
Abstract
Background:
Adipokines are markers of insulin resistance and play a role in the atherosclerotic process. The association of adipokines with the macrovascular complications of type 1 diabetes mellitus (DM) needs to be determined. The aim of this study was to measure serum adiponectin, leptin, and resistin levels in type 1 DM patients and investigate their relationship with carotid intima media thickness (CIMT), a clinical marker of atherosclerosis.
Methods:
Seventy-five type 1 DM patients and 115 sex and age-matched healthy controls were included in the study. Serum adiponectin, leptin, and resistin levels were measured by the enzyme-linked immunosorbent assay (ELISA method). CIMT was assessed by Doppler ultrasonography
Results:
Adiponectin levels in diabetics were higher (25.8±14.8 μg/mL vs. 5.5±7.3 μg/mL; P<0.0001) and leptin levels were lower than controls (9.4±6.2 ng/mL vs. 12.8±8.6 ng/mL; P=0.01). Resistin levels were also higher in the diabetic group compared to controls (2.1±1.4 ng/mL vs. 1.6±0.8 ng/mL; P=0.04). Adiponectin was correlated negatively with CIMT (r=−0.24, P=0.03), age (r=−0.30, P=0.02), BMI (r=−0.33, P=0.02), waist-to-hip ratio (WHR) (r=−0.38, P=0.01) and positively with creatinine (r=0.44, P=0.004). Leptin levels were correlated with total cholesterol (r=0.53, P=0.01) and high-density lipoprotein (HDL) (r=0.67, P=0.001). Resistin was correlated with CIMT (r=0.24, P=0.03) and systolic blood pressure (r=0.48, P=0.009). Multivariate analysis revealed resistin and creatinine to be independent predictors of CIMT among adiponectin, leptin, resistin, WHR, glycosylated hemoglobin (HbA1c), and creatinine.
Conclusions:
Increased adiponectin correlates negatively and resistin positively with CIMT in type 1 diabetic patients, but adjusting for other known predictors reveals only resistin to be associated with subclinical atherosclerosis in this group of patients.
Introduction
Serum adipokines have been demonstrated to be associated with insulin resistance. Adiponectin regulates energy homeostasis and increases insulin sensitivity, 5,6 along with possible antiatherogenic and antiinflammatory properties. 7,8 Leptin is another adipokine that is involved in regulation of energy homeostasis, with direct effects on lipolysis, insulin secretion, and insulin sensitivity. 9,10 Hyperleptinemia has contributed to cardiovascular risk in patients with the metabolic syndrome. 11 Resistin is a novel adipokine that has been suggested to enhance insulin sensitivity in rodent models. 12 Although a possible role of resistin on vascular endothelial cells has been demonstrated, 13,14 serum resistin levels are generally found to be unrelated to markers of insulin resistance. 15,16
Clinical studies indicate that adiponectin levels are elevated in patients with type 1 DM compared to nondiabetic controls. 17 –20 Leptin levels are lower in adult type 1 DM patients compared to patients with type 2 DM and controls. 21 There are conflicting reports about resistin levels in type 1 DM patients. 22,23
The increase in adiponectin is more prominent in type 1 DM patients with microvascular complications. 17,19,24 Adiponectin and leptin are predictors of microvascular complications in type 1 DM patients. 25 Serum adiponectin levels predict all-cause mortality in type 1 diabetic patients with overt diabetic nephropathy. 26 The relationship of resistin with microvascular complications of type 1 DM has not been investigated.
Conflicting data exist concerning the association of different adipokines with markers of macrovascular disease. 17,27 –31 Moreover, the role of adipokines in macrovascular disease of type 1 DM is questionable.The aim of the present study was to determine serum adiponectin, leptin, and resistin concentrations in type 1 DM patients and to determine their relationship with carotid intima media thickness (CIMT), as an early marker of atherosclerosis.
Materials and Methods
Patients
Seventy-five type 1 DM patients with a disease duration of at least 1 year were included in the study. The patients were selected consecutively from our outpatients clinic. The diagnosis of type 1 DM was based on the presence of autoantibodies. The control group consisted of 115 sex and age-matched healthy people. The study protocol was approved by the local research ethics committee and and was carried out in accordance with the declaration of Helsinki. All subjects gave written informed consent.
Medical history was obtained, physical examination was performed in all patients and controls, and electrocardiograms were recorded. Blood was withdrawn from all subjects following 12 h of fasting. Two or more timed overnight urine collections were used to measure urinary albumin excretion., and fundoscopic eye examinations were performed to assess retinopathy. Patients were evaluated for neuropathy by medical history and neurologic examination.
Subjects with ischemic heart disease, valvular heart disease, congestive heart failure, any other systemic or inflammatory disease, patients with cardiac symptoms and abnormal electrocardiogram (ECG), and patients on any antihypertensive agents or any medication other than insulin were excluded.
Anthropometric measurements
Anthropometric measurements of body weight, height, waist circumference, and hip circumference were performed with the patient dressed in underwear. Body mass index (BMI) was calculated as body weight divided by height squared. Waist circumference was measured at the midpoint between the lateral iliac crest and lowest rib. Hip circumference was measured at the level of the greater trochanter. The waist-hip-ratio (WHR) was calculated as the ratio of waist circumference to hip circumference.
Biochemical measurements
Serum adiponectin, leptin, and resistin were measured using the sandwich enzyme-linked immunosorbent assay (ELISA) method (Thermo Scientific Muitiskan FC, Finland). The intraassay and interassay variabilities were 1.0%–7.4% and 2.4%–8.4% for adiponectin, 2.6%–4.6% and 3.8%–4.0% for leptin, and 2.6%–6.2% and 7.1%–7.7% for resistin. Glycosylated hemoglobin (HbA1c) levels were measured by high-pressure liquid chromatography (HPLC) with a Thermo system. Fasting blood glucose (FBG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides were measured by enzymatic colorimetric assays (Roche Diagnostics GmbH, Mannheim, Germany). Serum creatinine was determined by kinetic calorimetry (Roche Diagnostics GmbH, Mannheim, Germany). The estimated glucose disposal rate (eGDR) was calculated as defined before. 32
Statistical analysis
Statistical analysis was performed with a SPSS software package. Comparisons of continous variables were done using the Student unpaired t-test or Mann–Whitney U-test according to the distribution of values. The chi-squared test was used for the comparison of categorical variables. Correlation analysis was performed using Pearson or Spearman tests where appropriate. We evaluated for potential associations of serum adiponectin with age, BMI, WHR, creatinine and CIMT, leptin with WHR, total cholesterol, HDL and CIMT, and resistin with WHR, systolic blood pressure (SBP), creatinine and CIMT. Moreover linear regression analysis was performed for the determinants of CIMT, where adiponectin, leptin, resistin, WHR, HbA1c, and creatinine were the independent variables. Levels of statistical significance were set at a P value<0.05. The results were expressed as mean±standard deviation (SD).
Results
The demographic findings and laboratory values of the study groups are shown in Table 1. Fasting blood glucose and HbA1c levels were higher in the diabetic group compared to controls. Diastolic blood pressures (DBP) of the patients were comparable to controls eGDR of the patients was lower than controls. Two patients had retinopathy, 5 patients had nephropathy in the form of microalbuminuria, and 6 patients had neuropathy. CIMT measurements in the diabetic patients were higher than controls (Table 1). Adiponectin and resistin levels in the diabetic patients were higher, whereas leptin levels were lower than controls (Fig. 1).
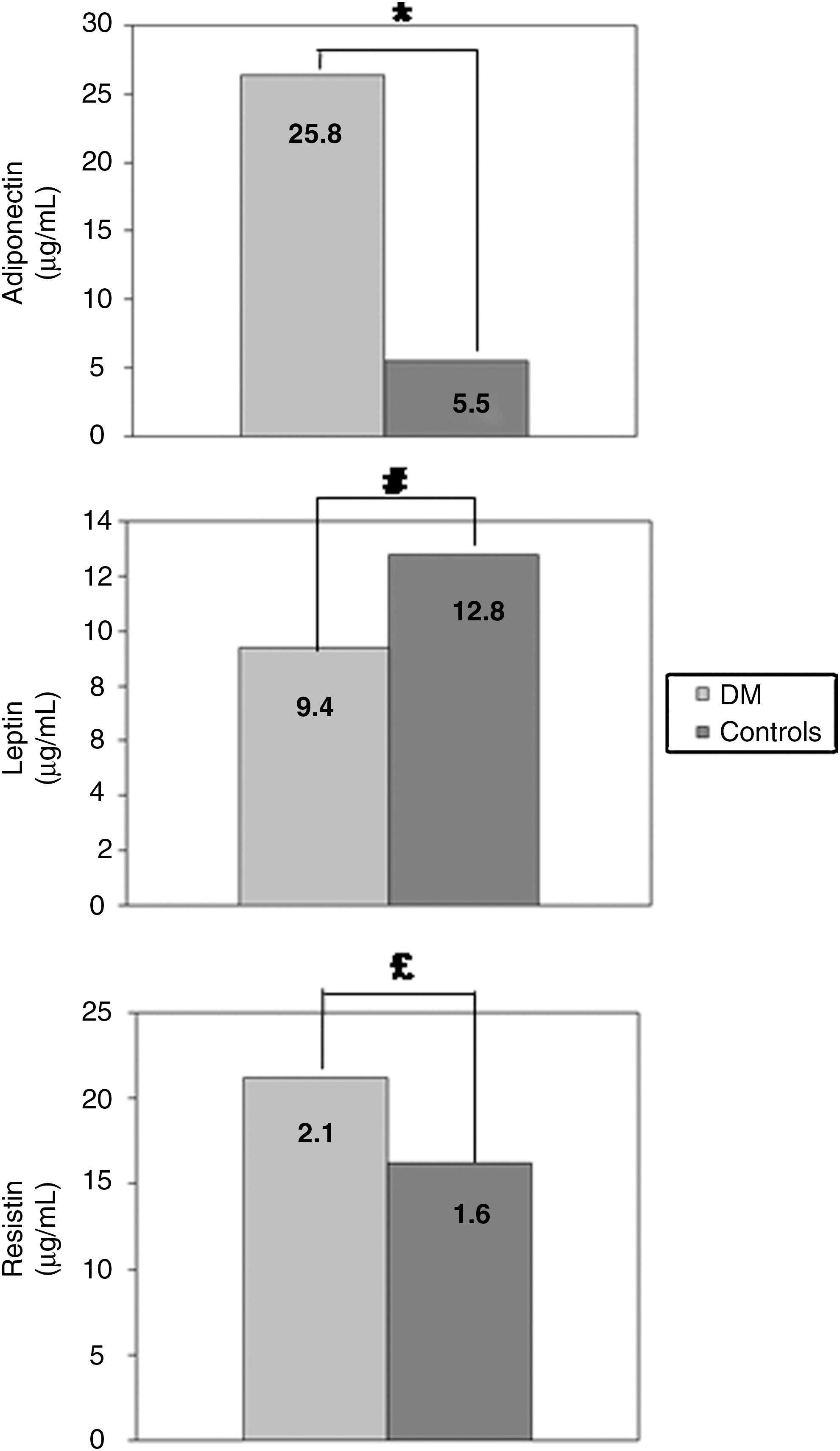
Comparison of adiponectin, leptin, and resistin among type 1 diabetic patients and controls. (*) P<0.0001; (#) P=0.01; (£) P=0.04.
Values are expressed as means±SD.
CIMT, carotid intima media thickness; N.S., not significant; DM, diabetes mellitus; F/M, female/male; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; WHR, waist-to-hip ratio; eGDR, estimated glucose disposal rate; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Adiponectin levels were correlated negatively with CIMT (Fig. 2), age (r=−0.30, P=0.02), BMI (r=−0.33, P=0.02), and WHR (r=−0.38, P=0.01) and positively with eGDR (r=0.32, P=0.01) and creatinine (r=0.44, p=0.004), whereas no correlation was observed with duration of diabetes, SBP and DBP, HbA1c, FBG, and lipid levels. When regression analysis was performed with adiponectin as the dependent variable and age, BMI, WHR, creatinine, and CIMT as the independent ones, WHR was associated with a borderline significance (r 2=0.34, P=0.05). When CIMT was excluded from the model, the relationship of WHR with adiponectin became significant (r 2=0.30, P=0.03).
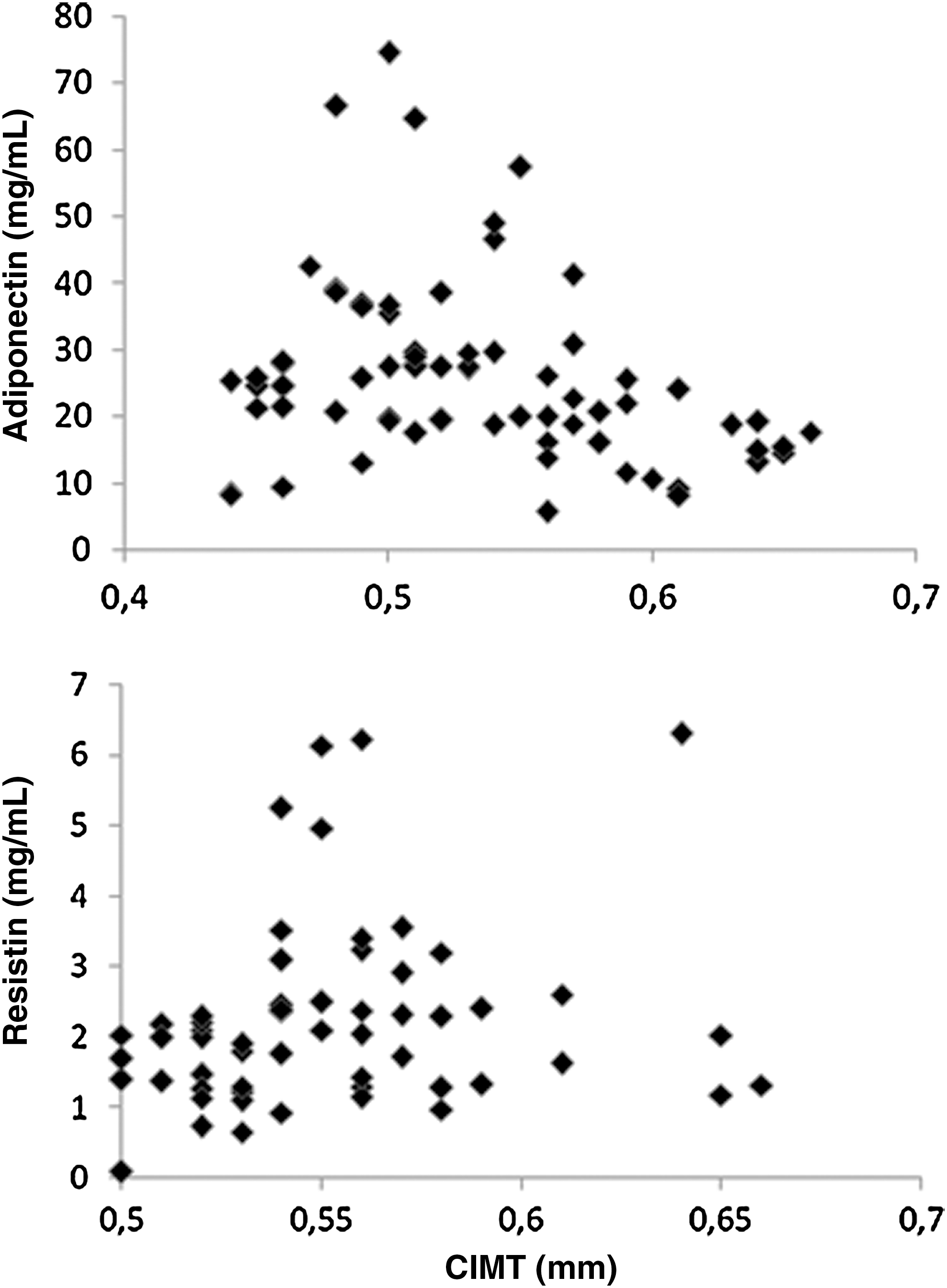
Scatter plots showing correlation of adiponectin with CIMT (r=−0.24, P=0.03) and resistin with CIMT (r=0.24, P=0.03) within the diabetic group.
Leptin was correlated with total cholesterol (r=0.53, P=0.01) and HDL levels (r=0.67, P=0.001), whereas no correlation was observed with age, BMI, WHR, duration of diabetes, SBP and DBP, eGDR, HbA1c, FBG, creatinine, triglyceride, LDL levels, and CIMT measurements. Regression analysis did not show an association of leptin with WHR, total cholesterol, HDL, and CIMT as independent variables.
Resistin was correlated with CIMT (Fig. 2) and SBP (r=0.48, P=0.009), whereas no correlation was observed with age, BMI, WHR, duration of diabetes, DBP, eGDR, HbA1c, FBG, creatinine, and lipid levels. When regression analysis was performed with a model including resistin as the dependent variable and WHR, SBP, creatinine, and CIMT as independent variables, CIMT and SBP were related (r 2=0.44, P=0.006).
Regression analysis performed to document the predictors of CIMT among adiponectin, leptin, resistin, WHR, HbA1c, and creatinine, revealed resistin and creatinine to be influential (r 2=0.77, P=0.02).
Discussion
We investigated the presence of different adipokines in a type 1 DM population and their association with CIMT. To our knowledge, this is the first study investigating the association of different adipokines with subclinical atherosclerosis in adult type 1 DM patients. The results revealed increased adiponectin and resistin along with decreased leptin concentrations in the diabetic patients compared to controls. Whereas adiponectin was correlated negatively and resistin positively with CIMT, no correlation of leptin with CIMT was observed. Adjusting for other known predictors of CIMT left only resistin to be associated with CIMT.
Adiponectin levels have been previously demonstrated to be elevated in patients with type 1 DM. 17 –20 The association of adiponectin with cardiovascular events is also evident from previous data. 33,34 Insulin resistance has been suggested to play role in the macrovascular complications of type 1 DM. 2 –4 Costacou et al. examined type 1 DM patients with coronary artery disease (CAD), determined by physician-diagnosed angina, confirmed myocardial infarction, stenosis greater than 50%, ischemic ECG, or revascularization. They observed decreased levels of adiponectin in type 1 DM patients that developed CAD compared to ones who did not. They reported a 63% reduction in the risk of CAD per 6.3 μg/mL increase in serum adiponectin levels after controlling for urinary albumin excretion. 28 Frystyk et al. have determined adiponectin levels in a type 1 DM population of 391 subjects and 25 controls. They demonstrated increased levels of adiponectin in the patient group, with adiponectin levels being even higher in patients with nephropathy. Adiponectin levels were also increased in 24 patients with microalbuminuria and 60 patients with overt nephropathy who developed cardiovascular disease, assessed by medical history and resting ECG. However these differences became insignificant after adjustment for diabetes duration, sex, daily insulin dose, HbA1c, BMI, SBP, and renal function in multivariate analysis. 17
Our results regarding increased adiponectin in our patient group is in accordance with the previously mentioned data. In our study, we have determined CIMT as a marker of cardiovascular disease. CIMT was increased in our diabetic population in comparison to healthy controls. The increased levels were correlated negatively with adiponectin, but when multivariate analysis was performed, this association became insignificant. The fact that adiponectin was correlated negatively with CIMT is in concert with Costacou's finding of decreased adiponectin in patients that developed CAD. However in our study, the association became insignificant after adjusting for other variables. Thus, our results coincide with those of Frytsk et al. but are at variance with those of Costacou's, where the number of subjects was limited compared to our group. In the multivariate analyses concerning the association of adiponectin with CIMT, when we corrected for age, BMI, WHR, and creatinine, which were all separately found to be correlated with adiponectin; only WHR was left to be effective, with a borderline significance. This suggests that adiponectin may be related to CIMT through its association with WHR, a clinical surrogate of insulin resistance. Thus, adiponectin itself does not seem to be associated directly with increased CIMT in these patients.
Low levels of adiponectin have been associated with CAD. 33,34 Interestingly, adiponectin is generally elevated in type 1 DM patients, especially in patients with microvascular complications. There is conflicting evidence about adiponectin levels concerning macrovascular complications in type 1 DM patitents, 17,28 thus the true association with macrovascular disease needs to be determined. One suggestion for the elevation in microvascular disease in type 1 DM is that it is a compensatory response due to its antiinflammatory and antiatherosclerotic properties. 17 Perhaps high-molecular weight adiponectin may be the culprit, although it has been found to be unaffected by nephropathy status in type 1 DM patients. 35
Leptin levels were reported to be decreased in adult patients with type 1 DM by Roden et al., 21 and our findings coincide with these results. Atabek and his colleagues have demonstrated that leptin was related to cross-sectional compliance, cross-sectional distensibility, and incremental elastic modulus of the common carotid artery in children and adolescents with type 1 DM. 31 Leptin was also associated with CIMT in type 2 DM patients. 36 Our results revealed no association of CIMT with leptin.
Resistin levels have been found to be decreased in adult type 1 DM patients compared to controls. 23 Another group found no difference in resistin levels between type 1, type 2 DM patients, and controls. 22 Resistin levels were higher in type 2 DM patients with CAD. Moreover resistin levels were even higher in patients with restenosis. 37 Neither adiponectin nor resistin was found to be associated with the vascular reactivity test, used as a marker for endothelial dysfunction in patients with type 2 DM and patients at risk of diabetes. 27 Our findings revealed elevated resistin levels in adult-type diabetic patients with respect to controls. Resistin was correlated positively with CIMT. Furthermore, multivariate analysis revealed that resistin was the only adipokine in this population to be associated with CIMT when corrected for other possible risk factors. Thus, increased resistin in type 1 DM patients seems to be suggestive of subclinical atherosclerosis. Because serum resistin levels are generally unrelated to markers of insulin resistance 15,16 and the association of adiponectin and leptin with insulin resistance seems to be more evident, 5,6,9,10 the sole relationship of resistin with CIMT in this population of type 1 DM patients raises a question about the association of insulin resistance with macrovascular complications.
Our findings are novel given that adiponectin levels have been demonstrated to be low in type 1 DM patients with known coronary artery disease 28 ; however, no data were evident to the authors regarding the levels of adiponectin with only increased CIMT, indicating only subclinical atherosclerosis. Leptin was related to cross-sectional compliance, cross-sectional distensibility, and incremental elastic modulus of the common carotid artery in children and adolescents with type 1 DM, 31 but not adults. Association of leptin with CIMT was shown in type 2 DM patients, 36 but not adult type 1 DM patients. Higher resistin levels were demonstrated in type 2 DM patients with coronary artery disease 37 but not in type 1 DM patients as far as we know.
In conclusion, adiponectin and resistin are increased whereas leptin is decreased in type 1 DM patients. Adiponectin levels correlate negatively and resistin levels correlate positively with CIMT; however, after adjusting for other known predictors, only resistin is associated with subclinical atherosclerosis in this group of patients. Further studies with larger populations are needed also to determine the association of adipokines with coronary artery disease in type 1 DM patients and to decipher the pathogenetic mechanism behind this association.
Footnotes
Author Disclosure Statement
No competing financial interests exist.