
Abstract
Background:
Change in high-density lipoprotein cholesterol (HDL-C) observed in large randomized controlled trials using fibrates has varied. Inconsistent cardiovascular outcomes have also been the common theme of these trials. Subgroup analysis of even the negative trials, however, reveals significant reduction in cardiovascular disease in patients with low HDL-C and high triglycerides. We wished to study HDL-C change following fibrate therapy in our lipid clinic and determine the factors associated with HDL-C change.
Methods:
Data were collected from case notes of patients started on fibrates (n=248) between 2002 and 2008 in the lipid clinics at Heart of England NHS Foundation Trust. Regression analyses were carried out to determine factors associated with changes in HDL-C.
Results:
Linear regression analysis revealed that HDL-C change was associated with pretreatment HDL-C (P<0.001), diabetes (P=0.004) and treatment duration (P=0.036). Multiple regression analysis with all of the factors in the model suggested that they were independent. Patients with a baseline HDL-C <1.0 mmol/L showed a greater HDL-C increase when compared to patients with a baseline HDL-C ≥1.0 mmol/L; HDL-C <1.0 mmol/L (increase of 0.15 mmol/L, linear regression: c=0.14, 95% confidence interval 0.05–0.30, P<0.001) and HDL-C ≥1.0 (increase of 0.002 mmol/L, linear regression: reference category). A similar relationship between change in HDL-C and baseline HDL-C was observed within groups stratified by patient characteristics (apart from those on concurrent statin therapy and females).
Conclusions:
Our results may explain the discrepancies observed in some randomized controlled trials whereby subgroup analysis of patients with the metabolic syndrome appeared to show benefit whereas this was absent in the total cohort. Thus, future interventional studies using fibrates should perhaps focus on patients with low HDL-C levels.
Introduction
There are many potential mechanisms by which HDL-C can affect progression of atherosclerosis. These include efflux of cholesterol from arterial walls, prevention of endothelial dysfunction, and possession of both antiinflammatory and antioxidant properties. 7 –10
Fibrates bind and activate peroxisome proliferator-activated receptor-α (PPAR-α), leading to the activation of a nuclear transcription factor that in turn regulates expression of genes involved in regulating fatty acid and lipoprotein metabolism. 11 –13 These include genes coding for apoliporpotein AI (Apo AI), Apo AII, Apo C-III, lipoprotein lipase (LPL), adenosine triphosphate (ATP)-binding cassette transporter 1 (ABCA1), chosteryl ester transfer protein (CETP), scavenger receptor class B1(SR-B1), and ApoA5. 14 The effect on the lipid profile following fibrate therapy includes a modest decrease in LDL-C concentrations, a variable increase in HDL-C concentrations, and a greater reduction in TG levels. 15 Increase in HDL-C levels following fibrate treatment has been reported to be maximal in patients with low HDL-C at baseline. 16 Kornitzer et al. reported a significant 15.2% mean increase in HDL-C in 1,334 patients after 6 months of treatment with 200 mg of micronized fenofibrate. 16 Patients with baseline HDL-C equal or lower than 0.91 mmol/L (35 mg/dL) demonstrated a larger significant increase of 37.9%.
HDL-C increases following fibrate therapy in large intervention studies have varied significantly. Baseline and percentage increase in HDL-C observed with fibrates are as follows: Veterans Affairs High-Density Lipoprotein Intervention Trial (VAHIT; gemfibrozil), baseline 0.8 mmol/L, increase 6.3%; Bezafibrate Infarction Prevention Study (BIPS; bezafibrate), baseline 0.9 mmol/L, increase 17.9%; Action to Control Cardiovascular Risk in Diabetes (ACCORD), 0.98 mmol/L, increase 8.4%; Fenofibrate Intervention and Event Lowering in Diabetes (FIELD; fenofibrate), baseline 1.1 mmol/L, increase 2.6%; Helsinki Heart Study (HHS; gemfibrozil), baseline 1.2 mmol/L, increase 8.2%. In contrast with the consistent results observed following reduction in LDL-C in statin trials [Scandinavian Simvastatin Survival Study (4S), 17 West of Scotland Coronary Prevention Study group (WOSCOPS), 18 Heart Protection Study (HPS), 4 Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER 19 )], only VAHIT and HHS have resulted in a significant reduction in primary outcome. However, subgroup analysis of ACCORD, 20 HHS, 21 VAHIT, 22 BIP, 23 and FIELD 24 has suggested that cardiovascular benefits appear to be maximal in subjects with insulin resistance and other characteristics of the metabolic syndrome.
The dyslipidemia clinics run at the Heart of England NHS Foundation Trust [Good Hope Hospital (GHH) and Birmingham Heartlands Hospital (BHH)] have used fibrates in patients with severe hypertriglyceridemia and those with the atherogenic lipoprotein phenotype. In light of the considerable variation in HDL-C change in the above-described fibrate trials, we wished to ascertain the changes in HDL-C following fibrate treatment in our clinical setting. We also wished to determine if the observed HDL-C change was associated with any pretreatment baseline characteristics.
Patients and Methods
Patients started on fibrates between 2002 and 2008 in the lipid clinics run by the Heart of England NHS Foundation Trust were identified from the electronic patient record databases by using appropriate search keywords. Data were collected from 248 consecutive case notes of patients: GHH, 150 patients; BHH, 98 patients. The proportion of Asian patients varied between the two sites [GHH, 5 patients (3.3%); BHH, 19 patients (19.4%)]. Lifestyle advice was given to all patients at the initial appointment and this preceded fibrate treatment. The prefibrate treatment total cholesterol (TC), TG, HDL-C, calculated LDL-C, and creatinine concentrations were obtained from the pathology database just prior to fibrate initiation. The posttreatment levels were the most recent results available (up to March 30, 2009) or prior to addition of further agents that could influence lipid values (including medication used in the treatment of dyslipidemia or diabetes).
TC, TG, and HDL-C levels were measured on the Roche Modular P800 platform analyzer in both sites using Roche reagents. LDL-C was calculated on the laboratory computer system using the Friedwald equation when TG and HDL-C values were available and when TG levels were below 4.5 mmol/L. The data were entered on an Excel spreadsheet and then transferred to the STATA (version 8.0 for Windows) statistics program for analysis. A paired t-test was performed to determine significant change in HDL-C following fibrate treatment. Linear and multiple regression analyses were carried out to study factors that were associated with change in HDL-C. When the independent variable was not continuous in these regression analyses, one characteristic of the variable was chosen as the reference category. All of the other characteristics of that variable were then factorized and compared to the reference category with regard to the selected outcome (dependent variable). Thus the ability to factorize variables allowed multiple comparisons to be made on a single model.
Results
Demographic details in patients treated with fibrates
The characteristics of the patients studied are presented in Table 1. Males made up 73% of our patient group. Diabetes and hypertension requiring treatment was observed in 34% and 53.6% of patients, respectively. Amongst patients with diabetes, the mean pre- and posttreatment glycosylated hemoglobin (HbA1c) values were 8.1% and 7.9%, respectively (paired t-test, p=0.96). Fenofibrate was the most commonly prescribed fibrate (213 patients, 85.9%) followed by bezafibrate (27 patients, 10.9%). Of the patients on fenofibrate, 76.5% were on 160 mg daily followed by 17.1% on 267 mg daily. Statins were prescribed in 131 (52.8%) patients before fibrates were started.
SD, standard deviation; TC, total cholesterol; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; creat, creatinine.
The dyslipidemia characterizing the metabolic syndrome includes TG above 1.7 mmol/L and HDL-C below 1.0 mmol/L and 1.3 mmol/L in males and females, respectively. 25 Among our patients, 44.6% of males and 60.3% of females had pretreatment HDL-C in keeping with the metabolic syndrome. The large majority of patients (96.8%) had pretreatment TG above 1.7 mmol/L. This suggests that fibrates in our practice were primarily prescribed in patients with hypertriglyceridemia. Not surprisingly, baseline HDL-C was significantly associated with TG.
Change in HDL-C following fibrate treatment
HDL-C increased significantly (paired t-test, p=0.033) following fibrate treatment by a mean of 0.059 mmol/L in the total patient group (median 0.02 mmol/L, range: −1.0 mmol/L to +1.45 mmol/L). We then carried out separate linear regression analysis with HDL-C change as the outcome (dependent variable) and patient characteristics and pretreatment lipid and creatinine concentrations as independent variables. The results are presented in Table 2, model 1. Duration of treatment, diabetes, and pretreatment HDL-C were significantly associated with change in HDL-C. All three of these factors were entered simultaneously into a multiple regression model with change in HDL-C once again the dependent variable (Table 2, model 2). It appears that all three factors were independently associated with change in HDL-C following fibrate treatment. Examination of the coefficients suggested that lower levels of pretreatment HDL-C (coefficient=−0.32) were associated with greater increases in HDL-C. Patients with diabetes had a significantly different response (coefficient −0.16) to those without diabetes (reference group) with regard HDL-C change. Whereas HDL-C in patients with diabetes decreased by a nonsignificant 0.06 mmol/L (P=0.19, paired t-test), patients without diabetes demonstrated a significant increase in HDL-C of 0.10 mmol/L (P=0.0002, paired t-test) following fibrate treatment. No difference in TG reduction was seen in patients with diabetes (TG decrease of 4.2 mmol/L) and those without diabetes (TG decrease of 4.3 mmol/L). Similarly, there was no significant difference in TG reduction between males (TG decrease 4.7 mmol/L) and females (TG decrease 3.1 mmol/L).
CI, confidence interval; TC, total cholesterol; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol.
Interestingly, baseline TG was not significantly associated with change in HDL-C (Table 2). Change in HDL-C when patients were stratified by baseline TG was as follows: 0.095 mmol/L (quartile 1, TG<3.9), 0.060 mmol/L (quartile 2, TG 3.9–5.3), 0.017 mmol/L (quartile 3, TG 5.4–8.0), and 0.067 mmol/L (quartile 4, TG >8.0). The differences among these four groups were not significant. The change in TG [coefficient=−0.001 (95% CI −0.011–0.008, P=0.75)] was also not significantly associated with change in HDL-C.
We then studied the association between pretreatment HDL-C and change in HDL-C in greater detail. The pretreatment HDL-C was categorized into four groups: HDL-C, <0.8 mmol/L (n=34); HDL-C, 0.8–1.00 mmol/L (n=70); HDL-C, 1.01–1.2 mmol/L (n=38); and HDL-C, >1.2 mmol/L (n=73). The change in HDL-C is presented in Fig. 1. We carried out a multiple regression analysis with change in HDL-C as outcome, and the pretreatment HDL-C categories as a factorized variable. This analysis was corrected for diabetes and duration of fibrate treatment, with both entered into the model as co-variables. Pretreatment HDL-C >1.2 mmol/L was the reference category, and the other pretreatment HDL-C categories were compared to this. It was observed that patients in the HDL-C <0.8 mmol/L [coefficient=0.22 (95% CI 0.090–0.35, P=0.001] and HDL-C 0.8–1.00 mmol/L [coefficient=0.14 (95% CI 0.032–0.24, P=0.011] categories were significantly different to the reference category in relation to the change in HDL-C following treatment. This was not observed in the group with pretreatment HDL-C of 1.01–1.20 mmol/L [coefficient=0.034 (95% CI −0.095–0.1, P=0.60]. To simplify the above finding we stratified the patients into those with HDL-C ≤1.00 mmol/L, and those with HDL-C >1.00 mmol/L (reference group). Patients with HDL-C ≤1.00 had a significantly greater increase in HDL-C following fibrate treatment when compared to the reference group [coefficient=0.15 (95% CI 0.066–0.24, P=0.001]. Similarly, we stratified the patients by pretreatment TG levels and studied the effect on HDL-C change following treatment. Multiple regression analysis showed no significant differences in HDL-C change existed between the TG categories.
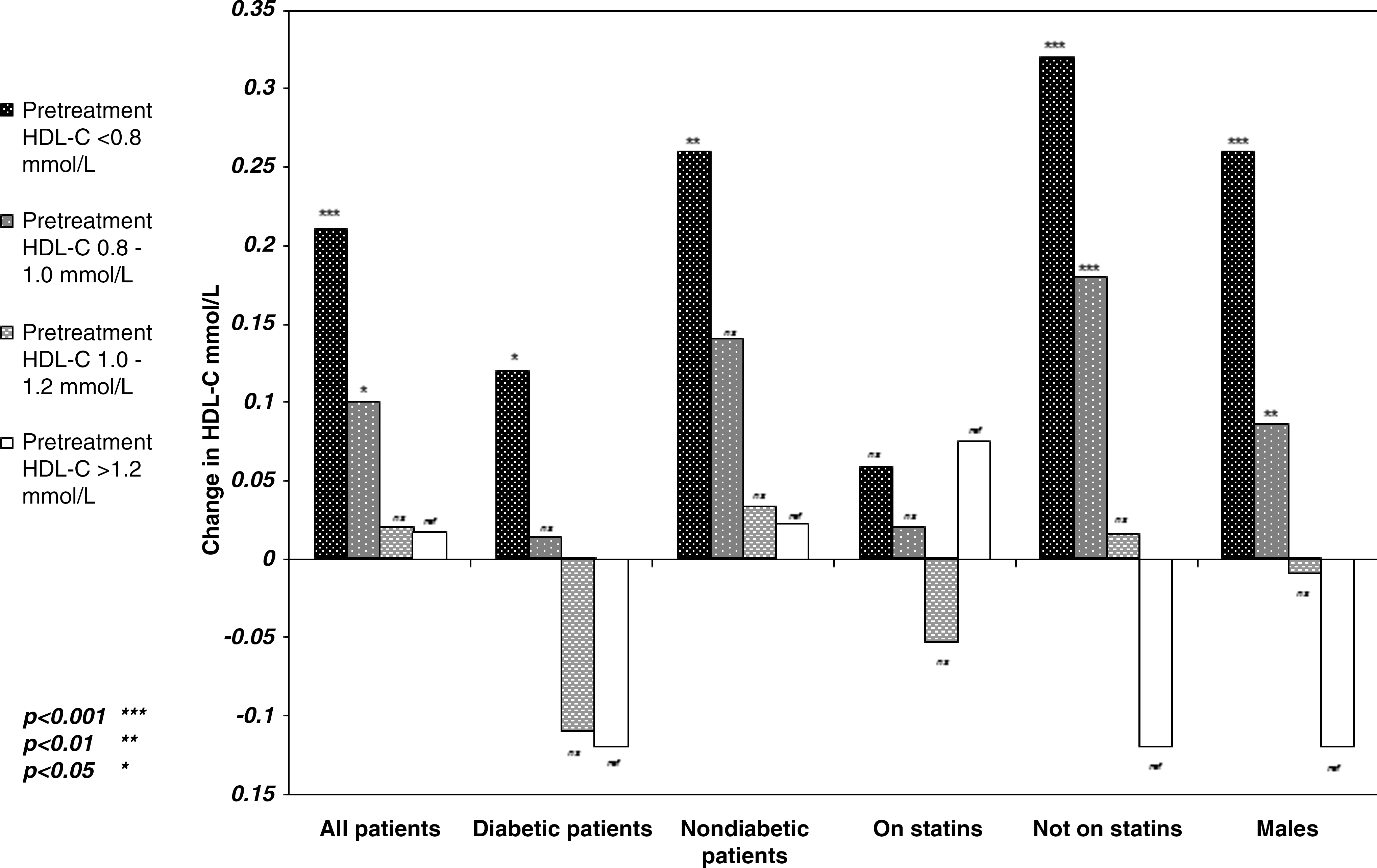
Change in high-density lipoprotein cholesterol (HDL-C) following fibrate treatment with the patient cohort stratified by pretreatment HDL-C concentrations.
Association between change in HDL-C and pretreatment HDL-C values in patient subgroups
Our group of patients consisted of a cohort referred to routine hospital lipid clinics with a range of patient characteristics as seen in Table 1. We stratified our patient groups by some of these characteristics and studied the relationship between pretreatment HDL-C and change in HDL-C in each of these groups. The association between pretreatment HDL-C and change in HDL-C following fibrate treatment was evident in all the subgroups apart from female patients, those on statin treatment, and the 28 patients who were on fibrates other than fenofibrate (Table 3). When the patients were stratified by the specific lipid clinic they attended (GHH, BHH), significant associations between change in HDL-C and pretreatment HDL-C were observed with similar coefficients (GHH, −0.28; BHH, −0.30). Figure 1 presents the change in HDL-C following fibrate treatment in relation to categorized pretreatment HDL-C in the total cohort as previously described and in some of the above-mentioned subgroups. We did not stratify the patients by their baseline TG as this was significantly associated with baseline HDL-C.
A significant association between change in HDL-C and pre-treatment HDL-C was also seen in patients stratified by alcohol intake (0 units/week, 1–28 units/week and >28 units/week), smoking status (never smoked, ex-smoker, and current smoker) and ethnicity (Asian, non-Asian).
CI, confidence interval; GHH, Good Hope Hospital; BHH, Birmingham Heartlands Hospital.
Discussion
The principal aim of this study was to investigate the effect of fibrates, principally fenofibrate, on HDL-C in our routine clinic setting. We then planned to identify factors that may be associated with any change in HDL-C. Overall the HDL-C increased by a mean of 0.059 mmol/L following fibrate therapy. Change in HDL-C was significantly associated with pretreatment HDL-C, diabetes, and duration of treatment. Greater increases in HDL-C were observed in patients with lower levels of pretreatment HDL-C, as previously described by Kornitzer et al. 16 This pattern was observed independently in both clinics run by the trust.
In addition to confirming Kornitzer's observation in a routine clinic setting, we have studied this phenomenon in greater depth. Patients with HDL-C ≤1.0 mmol/L showed significant increase in HDL-C when compared to patients with HDL-C >1.0 mmol/L. The association between change in HDL-C and pretreatment HDL-C was not observed in females, those on statins, and patients on fibrates other than fenofibrate. Females are known to have higher HDL-C compared to males, and this could possibly explain the lack of any observed association. Only 3.45% (n=2) and 24.14% (n=14) of females had pretreatment HDL-C concentrations below 0.8 mmol/L and 1.0 mmol/L, respectively; this in contrast to 10.83% (n=17) and 44.59% (n=70) of males. This distribution, together with the smaller number of females in our study, prohibited us from examining this data in further detail. Once again the number of patients on fibrates other than fenofibrate was too small to allow us to analyze the data further.
In our patients, we unexpectedly observed that fibrate therapy did not increase HDL-C when they were also on statins. In contrast, when fenofibrate was added to simvastatin in the ACCORD study, HDL-C increased by a mean of 8.4%. However, the dose of simvastatin was modified in response to changing guidelines, and similarly the dose of fenofibrate was adjusted depending on the estimated glomerular filtration rate. Furthermore, it must be noted that only 80% of the patients were on simvastatin at the end of the study and an additional 6% of patients were taking an alternative LDL-C–reducing agent. The effect of a statin–fibrate combination in the FIELD study is difficult to interpret due to the imbalanced statin “drop-in.” Statins have also been seen to increase HDL-C. Metaanalysis of the VOYAGER database showed that HDL-C increase following statin treatment was greater in patients with lower pre-statin treatment HDL-C. Although simvastatin, rosuvastatin, and atorvastatin all increased HDL-C, the dose–response effect of atorvastatin on HDL-C change was inverse. 26 However, none of these findings offer an explanation for our observation of insignificant HDL-C change in patients on statins.
There has been considerable speculation as to which group of patients would benefit from fibrate treatment 27 due to mixed outcomes regarding cardiovascular events in the large fibrate trials. However, in subgroups with low HDL-C and raised TG, which are features of the metabolic syndrome, there has been greater cardiovascular benefit when compared to the complementary groups. This has generated significant interest regarding the use of fibrates in such patients. 28 Our data showing that HDL-C increase following fibrate treatment were observed mainly in patients with low baseline HDL-C and may partly explain the greater cardiovascular benefits observed in the metabolic syndrome patient subgroups.
Ours was a retrospective evaluation of the effects of fibrates, mainly fenofibrate, on HDL-C in a routine outpatient setting. There are some weaknesses that are inherent to this type of study. Unlike randomized controlled trials, there was no inclusion or exclusion criteria. Frequency of patient follow-up was based on clinical judgement and not trial protocol, thus there was some missing data. Lack of accurate body mass index (BMI) measurements as recorded in the clinical notes was a further limitation of our study. Despite the above points, it is important that questions we have attempted to address are studied in both controlled and real-world settings.
Our study has presented us with some interesting findings. Whereas it is possible that the effect of baseline HDL-C on the magnitude of HDL-C increase may reflect a regression to the mean, it is important that this be further investigated in appropriately designed studies that should also focus on possible explanatory mechanisms. Furthermore, randomized controlled trials are essential to study the effect of fibrates on cardiovascular outcomes in patients with lower HDL-C than investigated in fibrate trials thus far. This would negate some of the limitations of subgroup analysis of existing studies that we have at present.
Footnotes
Author Disclosure Statement
The authors report no competing interests and other declarations.