
Abstract
Background:
The role of resistin in the pathophysiology of insulin resistance in human is controversial and different in men and women. Thus, the discrepancy among previous reports may be resolved by gender-specific analysis of a large number of participants.
Methods:
From a single community, we recruited 746 men (mean age, 60±14 years) and 1033 women (63±12 years) during their annual health examination. We investigated whether plasma resistin levels are associated with insulin resistance evaluated by homeostasis of model assessment of insulin resistance (HOMA-IR) according to gender.
Results:
Resistin levels were significantly correlated with HOMA-IR in men, but not in women. Analysis of covariance showed that two regression lines were significantly different (F=9.941, P=0.002). Multiple linear regression analyses for resistin showed that the resistin levels (β=0.124, P<0.001) were independently and significantly associated with HOMA-IR as well as body mass index (BMI), alcohol consumption, smoking status, uric acid, γ-glutamyltransferase (GGT), and high molecular weight (HMW) adiponectin only in men and not in women. The interaction between gender and resistin level (F=11.50, P<0.001) was also a significant and independent determinant for HOMA-IR as well as gender, BMI, alcohol consumption, smoking status, uric acid, GGT, HMW adiponectin, and resistin.
Conclusions:
These results suggest that plasma resistin levels are associated with insulin resistance in older Japanese men.
Introduction
The aim of this study was to determine whether plasma resistin levels are associated with insulin resistance according to gender. To determine this, we examined cross-sectional data from Japanese community-dwelling participants.
Methods
Subjects
The present study was designed as a part of the Nomura study. 16 Subjects were selected through a community-based annual check-up process in a rural town located in Ehime prefecture, Japan. Information on medical history, present conditions, and drugs were obtained by interview. Other characteristics, such as smoking, alcohol habit, and medication, were investigated by individual interviews using a structured questionnaire. Subjects taking medications for diabetes, or having fasting plasma glucose (FPG) levels of ≥126 mg/dL were excluded. The sample population comprised 2010 subjects. The final study sample consisted of 1779 subjects (746 men and 1033 women). This study was approved by the ethics committee of Ehime University School of Medicine, and written informed consent was obtained from each subject.
Evaluation of risk factors
Information on demographic characteristics and risk factors was collected using clinical files. Body mass index (BMI) was calculated by dividing weight (in kilograms) by the square of the height (in meters). We measured blood pressure with an appropriately sized cuff on the right upper arm of the subjects in a sedentary position using an automatic oscillometric blood pressure recorder (BP-103i, Colin, Aichi, Japan), while subjects were seated after having rested for at least 5 min. Daily alcohol consumption was measured using the Japanese liquor unit in which a unit corresponds to 22.9 grams of ethanol, and the participants were classified into never drinkers, occasional drinkers (<1 unit/day), and daily drinkers (≥1 unit/day). Smoking status was classified into never smokers, past smokers, and current smokers. Total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), FPG, creatinine (enzymatic method), uric acid, immunoreactive insulin (IRI), high-sensitivity C-reactive protein (hsCRP), γ-glutamyl transferase (GGT), high-molecular weight (HMW) adiponectin, and resistin were measured during fasting. Plasma hsCRP concentration was measured using a Behring BN II nephelometer (Dade Behring Inc., Marburg, Germany), and these inter- and intraassay coefficients of variation were 3.2% and 6.7%, respectively. Serum GGT concentration was assayed with an automatic analyzer (TBA-c6000, TOSHIBA, Tokyo) and this intraassay coefficient of variation was 0.87% to 2.11%. Plasma HMW adiponectin was determined using a recently developed enzyme-linked immunosorbent assay (ELISA) system (FUJIREBIO, Tokyo, Japan). 17 This assay system uses a monoclonal antibody against HMW adiponectin; the specificity of this antibody has been described elsewhere. 18 The inter- and intraassay coefficients of variation of the adiponectin assay at various substance concentrations were 2.1%–7.3% and 6.3%–7.2%, respectively. Plasma resistin was measured using a human resistin ELISA kit (LINCO Research) following the manufacturer's protocol as described. 19 These inter- and intraassay coefficients of variation were 1.7%–6.9% and 7.2%–8.1%, respectively. Low-density lipoprotein cholesterol (LDL-C) levels were calculated by the Friedewald formula. 20 Participants with TG levels ≥400 mg/dL were excluded. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated from FPG and IRI levels using the following formula: [FPG (mg/dL)×IRI (mU/mL)]/405. 21
Statistical analysis
Data are presented as the mean±standard deviation (SD) unless otherwise specified, and in the cases of parameters with nonnormal distributions (TG, IRI, FPG, hsCRP, GGT, HMW adiponectin, resistin, and HOMA-IR) the data are shown as median (interquartile range [IQR]) values. In all analyses, parameters with nonnormal distributions were used after log-transformation. As several background differences between men and women were demonstrated by previous studies, 22,23 the statistical analysis was performed according to gender using PASW Statistics 17.0 (Statistical Package for Social Science Japan, Inc., Tokyo, Japan). Differences among groups were analyzed by analysis of variance (ANOVA) for continuous variables or the chi-squared test for categorical variables. Correlations between various characteristics and HOMA-IR were determined using the Pearson's correlation coefficient. Multiple logistic regression analysis was used to evaluate the contribution of the confounding factors for HOMA-IR. The synergistic effect of resistin and gender was evaluated using a general linear model adjusted for the following parameters: Age, BMI, smoking status, alcohol consumption, uric acid, hsCRP, GGT, and HMW adiponectin. A P value<0.05 was considered significant.
Results
Characteristics of subjects categorized by gender
The characteristics of the subjects categorized according to gender are illustrated in Table 1. The study included 746 men (60±14 years) and 1033 women (63±12 years). Prevalence of smoker, alcohol consumption, and history of cardiovascular disease (CVD), diastolic blood pressure (DBP), TG, FPG, uric acid, hsCRP, and GGT were significantly higher in men than in women, but age, LDL-C, HDL-C, and prevalence of antilipidemic medication, HMW adiponectin, and resistin were significantly lower. There were no intergroup differences regarding BMI, systolic blood pressure (SBP), and prevalence of antihypertensive medication.
Data presented are the mean±standard deviation (interquartile range). Data for triglycerides, fasting plasma glucose, hsCRP, GGT, HMW adiponectin, and resistin were skewed and are presented as median (interquartile range) values, and were log-transformed for analysis.
P value from analysis of variance (ANOVA) for continuous variables or from the chi-squared test for categorical variables.
Body mass index was calculated using weight in kilograms divided by the square of the height in meters.
Alcohol consumption [nondrinkers, occasional drinkers (1–6 days/week), and daily drinkers (≥7 days/week)].
Smoking status [never smokers, past smokers, light smokers (<30 packs/year) and heavy smokers (≥30 pack/year)].
LDL, low-density lipoprotein; HDL, high-density lipoprotein; hsCRP, high sensitivity C-reactive protein; GGT, γ-glutamyl transferase; HMW, high molecular weight.
Relationship between various confounding factors and insulin resistance of subjects categorized by gender
Table 2 shows the relationship between participant characteristics and HOMA-IR of the subjects categorized by gender. The Pearson's correlation coefficient showed that HOMA-IR levels were significantly correlated with age, BMI, SBP, DBP, prevalence of antihypertensive medication, TG, LDL-C, HDL-C, uric acid, hsCRP, and HMW adiponectin in both genders, while correlated with alcohol consumption and resistin only in men and prevalence of antilipidemic medication only in women.
r, Pearson's coefficient correlation.
Homeostasis of minimal assessment of insulin resistance (HOMA-IR) was calculated using the following formula: Fasting blood glucose [(mg/dL)×IRI (mU/mL)]/405. Data for HOMA-IR, triglycerides, fasting plasma glucose, hsCRP, GGT, HMW adiponectin, and resistin were skewed, and were log-transformed for analysis.
HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; GGT, γ-glutamyl transferase; HMW, high-molecular-weight; IRI, immunoreactive insulin.
Correlation between resistin and HOMA-IR of subjects categorized by gender
As shown in Fig. 1, resistin levels were significantly correlated with HOMA-IR in men, but not in women. Analysis of covariance showed that two regression lines were significantly different (F=9.941, P=0.002).
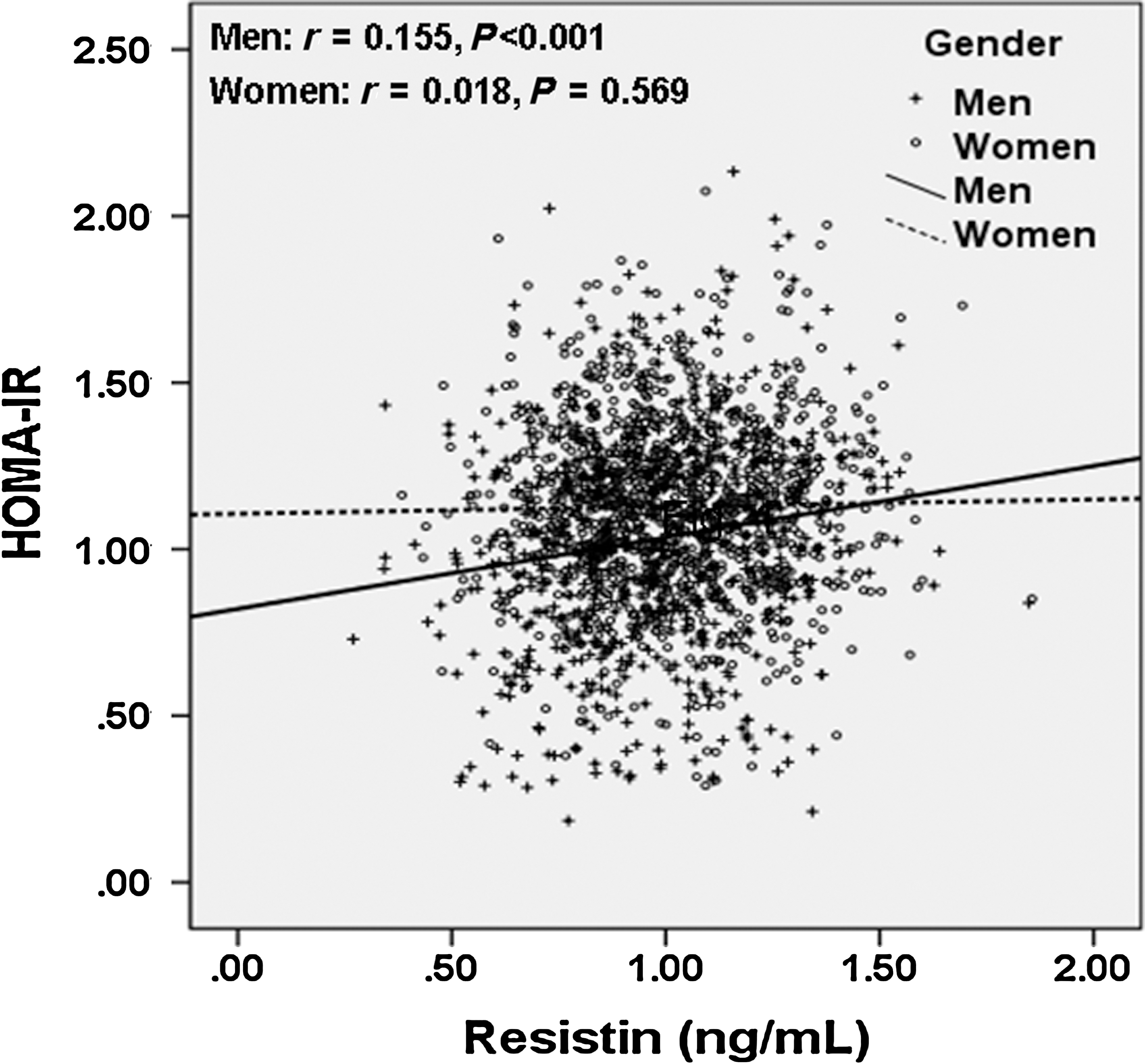
Correlation between resistin and homeostasis model assessment of insulin resistance (HOMA-IR) of subjects categorized by gender. Data for resistin and HOMA-IR were skewed and log-transformed for analysis. The lines of best fit (men, n=746, r=0.155, P<0.001; women, n=1033, r=0.018, P=0.569) are indicated. Analysis of covariance showed that two regression lines were significantly different (F=9.941, P=0.002).
Stepwise multiple linear regression analysis of the correlation between various confounding factors and HOMA-IR of subjects categorized by gender
To further investigate whether resistin levels can explain HOMA-IR levels independent of other known confounding factors, multiple linear regression analyses for resistin were performed by gender. In men, resistin levels were independently and significantly associated with HOMA-IR as well as BMI, alcohol consumption, smoking status, uric acid, GGT, and HMW adiponectin. In women, age, BMI, GGT, and HMW adiponectin were significantly associated with HOMA-IR, whereas resistin levels were not associated with HOMA-IR Table 3.
R2, Multiple coefficient of determination; β, standard regression coefficient.
HOMA-IR was calculated using the following formula; fasting blood glucose [(mg/dL)×immunoreactive insulin (mU/mL)]/405.
Data for HOMA-IR, hsCRP, GGT, HMW adiponectin, and resistin were skewed, and were log-transformed for analysis.
HOMA-IR, homeostasis model assessment of insulin resistance; hsCRP, high-sensitivity C-reactive protein; GGT, γ-glutamyl transferase; HMW, high-molecular-weight.
Interaction between gender and resistin for insulin resistance
In addition to their direct associations, we observed an interaction between gender and resistin levels for HOMA-IR (Table 4). We assessed the statistical significance of the interaction using a general linear model with the following confounding factors: Age, gender, BMI, alcohol consumption, smoking status, uric acid, hsCRP, GGT, HMW adiponectin, resistin, and the interaction between gender and resistin (Table 4). The interaction between gender and resistin was also a significant and independent determinant for HOMA-IR as well as gender, BMI, alcohol consumption, smoking status, uric acid, GGT, HMA adiponectin, and resistin.
The net effect of each interaction was estimated using a general linear model.
HOMA-IR, homeostasis model assessment of insulin resistance; hsCRP, high-sensitivity C-reactive protein; GGT, γ-glutamyl transferase; HMW, high-molecular-weight.
Discussion
In 1779 community-dwelling subjects, we showed that plasma resistin was an independent factor for HOMA-IR as well as BMI, alcohol consumption, smoking status, uric acid, GGT, and HMW adiponectin only in men and not in women. In addition, we demonstrated that there is an interaction between gender and resistin for HOMA-IR. To our knowledge, this is the first study to indicate these associations of gender and resistin with insulin resistance in about 2000 community-dwelling subjects.
The role of resistin in insulin resistance is controversial. In cross-sectional studies involving 123 middle-aged women and 120 healthy young subjects, Lee et al. 12 demonstrated that serum resistin levels were not associated with insulin resistance as well as markers of obesity, central adiposity, hyperlipidemia, leptin, or sex hormones. Some studies demonstrate that serum resistin levels are increased in patients with type 2 diabetes, but this increase is not linked to markers of insulin resistance or adiposity. 24,25 In Pima Indians, like other human populations, circulating resistin levels are related to the degree of adiposity, but not to insulin resistance. 13 Other studies also showed a relationship that was attenuated by adjusting for BMI or adiposity. 26,27 These studies involved small numbers of participants. In contrast, our findings are in accordance with some studies that show a significant relationship between resistin and HOMA-IR. 4,8 In a previous large population study, we 7 and Hivert et al. 8 have reported that plasma resistin levels are associated with age, gender, SBP, HDL-C, TG, PFG, IRI, and inflammatory markers (i.e., hsCRP), and are significantly associated with insulin resistance independent of age, gender, and BMI. Moreover, in this study, we demonstrated that a positive and independent association between plasma resistin and insulin resistance presented in men only.
The mechanisms underlying the reason by which resistin reflects a risk for HOMA-IR are not completely understood. However, systemic inflammation is closely involved in the pathogenesis of insulin resistance, and thus, increased resistin may also reflect inflammation and insulin resistance. In adipose tissue, tissue macrophages appear to be responsible for resistin expression. 28 Resistin is another protein believed to be involved in the inflammatory response, and it was related to hsCRP in our study (data not shown). Stumvull and Häring 29 proposed that resistin is one of these macrophage-derived factors in obesity that might induce insulin resistance under subclinical inflammatory states. The recent report that administration of recombinant resistin modulates hepatic glucose production in the rat 30,31 supports the original observation that resistin has a role in modulating insulin resistance. Majaj et al. also showed that pioglitazone treatment in type 2 diabetes causes a significant decrease in plasma resistin concentration, and the decrease in plasma resistin is positively correlated with the decrease in hepatic fat content and improvement in hepatic insulin sensitivity. 32
The mechanisms by which gender (i.e., men) and resistin synergistically reflect the risk for HOMA-IR have not been noted. Plasma resistin was related to fat mass in young, healthy participants, and this was more significant in women than in men. 33 Men are more likely to have fat stored around the abdomen due to gender-related hormone differences. 34 In women, the female sex hormone (i.e., estrogen) causes fat to be stored in the buttocks, thighs, and hips. 34 However, when women reach menopause and the estrogen produced by ovaries declines, fat migrates from the buttocks, hips, and thighs to the abdomen. 35 Resistin expression is higher in omental and abdominal subcutaneous white fat than in adipose tissue from the thigh or breast. 36 Several studies show that visceral fat is more strongly correlated with risk factors such as insulin resistance. 37 Thus, we could assume that the gender-specific effect of resistin could depend on various adipose tissue depositions that induce resistin production in men or women. In our study, many of women were postmenopausal, and the women were older than the men; however, resistin was significantly associated with insulin resistance in men, but not in women. This correlation remained highly significant, even after correcting for confounding factors (i.e., age and BMI).
There are some limitations to this study. First, our cross-sectional study design does not eliminate a potential causal relationships between plasma resistin levels and insulin resistance in Japanese community-dwelling men only. Second, resistin levels, FPG, and plasma insulin are based on a single assessment of blood, which may introduce a misclassification bias. Third, we could not eliminate the possible effects of underlying diseases on the results. We also could not eliminate the possible effects of medications for hypertension and dyslipidemia on the present findings. Fourth, HOMA-IR is less accurate and precise than the glucose clamp in measuring insulin resistance, but this limitation is mitigated when the number of subjects examined is large, as in our study. 38 Therefore the demographics and referral source may limit generalizability.
Conclusion
The present study showed that resistin levels are strongly associated with HOMA-IR in older Japanese men from a rural village. The underlying mechanism behind this relationship is unclear, but it seems to be independent of traditional cardiovascular risk factors such as age, gender, BMI, alcohol consumption, smoking status, uric acid, hsCRP, GGT, and HMW adiponectin. For community-dwelling healthy men, prospective population-based studies are needed to investigate the mechanisms underlying this association.
Footnotes
Acknowledgments
We thank Haruhiko Osawa, Department of Molecular and Genetic Medicine, Ehime University Graduate School of Medicine, who offered us data regarding resistin levels. This work was supported in part by a grant-in-aid for Scientific Research from the Foundation for Development of Community (2011).
Author Disclosure Statement
The authors declare that they have no competing interests.