
Abstract
Background:
Metabolic syndrome is a frequent condition that has been linked to cardiovascular disease (CVD) and mortality. Metabolic syndrome has been extensively shown to increase the risk of chronic nephropathies in Americans and Asians, but not in European populations. Renal disease increases the risk of CVD and mortality. However, the chronic nephropathy–CVD liaison has not been analyzed in the framework of the possible role of metabolic syndrome in both.
Methods:
We analyzed data from 3,757 subjects participating in the INCIPE survey (Initiative on Nephropathy, of relevance to public health, which is Chronic, possibly in its Initial stages, and carries a Potential risk of major clinical End-points), a cross-sectional study enrolling subjects from the general population in the Veneto region in Italy, and calculated the odds ratio (OR) and 95% confidence interval (CI) of the association between metabolic syndrome, and/or chronic kidney disease (CKD) and albuminuria, and/or previous CVD after adjustment for confounding factors.
Results:
Metabolic syndrome is associated with CKD (OR 2.17; P<0.001) and albuminuria (OR 2.28; P<0.001) and CVD (OR 1.58; P=0.002). There is a direct correlation between number of metabolic syndrome traits and nephropathy and CVD. CVD and nephropathies are associated even after adjustment for metabolic syndrome (OR 2.30; P<0.001).
Conclusions:
In a homogeneous Caucasian European population, metabolic syndrome is associated with CKD and albuminuria, and CVD. Although metabolic syndrome is a risk factor for both CVD and nephropathy, it does not entirely explain the dangerous CVD–nephropathy liaison.
Introduction
Chronic kidney disease (CKD), a public health problem, 3 is a recognized risk factor for cardiovascular mortality. 4 The cause/s for such an association is/are partly known. Besides traditional cardiovascular disease (CVD) risk factors, nontraditional CVD risk factors have been recognized in patients with CKD, 5 many of which play a role in the more advanced stages of CKD. However, although metabolic syndrome is a known CVD risk condition and has been associated with the risk of developing CKD as well, 6 –11 its possible role in explaining the CKD–CVD liaison has not been investigated.
The increased risk of CKD and/or proteinuria in subjects with metabolic syndrome has been shown in different populations and ethnic groups. Hoehner et al. reported an odds ratio (OR) of albuminuria associated with three or more traits of metabolic syndrome of 2.3 in a survey on 934 nondiabetic Native Americans. 12 Chen et al. analyzed U.S. data from the National Health and Nutrition Examination Survey (NHANES III) database confirming the same conclusions. 6 Similar associations have been also reported in Asian populations. 7 –9 To the best of our knowledge, the issue has been investigated in European populations in only two reports, with inconsistent results. 13,14
We studied the association between metabolic syndrome and renal disease (CKD and albuminuria) and history of CVD events in a randomly selected northern Italian adult population participating in the INCIPE (Initiative on Nephropathy, of relevance to public health, which is Chronic, possibly in its Initial stages, and carries a Potential risk of major clinical End-points) study. We also investigated the renal disease–CVD liaison in the framework of the possible role of metabolic syndrome in both. Results are reported here.
Methods
The INCIPE study
The INCIPE study design has been described elsewhere. 15 Briefly, 6,200 subjects, all Caucasians, ≥40 years old by January 1, 2006, were randomly chosen from the lists of patients of 62 general practitioners based in four geographical areas in the Veneto Region, northeastern Italy. Pregnant women were not enrolled. After obtaining written informed consent, each participant completed a self-administered questionnaire (family and personal medical history, pharmacological treatments, smoking habits). Subjects were asked to refrain from smoking from the night before. Blood pressure, waist and hip circumferences, body weight, and height were measured. Freshly voided morning urine was collected. Blood and urine samples were frozen at −80°C by 5 h after collection. With reference to the urine albumin assay, samples were prescreened with a strip test (Clinitek Microalbumin, Siemens Medical Solutions Diagnostics, Mishawaka, IN). Positive results (≥3.4 mg/mmol creatinine) were confirmed by measuring albumin immunochemically (Immage 800, Beckman Coulter, Inc Fullerton, CA) and creatinine with a kinetic-rate Jaffe method on Dimension RxL Max Integrated Chemistry System (Dade-Behring, Inc., Newark, DE). For the estimated glomerular filtration rate (eGFR), creatinine measurements were recalibrated to standardized creatinine measurements obtained at the Cleveland Clinic Research Laboratory as described. 16 The GFR was estimated with the Chronic Kidney Disease Epidemiology Collaboration (CKD EPI) equation using calibrated creatinine. 17
Serum triglycerides and glucose were determined by standard enzymatic methods and serum high-density lipoprotein cholesterol (HDL-C) by a homogeneous method. All biochemical tests were performed on the Dimension RxL Max system.
Definitions
Metabolic syndrome was defined by the presence of at least three of the following five criteria, according to the modified criteria of the Third Adults Treatment Panel (modified ATP III) of the National Cholesterol Education Program (NCEP) 18 : Waist circumference ≥102 cm in men and ≥88 cm in women, fasting plasma triglycerides ≥1.7 mmol/L, fasting HDL-C ≤1.03 mmol/L in men and ≤1.29 mmol/L in women, history of high blood pressure (HBP) or active antihypertensive drug treatment, fasting plasma glucose ≥5.6 mmol/L, or diabetes or active drug treatment of diabetes.
For sensitivity analyses, the metabolic syndrome definition followed the International Diabetes Federation (IDF) criteria of central obesity (waist circumference ≥94 cm in men and ≥80 cm in women) plus any two of the other four criteria, which are identical to those provided by the NCEP ATP III. 19
CVD was defined by self-reported history of angina, coronary heart disease, myocardial infarction, stroke, or transient ischemic attack. Diabetes was defined by self-reported diagnosis or fasting plasma glucose ≥7.0 mmol/L. CKD was defined by a GFR below the age- and gender-specific 5th percentile. According to the analysis of the INCIPE data, the percentiles for 40–49, 50–59, 60–69, 70–79, and ≥80 years were 76.3, 69.1, 61.2, 43.8, and 40.1 mL/min, respectively, in men and 73.0, 65.3, 60.2, 46.7, and 37.5 mL/min, in women. 15 This more conservative CKD definition was chosen to better identify a true CKD condition. 20 Albuminuria was defined by an albumin-to-creatinine ratio (ACR) ≥3.4 mg/mmol.
Statistical analysis
Continuous variables were expressed as mean±standard deviation (SD) and categorical variables as percent proportion. Differences between groups for continuous and categorical variables were analyzed by t-test or analysis of variance (ANOVA) and chi-squared test, respectively. The Pearson correlation coefficient was used to analyze correlations between continuous variables. The prevalence of CKD and albuminuria was determined for participants with and without metabolic syndrome and with and without each of the five components of metabolic syndrome. Prevalences of CKD and albuminuria were also calculated by the number of metabolic syndrome components present. Logistic regression analysis was used to determine the statistical significance of the differences in prevalence; the crude, age- and gender-adjusted, and multivariate-adjusted OR with 95% CI were reported. The multivariate model included age, gender, smoking status, and presence of CVD. Because only 68 subjects (1.8%) had five metabolic syndrome components, participants with four or five components were pooled in a single category to obtain more stable estimates of the OR associated with the number of components.
To test whether metabolic syndrome components have a synergic effect on the prevalence of CKD, albuminuria, and CVD, interaction terms for metabolic syndrome components were included in the logistic model. Significant interaction terms were quantified calculating the Rothman synergy index (S) following the theory of departure from the additive model. 21 A value of S greater than 1 indicates a synergic biological interaction.
The presence of potential clusters of components in subjects with metabolic syndrome and either CKD, albuminuria, or CVD was carried out by hierarchical clustering. Furthermore, each cluster was tested in logistic regression to determine its association with the outcomes.
Sensitivity analyses were carried out by using the IDF definition of metabolic syndrome to extend the generalizability of the findings. Furthermore, because the NCEP definition of metabolic syndrome does not exclude subjects with diabetes mellitus, the multivariate analysis was repeated after removal of diabetics to rule out the effect of established diabetes mellitus on kidney function, i.e., diabetic nephropathy cases.
The performance of several markers of obesity in predicting CKD and albuminuria was analyzed by receiver operating characteristic (ROC) curves and the respective area under the ROC (AUROC).
Results
A total of 3,757 subjects had data available for the analysis. Table 1 presents the general characteristics of the study participants by metabolic syndrome status. Overall, 22.4% of the study participants had metabolic syndrome; 997 subjects (26.5%) had one metbolic syndrome component, 873 (23.2%) had two components, 573 (15.3%) had three components, and 268 (7.1%) had four or five components.
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; GFR, glomerular filtration rate; CKD, chronic kidney disease.
Association between metabolic syndrome, CKD, and albuminuria
Table 2 reports the proportion of participants with CKD and albuminuria among those with and without each component of the metabolic syndrome. Each component was significantly more prevalent in subjects with CKD and with albuminuria, with the exception of waist circumference, which was more prevalent only in subjects with albuminuria. Figure 1 shows the prevalence of CKD and albuminuria by number of components of the metabolic syndrome. The prevalence of both CKD and albuminuria increased with the number of metabolic syndrome components (P<0.001 for all comparisons).

Prevalence of CKD and albuminuria by number of the metaoblic syndrome components. CKD, chronic kidney disease.
CKD, chronic kidney disease; HDL-C, high-density lipoprotein cholesterol.
Tables 3 and 4 show the OR of CKD and albuminuria associated with presence of metabolic syndrome, individual components of metabolic syndrome, and number of metabolic syndrome components after adjustment for different confounders. The ORs of CKD and albuminuria were significantly higher for participants with metabolic syndrome; subjects with any component of metabolic syndrome had an increased OR of CKD, except for the waist circumference criterion. Compared with subjects with no metabolic syndrome components, the OR of CKD and albuminuria increased for each increase in the number of metabolic syndrome components.
Multivariate model 1 is adjusted for age and gender; multivariate model 2 is adjusted for age, gender, body mass index, smoking status, cardiovascular disease
CKD, chronic kidney disease; OR, odds ratio; CI, confidence interval; HDL-C, high-density lipoprotein cholesterol.
Multivariate model 1 is adjusted for age and gender; multivariate model 2 is adjusted for age, gender, body mass index, smoking status, cardiovascular disease
OR, odds ratio; CI, confidence interval; HDL-C, high-density lipoprotein cholesterol.
Association between metabolic syndrome, CKD, and CVD
The OR of CVD associated with metabolic syndrome was 1.58 (95% CI 1.18, 2.12; P=0.002) after adjustment for age, gender, smoking status, and nephropathy. Compared with subjects with neither metabolic syndrome nor nephropathy (defined as the presence of CKD, albuminuria or both), the age, gender, and smoke-adjusted OR of CVD for subjects with metabolic syndrome but not nephropathy was 1.42 (95% CI 1.03, 1.94; P=0.031); for subjects with nephropathy but not metabolic syndrome, the OR was 1.70 (95% CI 1.10, 2.61; P=0.017); for subjects with both metabolic syndrome and nephropathy, the OR was 3.34 (95% CI 2.19, 5.11; P<0.001). The OR of CKD associated with the presence of CVD was 2.30 (95% CI 1.34, 3.96; P<0.001) after adjustment for metabolic syndrome.
Table 5 shows the OR of CVD associated with presence of metabolic syndrome and individual components of metabolic syndrome and number of metabolic syndrome components. Considering the number of metabolic syndrome components as a continuous variable, each trait was associated with an OR for CVD of 1.47 (95% CI 1.32, 1.63; P<0.001).
Multivariate model 1 is adjusted for age and gender; multivariate model 2 is adjusted for age, gender, body mass index, smoking status, and nephropathy (CKD and/or albuminuria).
CVD, cardiovascular disease; OR, odds ratio; CI, confidence interval; HDL-C, high-density lipoprotein cholesterol.
Sensitivity analyses
The main findings were substantially unchanged upon using the IDF definition of metabolic syndrome (data not shown). After exclusion of subjects with diabetes, the results did not change, with an OR of CKD and albuminuria associated with metabolic syndrome of 2.00 (95% CI 1.33, 3.00; P=0.001) and 2.01 (95% CI 1.44, 2.79; P<0.001), respectively.
Cluster analysis of metabolic syndrome components
Analysis of the data revealed the presence of three clusters. In the first cluster, visceral adiposity, high blood pressure, and impaired glucose metabolism were prevalent; in the second cluster, visceral adiposity, high blood pressure, and low HDL-C; in the third cluster, low HDL-C, high triglycerides, and impaired glucose metabolism. The first cluster was more frequent in subjects with metabolic syndrome and without nephropathy or CVD, and its prevalence decreased in subjects with metabolic syndrome and nephropathy and/or CVD and in subjects with metabolic syndrome and both nephropathy and CVD, whereas the second and third clusters showed the opposite tendency, although none of these trends was significant.
After multivariate adjustment, none of the interaction terms of the metabolic syndrome components reached statistical significance for CKD and albuminuria, whereas the interaction was significant for CVD between waist circumference and high blood pressure (P=0.014) with an S value of 7.43, indicating biological synergy.
Other markers of central adiposity
We investigated the association between CKD, albuminuria, and markers of central adiposity different than waist circumference, namely the waist-to-hip ratio (WHR) and the body mass index (BMI). After adjustment for age and gender, the WHR was significantly associated with albuminuria (OR=1.02, 95% CI 1.01, 1.04, P=0.029) but not with CKD (OR=1.06, 95% CI 0.42, 1.08, P=0.213), whereas BMI was significantly associated with both CKD (OR=1.03, 95% CI 1.01, 1.05, P=0.006) and albuminuria (OR=1.04, 95% CI 1.01, 1.06, P=0.001). The same findings were confirmed by analysis of ROC curves (Fig. 2): for WHR, the AUROC was 0.54 for CKD (95% CI 0.49, 0.59, P=0.096) and 0.59 for albuminuria (95% CI 0.56, 0.62, P<0.001); for BMI, the AUROC was 0.60 for CKD (95% CI 0.55, 0.65, P<0.001) and 0.60 for albuminuria (95% CI 0.56, 0.63, P<0.001). A value of WHR >0.9 showed a sensitivity and a specificity for albuminuria of 0.75 and 0.40, respectively; a value of BMI >25 showed a sensitivity and a specificity of 0.73 and 0.45 for CKD and of 0.68 and 0.55 for albuminuria, respectively. Subjects with the waist circumference trait had a significantly higher prevalence of the triglycerides trait (24.3% vs. 11.8%), the HDL trait (20.0% vs. 10.1%), the high blood pressure trait (51.6% vs. 28.4%), and the glycemia trait (43.4% vs. 24.3%) compared with subjects without the waist circumference trait (P<0.001 for all the comparisons).
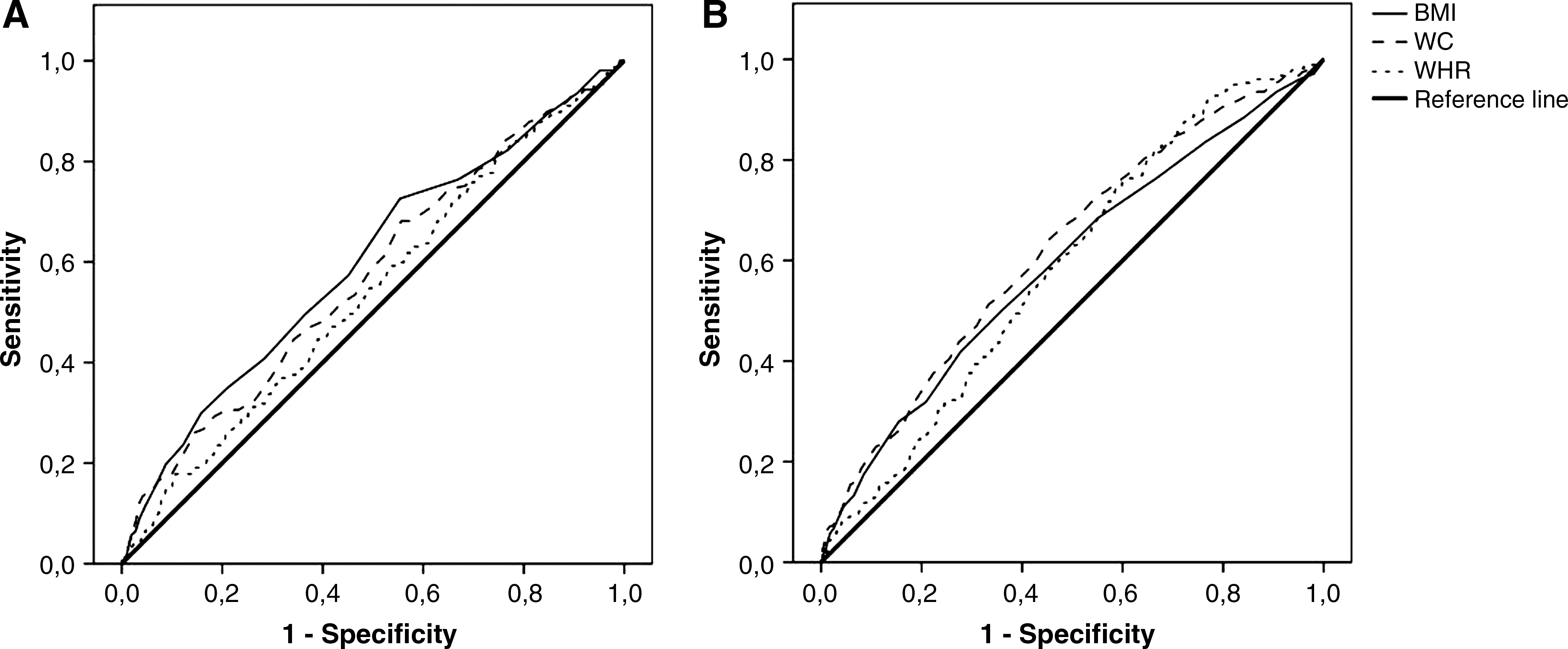
Receiver operating characteristic (ROC) curves for the association between WC, BMI, WHR, CKD, and albuminuria. Association between WC, BMI and WHR and CKD
Discussion
In the present study, we analyzed a randomly selected sample of the northern Italian adult population for the association between metabolic syndrome and presence of markers of kidney damage (reduced GFR and/or albuminuria) and previous CV events. We found that 22.4% of the subjects had metabolic syndrome, a finding consistent with published data on westernized populations. 1 As a matter of fact, in the United States the age-adjusted prevalence of metabolic syndrome has been reported to be approximately 27%. In Italy, the prevalence of metabolic syndrome has been reported to be 15%–18%, a lower figure compared with the present paper, probably because of the wider age range of the previously investigated populations. 22,23
In our study, compared with subjects without metabolic syndrome, those with metabolic syndrome were significantly older and reported a higher proportion of cardiovascular events (Table 1), which remained significant after adjustment for age and gender. That metabolic syndrome increases the cardiovascular risk is well known, 2,24 and this is confirmed by our results after adjustment for CKD and albuminuria (OR=1.58), both conditions responsible for an increase in CV risk. 4 Actually, in the INCIPE cohort, subjects with nephropathy without metabolic syndrome had a 1.70 OR from having had a CVD episode. On the other hand, subjects with both metabolic syndrome and nephropathy had the highest association with previous CVD events (OR=3.34).
The relationship between previous CVD events and metabolic syndrome is supported by the finding that the prevalence of CVD events correlated with the number of metabolic syndrome components after adjustment for nephropathy (OR for each trait 1.47).
We found a significantly higher prevalence of both CKD (7.4%) and albuminuria (15.0%) in subjects with metabolic syndrome compared with subjects without metabolic syndrome (3.3% and 5.5%, respectively). Similar findings have been reported in the U.S. adult population, 6 and in surveys from China, 7,9 Japan, 8 and other Asian countries. 10 Whether metabolic syndrome is a cause or a consequence of renal disease has been investigated by Kurella et al. 25 in the Atherosclerosis Risk in Communities (ARIC) study, in which 10,096 nondiabetic participants with normal baseline kidney function were followed for 9 years. Incident CKD developed in 10% of individuals with baseline metabolic syndrome and in 6% of individuals without baseline metabolic syndrome (P<0.001). Furthermore, the relative risk for developing CKD increased for increasing numbers of metabolic syndrome traits. Luk et al. 11 confirmed these data in a longitudinal study in which the OR for developing CKD was 1.31 (95% CI 1.12, 1.54) for individuals with metabolic syndrome. Thus, available evidence suggests a pathogenetic role of metabolic syndrome in the development of chronic nephropathy.
Our study uses a peculiar, and hence noncomparable, definition of CKD: We defined it as the presence of a GFR below the age and gender-specific 5th percentile. This conservative definition was chosen to better select subjects with a true impairment of kidney function, 20 and to avoid an overestimation of CKD, which can be common in elder people. In fact, applying the standard definition of CKD (GFR <60 mL/min), the study population would show an exponential increase in prevalence of CKD, with a possible underestimation in subjects <50 years (0.2%) and overestimation in subjects ≥80 years (35.4%). On the contrary, applying the conservative definition of CKD, the prevalence remains almost constant for each age class (on average 4%), with a slight increase in subjects ≥80 years (5.7%). However, the results of our analysis do not change when using the standard definition of CKD, i.e., <60 mL/min (data not shown).
The prevalence of both CKD and albuminuria was higher for each of the criteria defining metabolic syndrome, except for waist circumference and CKD (Table 2); in fact, each item was significantly associated with CKD and albuminuria in multivariate models, again with the exception of waist circumference and CKD (Tables 3 and 4). The presence of two or more traits of metabolic syndrome was significantly associated with CKD and albuminuria, and the risk of having CKD and albuminuria was directly related to the number of metabolic syndrome components (Tables 3 and 4, Fig. 1). Interestingly, a lack of association between waist circumference and CVD was observed (Table 5), although there seemed to be a synergic effect on CVD between central adiposity and blood pressure (S=7.43).
Regarding the lack of association between waist circumference and CKD, Chen et al. 6 found the same result. Furthermore, a similar finding has been recently reported in a cohort of 3,465 Chinese subjects with coronary heart disease: The authors found a significant association between all traits of metabolic syndrome and CKD except central obesity and hypothesized that the risk associated with central obesity may be “diluted” in other metabolic syndrome–related factors. 26 Data in our population confirm this hypothesis, because subjects with the waist circumference component had a significantly higher prevalence of all the other components compared with subjects with normal waist circumference. Therefore, either the definition of new population-specific cutoffs for central obesity or the application of more sensitive body composition analysis techniques might be necessary. Our analysis of alternative markers of obesity and their correlation with CKD and albuminuria showed a significant association between WHR and albuminuria and between BMI and both CKD and albuminuria, although these differences are difficult to interpret. Because BMI could be a proxy of lean body mass, the association with CKD (which was defined according to a specified GFR, i.e., a creatinine-derived measure) could be the expression of this rather than of a true causal relationship.
The origin of the CVD–CKD association is debated. 27 It has been proposed that, due to the large vascularization of the kidney, CKD is the expression of the same pathological process occurring in the cardiovascular system, with the metabolic syndrome being the connecting factor. However, the present results (Table 3) suggest that the renal damage induced by metabolic syndrome occurs even independently of CVD. Conversely, the association between CKD and CVD is significant (OR=2.30), even after adjustment for metabolic syndrome. Hence, these results suggest that metabolic syndrome does not entirely explain the CVD–CKD association.
It is interesting that our cluster analysis showed the presence of three distinct “phenotypes” of metabolic syndrome. One of these phenotypes, which could be called the “atherogenic phenotype” for the contemporary presence of both low HDL-C and high triglycerides, showed a tendency to associate with complicated forms of metabolic syndrome (e.g., those with already established nephropathy and/or cardiovascular disease).
Our study is limited by the fact that a single measurement of serum creatinine and urinary albumin was available. For the definition of CKD, the GFR must be constantly reduced for at least 3 months. However, all the individuals were stable at the moment of examination and unlikely to have an acute impairment of renal function. Furthermore, the same was done in other epidemiological investigations. A further limitation is that for the designation of high blood pressure, diabetes mellitus, and cardiovascular disease, we relied also on self-reported diagnoses, which, however, are not excluded by the definition of NCEP ATP III criteria. Due to the previous occurrence of CVD events and the cross-sectional design of the study, it is not possible to infer any causal relationship between metabolic syndrome, CVD, and nephropathy. Furthermore, there could be a survival bias. However, our data showing an association of metabolic syndrome and nephropathy and CVD events are consistent with a number of previous observations supporting their plausibility.
In conclusion, the present data confirm the association between metabolic syndrome and renal disease in an ethnically homogeneous Caucasian European population and support the idea that, although metabolic syndrome is a risk condition for both CVD and CKD, it does not entirely explain the dangerous relationship between CVD and renal disease.
Footnotes
Acknowledgments
The cross-sectional phase of the INCIPE study was co-sponsored by Fondazione Cassa di Risparmio di Verona, Azienda Ospedaliera di Verona, and University of Verona. The present substudy was sponsored by Ministero della Salute, Programma Strategico 2006 “Costituzione di un Network multi-regionale per migliorare il management clinico del paziente nefropatico,” and Project “Stima della prevalenza dell'Insufficienza Renale Cronica (IRC) in diverse Regioni di Italia e “follow-up” dei pazienti affetti da I.R.C.
The INCIPE study group composition was as follows.
Study Design: G. Gambaro, A. D'Angelo, A. Lupo. Statistics: F. Grigoletto, A.C. Frigo, P.M. Ferraro. General coordination: G. Gambaro, A. Lupo.
Local coordination: L. Bonfante, P. Conz, G. Meneghel, G. Gambaro.
Data base and Privacy: A. Legnaro. Laboratory: M.S. Graziani, P. Rizzotti, A. Sorio, L. Mantovani. GFR validation: C. Abaterusso, M.S. Graziani, G. Gambaro, F. Van Lente, C. O'Laughlin. Enrolling physicians: C. Canciani, S. Casarotti, L. Citron, A. Gemelli, N. Marchionna, P. Romano, S. Tata, T. Yabarek.
Logistics: T. Yabarek. GPs: Dolo: G. Agnesini, C. Barolo, F. Boscaro, A. Braga, C. Cotrino, D. Danieli, L. Favero, A. Gallo, C. Garzotto, P.A. Marcato, G. Masoch Bof, I. Mattiello, E. Mioni, O. Oliva, E. Olivo, D. Pettenà, D. Pinton.
Monselice: A. Trimarchi, M. Borin, F.M. Andolfo, G. Bernardi, D. Colombara, R. Finco, R. Lancerotto, E. Marcato, L. Marini, R. Ragliani, R. Ramponi, S. Romano, G. Scolaro, F. Seren, L. Simonato, F. Toniato, G. Varotto, G. Zilio.
Padova: M.R. Cappellari, R. Castrignano, A. Fragasso, C. Gardellin, M. Nobile, G. Mazzuccato, L. Mazzuccato, G. Pisani, L. Rossetto, D. Sandon, S. Tardia.
Verona: S. Agnello, B. Bresaola, P. Cortina, F. Del Zotti, S. Carlini, S. Ferrara, M. Ferroni, P. Garonzi, S. Marinelli, C. Melotti, M. Sighele, C. Sovran, T. Sandrini, A. Tosi, G. Tosi, and V. Villani. Secretarial assistance: N. Faccio, A. Zambelli.
Author Disclosure Statement
No competing financial interests exist.