of the Sberbank state bank in St. Petersburg. The response rate was 86% from all employees in the selected offices. All screening procedures were performed in June to August of 2008. The signed informed consent was obtained from all participants. The study was approved by the Institutional Review Board (IRB) on cardiology and endocrinology from the Almazov Federal Heart, Blood, end Endocrinology Centre.
All subjects were interviewed by trained personnel with a special questionnaire that included personal data, information about heredity, smoking status, physical activity, alcohol consumption, medical history, including known cardiovascular risk factors, and current medication. Personal data included birth date, marital status, education, income, and occupation. Data were collected by trained physicians and nurses (body weight, height, blood sampling).
Anthropometry, vital signs, and fasting blood samples were obtained in the morning between 9.00 a.m. and 11.00 a.m. Standard procedure for the measurement of blood pressure was used. Three blood pressure measurements were taken by trained personnel on the right arm of each participant, who had been seated prior to measurement. Standard mercury sphygmomanometers were used with appropriate cuff sizes. Systolic blood pressure (SBP) was measured at the first appearance of a pulse sound (Korotkoff phase 1) and diastolic blood pressure (DBP) at the disappearance of the pulse sound (Korotkoff phase 5). The mean value of the second and third measurements was calculated. Heart rate (HR) was calculated according to radial pulse after the last blood pressure measurement by 30 sec and multiplied by 2. Height was measured in centimeters while the participant stood without shoes, and weight was measured in kilograms without shoes and in light clothing. Body mass index (BMI) was calculated as weight in kilograms over height in meters squared. Waist circumference (WC) was measured in centimeters at the midpoint between the bottom of the ribs and the top of the iliac crest. Hip circumference (HC) was measured at the largest posterior extension of the buttocks.
Serum lipids and plasma glucoses were measured by Hitachi-902 equipment with Roche Diagnostics kits. Serum triglyceride level and high-density lipoprotein cholesterol (HDL-C) were measured directly.
Definition of metabolic syndrome
Individuals with metabolic syndrome were defined according to 2009 Harmonizing Definition of the Metabolic Syndrome 1 as specified in Table 1.
Because no population and country-specific cut points are available, the IDF criteria were chosen.
WC, waist circumference; HDL-C, high-density lipoprotein cholesterol; IDF, International Diabetes Federation.
Statistics
The statistical package Statistica 6.0 (StatSoft, USA) was used for statistical analysis. To check the correctness of data entry and exposure of possible data heterogeneity, principal component analysis and cluster analysis were applied. The chi-squared statistics were calculated to compare distribution of qualitative variables. Differences for continuous variables among the subgroups were compared with one-way analysis of variance (ANOVA) if the data were approximately normally distributed. A data logarithm was applied when appropriate. Multiple pairwise comparisons were made with a post hoc Scheffè test, with the overall alpha level set at 0.05. Relationships between continuous variables were assessed with the Pearson correlation coefficient; relationships between categorical variables were assessed with a chi-squared test of association. All tests were two-sided and carried out to a significance level (P) of 0.05. In case of multiple parallel comparisons, the P value was reduced to 0.005.
Results
Characteristics of the studied group
During data entry, 36 questionnaires were not included in the analysis because of the lack of important data concerning metabolic syndrome or more than five items of the questionnaire missing. Three serum specimens were not applicable for lipid measurements. Finally, 1,561 responders were included in the database. Characteristics of the studied population are presented in Table 2. Females were highly predominant in the selected population, which is typical for professions performing mental work in Russia.
BMI, body mass index; WC, waist circumference; W/H, waist-to-hip ratio; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; BP, blood pressure.
Prevalence of the selected components of metabolic syndrome
Hypertension
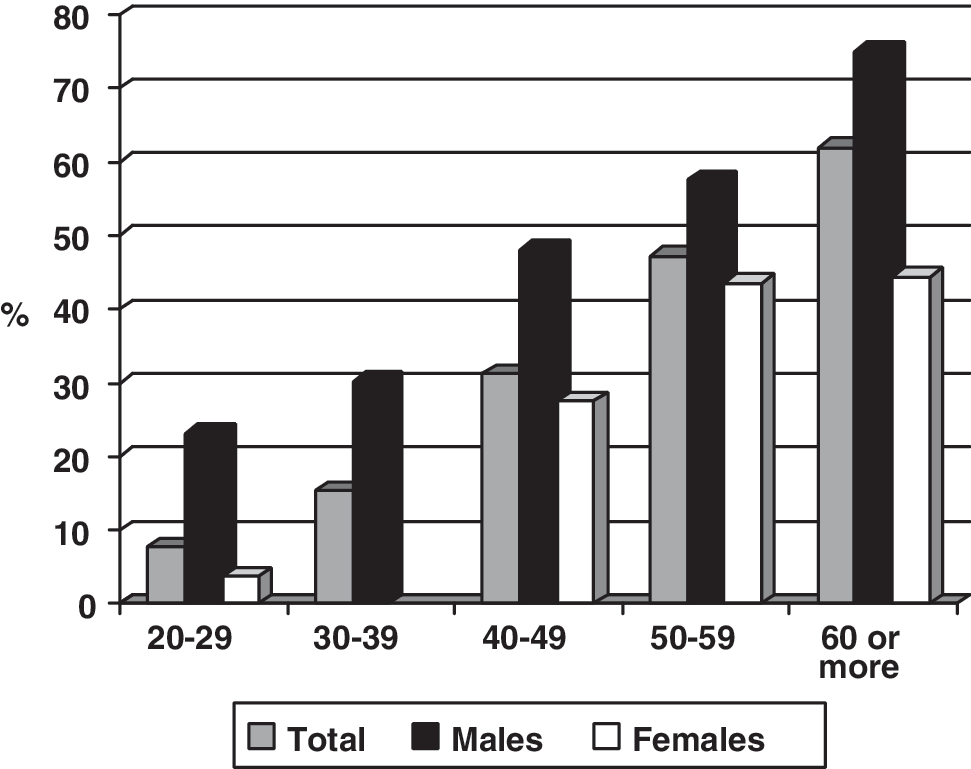
Hypertension (HTN) was diagnosed according to blood pressure elevation over threshold level according to metabolic syndrome criteria or use of regular antihypertensive medication (see Table 2). The latter criterion was applicable to only 29 subjects (1.9%). Other subjects on antihypertensive medication did not have goal blood pressure levels and were considered hypertensive according to blood pressure data. The prevalence of elevated blood pressure was high in the studied population, especially in males, possibly due to regular mental stress. The HTN awareness was extremely high (more than 80%), which can be explained by high educational level. The optimal blood pressure according to European Society of Cardiology (ESC) 2007 13 was observed only in 620 subjects (43%), and normal blood pressure was considered in an additional 401 subjects (27.7%). The prevalence of HT increased with age from 9.9% in age group 20–29 years to 64.6% in subjects 50–59 years old (Fig. 1). In patients older than 60 years, 76.2% were hypertensive, mostly according to isolated systolic HTN.

Prevalence of blood pressure elevation ≥130/85 mmHg according to age.
Obesity
In Table 2, the prevalence of obesity defined by different diagnostic criteria is also presented. The number of subjects in whom abdominal obesity (AO) could be diagnosed only by WC measurement with normal a BMI was 103 (6.6%). Alternatively, in patients with a BMI over 30 kg/m2, normal WC was observed in 96 (6.2%) cases. The highest prevalence of AO was estimated according to strict WC criteria (female/male over 80/94 cm, respectively) (45.6%). It is worth mentioning that in subjects with WC from 94 to 102 cm in males and from 80 to 88 cm in females (n=316) obesity according to BMI level was verified only in 14.7%. One can see also that lower cutoff points increase prevalence of AO in males, whereas according to the NCEP definition the prevalence of AO was equal in both sexes. It was also documented that change in cutoff points for WC increases the number of patients at risk at a younger age more that two times, which can be interpreted as an early detection of subjects at risk, where intervention can be needed, at least for lifestyle changes.
Biochemistry
Diabetes mellitus was diagnosed in cases of fasting glucose levels greater than 7.0 mmol/L, confirmed by repeated test in all cases. In all, 39 cases of newly diagnosed type 2 diabetes were registered among 47 (3%) diabetic patients. Fasting plasma glucose greater than 5.6 mmol/L was observed in 443 (28.4%) of participants—142 (42.0%) males and 301 (24.6%) females (P<0.001). The prevalence of elevated glucose level and diabetes also increased with age (data not shown).
Increased triglyceride levels more than 1.7 mmol/L were documented in 242 (15.5%) subjects—88 (26.0%) males and 154 (12.6%) females (P<0.0001). The HDL level was lower—1.3 mmol/L in 302 (24.3%) females and 1.0 in 77 (22.8%) males (P=0.57). The total prevalence of this metabolic syndrome component was 23.9%. High triglyceride and low HDL levels were also associated with age (data not shown).
Thus, in the studied population, the most prevalent component of metabolic syndrome was AO. The second place could be given to HTN, followed by hyperglycemia and high TG level. The proportion of subjects having at least one metabolic syndrome component was 69.2%.
The frequency of different combinations of metabolic syndrome criteria
In Table 3 the frequency of coupled metabolic syndrome criteria is presented. The more prevalent co-morbidities were obesity associated with HTN (24.3%).
AO, abdominal obesity; HTN, hypertension; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides.
Figures 3 and 4 illustrate the prevalence of different numbers of metabolic syndrome criteria in the studied group. Interestingly, in males, the number of subjects with one, two, or three components was similar, whereas in females it decreased progressively. The coexistence of multiple (more than three) risk factors was rare in females and relatively frequent in males. Because HTN was more common for males in the selected group and HTN and obesity were the most frequent metabolic syndrome factors, this can be a confounder (see Table 4).
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides.
The prevalence of metabolic syndrome was 23.3% (336 subjects) (39.4% in males vs. 19.1% in females, P<0.0001). If the WC cutoff for 102/88 cm was applied, the prevalence was 18.6% (291 subjects) (28.4% in males vs. 15.9% in females, P<0.0001) respectively. The syndrome was more prevalent in males.
The metabolic syndrome in subjects with AO was 11.6 times higher that in lean patients (46.6% vs. 4%). Similarly, in hypertensive subjects, the metabolic syndrome was 8.7 times higher that in normotensive (57.2% vs. 6,6%).
Figure 2 shows the age-dependence prevalence of the syndrome according to different criteria. The prevalence of the syndrome increases with age but was high in the studied population, especially in young ages.
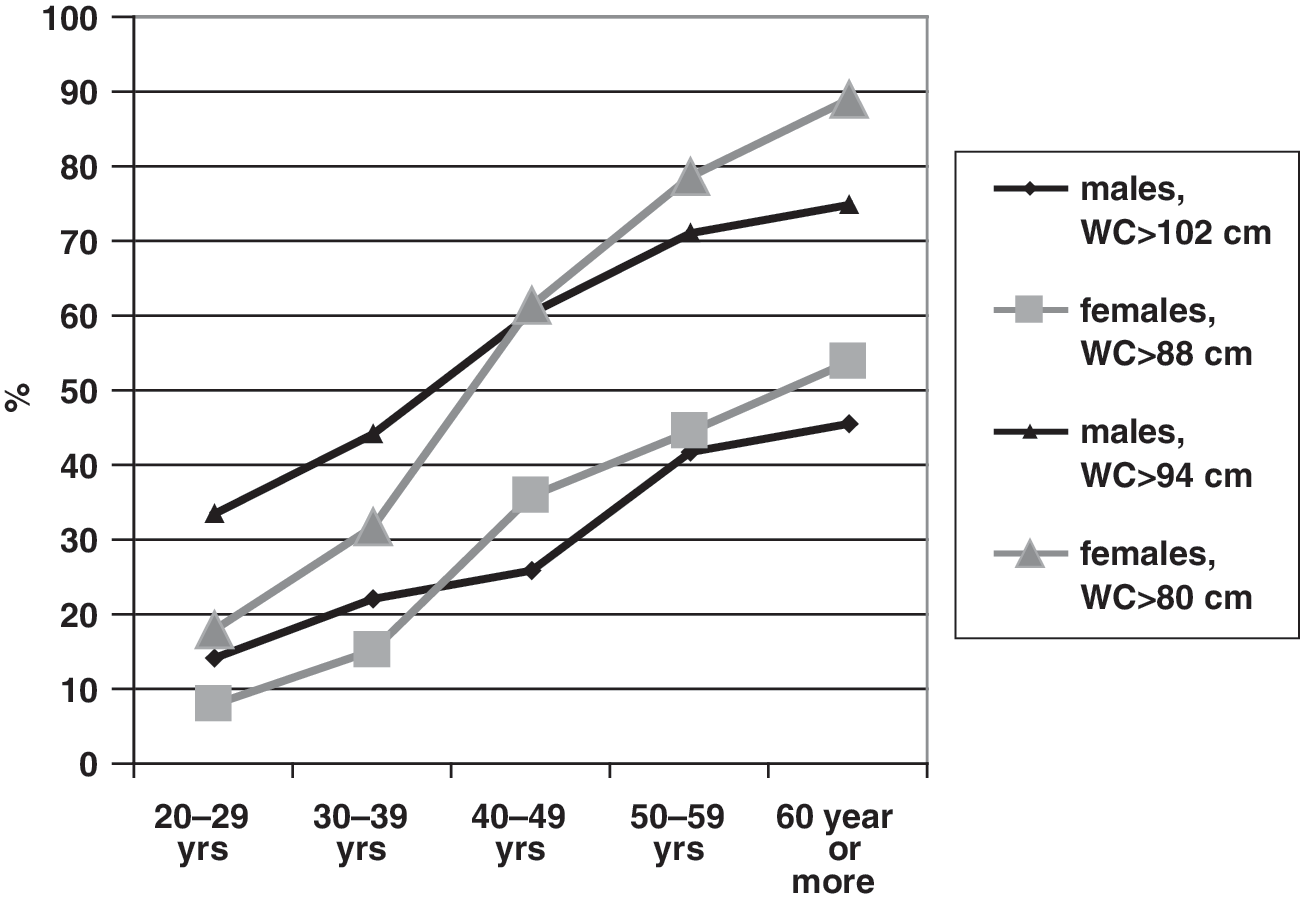
Prevalence of abdominal obesity diagnosed by different cut points for waist circumference according to age and gender (%). WC, Waist circumference.

The frequency of different numbers of metabolic syndrome components.
Prevalence of metabolic syndrome in different age groups.
The absolute values of separate metabolic syndrome components showed a significant correlation with each other. The highest correlation was observed between WC and BP (r=0.51 for SBP, P<0.001 and r=0.52 for DBP, P<0.001). WC also correlated with TG level (r=0.37, P<0,001). TG level negatively correlated with HDL-C (r=−0.26, P<0.001).
Lifestyle factors and metabolic syndrome
Metabolic syndrome according was diagnosed in 96 smoking subjects (22%), 53 ex-smokers (21.8%), and 14.1% nonsmoking subjects (P=0.0003). According to the questionnaires, in 15.7% of subjects the alcohol consumption could be classified as moderate/severe. The prevalence of metabolic syndrome was higher in drinkers (20.3%) compared to nondrinking responders (13.2%), P=0.003. According to physical activity, all subjects were classified in three groups: Having sedentary lifestyle (829 subjects), moderate physical exercise less than three times per week (386 subjects), and exercising regularly (346 subjects) (more that three times per week). The prevalence of metabolic syndrome was 21.4%; 16.1%, and 10.1%, respectively (P=0.00002), indicating strong association of this factor with metabolic syndrome. This association was confirmed for both genders.
Discussion
Any comparison of metabolic syndrome prevalence can be done only in relation to population features and criteria used. We calculated the prevalence of metabolic syndrome according to the 2009 Harmonizing definition, but, as the prognostic value of WC in Russia has been never studied before, we assessed both cutoff points for WC (applied to a European population) to observe the discrepancies compared to other populations.
The present study indicates that metabolic syndrome is highly prevalent in bank employees working in St. Petersburg. This occupational group has not been studied in detail previously. Differences in the prevalence of cardiovascular disease and its risk factors among occupational groups have been found in several studies, including metabolic syndrome prevalence. 17,18 In a Spanish study among female subjects, the age-adjusted prevalence of metabolic syndrome was higher in blue-collar than in white-collar workers, but not in males. 12 Alternatively, in our study, the metabolic syndrome was more prevalent in males that in females, mainly due to higher prevalence of HTN in males. In a majority of European populations, metabolic syndrome was more frequent in males, 10,14 –16 whereas in Asian studies females appear to be the leaders. 7,8 But recently it was observed that the prevalence of metabolic syndrome among Thai professional and office workers was 15.2% and approximately three times more common among men than women (25.8% vs. 8.2%). 18 The general metabolic syndrome prevalence in our population was comparable to adult populations of France, 10 Italy, 16 and Finland. 19 When compared to age-dependent prevalence in the United States, 11 the studied population had higher metabolic syndrome prevalence by 10% in the third and forth decades. This can be explained by very high prevalence of AO, especially by IDF criteria, in the selected group. This risk factor can be occupation related and explained by a sedentary lifestyle. Another example of professional involvement can be HTN, which was observed in two-thirds of males. The bank employees under investigation have very high level of professional stress, which can to some extent be related to blood pressure elevation. In 1997 Helmert et al. 17 showed that certain aspects of the workplace and its culture, particularly in blue-collar occupations, influence the cardiovascular risk to a greater extent in men than in women. The white-coat phenomenon, especially in males, also cannot be excluded as the reason of high blood pressure levels during screening procedures. On the other hand, the screening protocol and blood pressure measurements were standardized and did not differ from those used in other studies. In a Turkish population, metabolic syndrome was significantly more prevalent among workers who had high strain in their jobs. 20 In the present study, the level of job strain was not assessed but can be supposed to be rather high.
In the studied group, the prevalence of obesity was high, and IDF criteria appear to be more sensitive for metabolic syndrome. But many subjects included in the group with metabolic syndrome according to IDF had very modest changes in blood pressure, lipids, and glucose and a mild increase in WC. At the same time, a lot of subjects with higher blood pressure and severe dyslipidemia were not included in the syndrome by IDF definition because they were lean. According to other published studies, about 7% of metabolic syndrome (ATP III) subjects have no obesity. 6 In our study, the proportion of such subjects was even higher (11.2%). This indicates that approximately every ninth subject with three components of metabolic syndrome according to ATP III will be “lost” from the high-risk group in cases of implementation of the IDF definition.
One of the limitations of our study was self-confirmation of fasting status. This can compromise the data regarding the glucose level, because the estimated prevalence of high plasma glucose was higher than in other populations. On the contrary, hypertriglyceridemia was observed in the same proportion of subjects as in other comparable groups. 15,20
Recently, studies performed in different populations were compared according to metabolic syndrome prevalence [Dallas Health Study, National Health and Nutrition Examination Survey (NHANES), and Prospective Cardiovascular Munster study (Germany)]. 6 It was shown that according to ATP III versus IDF, the metabolic syndrome is more prevalent in the United States both in males (30% vs. 25%), and females (37% vs. 18%). Alternatively, when IDF 2005 criteria were applied, the prevalence of metabolic syndrome became higher in Germany. The agreement of both criteria in the U.S. population was 90%, whereas in Germany it was only 80%. In our study, the total agreement of criteria was 93%, higher than in both mentioned populations. The data obtained again indicate that the frequency and impact of different components of metabolic syndrome can vary significantly in different populations.
Lifestyle factors were also assessed in this study and showed a strong association with metabolic syndrome, especially physical activity and smoking. 21 According to recent data, smoking is associated with low HDL in the French population. 9 Other studies have shown no association between smoking and insulin resistance. 22 The relation of smoking status with metabolic syndrome in our study can be challenged by the high prevalence of smoking in this specific population combined with additional lifestyle factors. In the single study performed in Russia, moderate frequency of alcohol consumption and binge drinking in men and higher leisure time physical activity in women were inversely associated with metabolic syndrome. 23 We observed an association with low physical exercise in both genders.
In conclusion, metabolic syndrome and its distinct components were very prevalent in a Russian population whose occupation was bank office workers. Obesity was most prevalent for females, whereas HTN was for males. Coexistence of AO and HTN was the most prevalent coupling of metabolic syndrome components. Unhealthy lifestyle was very typical for the selected group and was associated with metabolic syndrome, especially low physical activity.
Footnotes
Acknowledgments
This study was supported by state contract no. 06/303 from 30.05.2008 of the Ministry of Science and Education of Russian Federation (Program “Prevention of socially important diseases” (2007–2011), section “Diabetes Mellitus.”
Author Disclosure Statement
The authors have no conflicts of interest to declare.