
Abstract
Background:
The aim was to analyze the impact of obesity on women with gestational diabetes mellitus (GDM) and the association of obesity and GDM with the metabolic syndrome.
Methods:
In a retrospective study, the data of 233 obese women with GDM were compared with the data of 96 women with GDM and normal weight.
Results:
Significantly higher fasting glycemia before the oral glucose tolerance test (5.2±1.1 mmol/L vs. 4.5±0.8 mmol/L, P<0.00001) and higher frequency of hypertensive disorders of pregnancy (26.2% vs. 9.4%, P=0.0003) were found in obese women with GDM than in GDM women of normal weight. These women needed insulin therapy more often (18.9% vs. 8.3%, P=0.007). Also 31 (13.3 %) of them had chronic hypertension as compared with 3.1% in women of normal weight (P=0.003). These 31 women had three components necessary for diagnosing of metabolic syndrome according to the World Health Organization—impaired glucose tolerance, obesity, and hypertension. No difference in gestational age and mean weight of their newborns was found, but newborns of obese GDM women with metabolic syndrome components more often were significantly macrosomic with features of diabetic fetopathy and had more often symptoms of hypoglycemia after birth.
Conclusions:
The presence of obesity and GDM has a significant impact on both maternal and fetal complications. The metabolic syndrome can be diagnosed not only after pregnancy but also during pregnancy.
Introduction
It is well known that the women with a history of GDM have an increased risk of developing metabolic syndrome later in their life 6,7 as well as type 2 diabetes, which increases the risk of cardiovascular diseases (CVD) as well as morbidity and mortality. 8,9 The aim of this study was to analyze the impact of obesity on women with GDM and the association of these conditions with metabolic syndrome.
Material and Methods
In a retrospective study, the data of 233 obese women with GDM were analyzed and compared with the data of 96 women with GDM and normal weight. The study was approved by our local ethics board (protocol N.BE-2-4).
GDM was diagnosed according to the World Health Organization (WHO) criteria using a 75-gram oral glucose tolerance test, when the glucose was ≥7.8 mmol/L (2 h). Prepregnancy body mass index (BMI) ≥30 kg/m2 was defined as obesity and normal weight was a BMI <25 kg/m2.
Metabolic syndrome was diagnosed according to the WHO criteria—impaired glucose tolerance or diabetes mellitus and/or insulin resistance (in our case GDM) with two of the following components, hypertension, central obesity, or BMI ≥30 kg/m2 and/or dislipidemia. 10
Macrosomia, or a large for gestational age (LGA) newborn, was defined as a birth weight ≥90th percentile for gestational age and sex according to the Lithuanian standard population. Glycemia <2.6 mmol/Lduring the first 48 h of life was the criterion for neonatal hypoglycemia. Hyperbilirubinemia was diagnosed when bilirubin levels exceeded the physiological level in absence of hemolysis. Congenital malformations were diagnosed during the hospital stay.
Statistical analyses performed using the SPSS statistical package (version 12.0; Chicago, IL). Data in text and tables are presented as means±standard deviation (SD). The chi-squared or Fisher exact test was used to compare proportions among groups. The difference between two independent samples was calculated using the Mann–Whitney U-test. P<0.05 on two-sided tests was considered statistically significant.
Results
Maternal characteristics and obstetrical complications in obese and normal-weight women with GDM are presented in Table 1. Obese women with GDM were older (31.5±5.8 vs. 27.5±5.6 years), their fasting glycemia was higher (5.2±1.1 mmol/L vs. 4.5±0.8 mmol/L), and they were treated more often with insulin (18.9% vs. 8.3%). An increased rate of obstetrical complications was found in these women; the frequency of hypertensive disorders of pregnancy was three-fold and polyhydramnios almost two-fold higher. The rate of chronic hypertension (diagnosed before pregnancy) was four-fold higher in obese women than in women with normal weight (13.3% vs. 3.1%).
Data are means±standard deviation (SD) or n (%).
GDM, gestational diabetes mellitus.
The main neonatal characteristics and complications in the newborns are presented in Table 2. Newborns of obese women with GDM had significantly higher birth weights, and macrosomia was found six-fold more often when compared with the newborns of normal-weight women with GDM. Half of newborns with macrosomia had signs of diabetic fetopathy with cushingoid outlook and visceromegaly.
Data are mean±standard deviation (SD) or n (%).
GDM, gestational diabetes mellitus.
Thirty-one women with GDM matched at least three WHO diagnostic criteria of metabolic syndrome—glucose intolerance, obesity, and chronic hypertension (not associated with pregnancy). No significant difference was found in maternal age and parity of women with metabolic syndrome and the rest of GDM obese women (n=202), but women with metabolic syndrome were more often treated with insulin (29.3% vs. 17.3%). The main characteristics of newborns of obese women with GDM and metabolic syndrome are presented in Table 3. No difference in gestational age and mean weight was found, but newborns of obese GDM women with metabolic syndrome were macrosomic more often and had features of diabetic fetopathy and hypoglycemia after birth (Fig. 1).
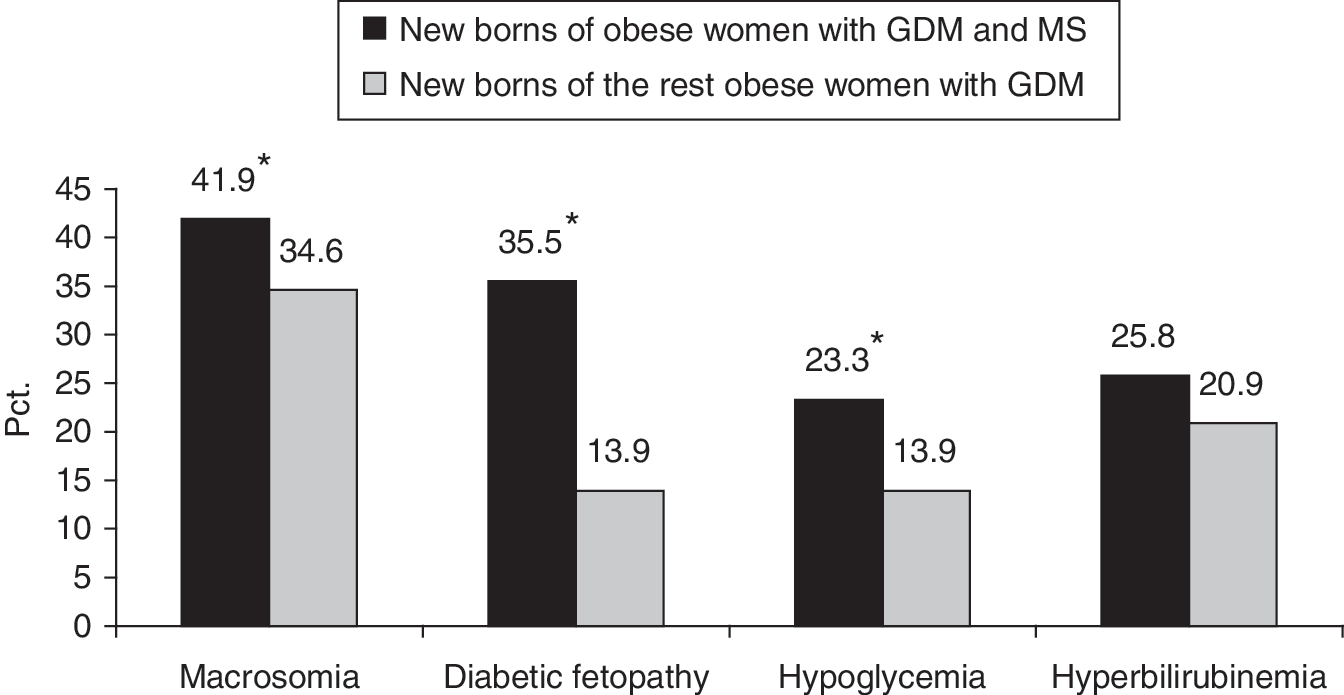
Neonatal complications of the newborns of obese women with gestational diabetes mellitus (GDM) and metabolic syndrome (MS) components compared with the newborns of the rest GDM obese women. (*) P<0.05.
GDM, gestational diabetes mellitus.
Discussion
GDM and obesity are closely connected. Many studies have reported a higher risk of GDM with an increase of BMI. 3,11 In a metaanalysis, Chu et al. reported that the risk of developing GDM is about two-, four-, and eight-fold higher in overweight, obese, and severely obese women, respectively, when compared with normal-weight pregnant women. 12
Although most authors analyze the impact of GDM and obesity on outcomes of pregnancy separately, 13 –17 we investigated the influence of both factors together. GDM in obese women was associated with increased frequency of hypertensive disorders of pregnancy, chronic hypertension, and higher rate of cesarean section as compared with nonobese (normal weight) women with GDM. Higher fasting glycemia and more often insulin therapy, which refer to higher degree of insulin resistance, were observed in obese women with GDM. Newborns of these women had macrosomia more often and features of diabetic fetopathy—signs of hormonal disturbances.
Several studies show the association of GDM with the risk of development of metabolic syndrome later in life. 18 –21 Lauenborg et al. have reported that obese women with history of GDM had a seven-fold higher prevalence of the metabolic syndrome than normal-weight women. 22 Vohr et al. have shown that women with a history of GDM and obesity were at a significantly greater risk of developing metabolic syndrome than mothers with no history of GDM or obesity, and they named GDM as a forerunner of metabolic syndrome. 23 We suggest that metabolic syndrome can be diagnosed not only after pregnancy but also during pregnancy. We found that 31 (13.3%) of 233 obese women with GDM matched at least three WHO diagnostic criteria for metabolic syndrome—impaired glucose tolerance, obesity, and chronic hypertension. Newborns of these women more often were LGA and had signs of diabetic fetopathy.
Other studies also suggest that metabolic syndrome can be diagnosed during pregnancy in women with GDM. According Sattar et al., even normal pregnancy can be described as some transient excursion into the metabolic syndrome. 24 Clark et al. suggest that many of the known metabolic components of the metabolic syndrome are predictive for GDM, and GDM is one phase of the syndrome. 25 Bartha et al. have reported metabolic syndrome in one-third of women with pregnancy-induced hypertension and in 10% of women with late-onset GDM, 26 but pregnancy-induced hypertension can not be a component of metabolic syndrome because in most cases it is transient.
Recent studies show that obesity and GDM have a significant impact not only on fetal complications during pregnancy, but LGA offspring of diabetic and obese mothers have increased risk of developing metabolic syndrome in childhood and later in life. 27,28 That means that fetuses of obese mothers develop insulin resistance in utero. 14 Therefore, early diagnosis of metabolic syndrome is important for prevention of cardiovascular adverse events not only in women but also in their children.
In conclusion, the presence of obesity and GDM has a significant impact on both maternal and fetal complications. The metabolic syndrome can be diagnosed not only after pregnancy but also during pregnancy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.